


Abstract
Stage-adapted treatment in oncology relies on correct tumor staging for patients with malignant diseases. To ensure accurate assessment of the tumor stage in thoracic and abdominal diseases by PET/CT, both CT and PET need to be optimized. In this setting, different malignant diseases require customized imaging protocols. Although in the clinical setting of therapy assessment, PET/CT with integration of low-dose, nonenhanced CT may be sufficient, tumor staging may require a more sophisticated CT protocol. This review focuses on potential CT protocols for imaging cancers of the chest and abdomen. Examples of CT protocols are presented and discussed for non–small cell lung cancer, breast cancer, colorectal cancer, gastrointestinal stromal tumors, and interventional liver therapy.
Stage-adapted treatment in oncology relies on correct tumor staging for patients with malignant diseases. Since the introduction of CT more than 25 y ago, this radiologic procedure has become widely used and can be considered the imaging modality of choice for many tumor entities. Not only CT but also all morphologic imaging modalities, including ultrasound, conventional radiography, and MRI, share the same mechanism for detecting malignant diseases. The main principle of these imaging procedures is the identification of morphologic tissue alterations caused by the underlying malignancy. CT depicts changes in tissue attenuation measured in Hounsfield units (HU). These attenuation differences may show as either hypodense or hyperdense areas representing focal lesions in parenchymal organs, in bone, or in enlarged lymph nodes.
Early generations of CT scanners were capable of sequential scanning only. As a result, small lesions could be missed because of partial-volume effects or patient movement during the examination. These limitations applied to the chest and upper abdomen in particular. Additionally, lengthy examination times allowed for only a single phase of intravascular contrast enhancement; multiphase examinations were not possible. The next generation of CT scanners allowed for helical scanning with faster protocols, which enabled volumetric data acquisition and larger scan volumes. The development of multislice CT, which currently accumulates data with up to 64 detector rows, led to 3-dimensional imaging with isotropic voxels, perfusion imaging of whole organs, and cardiac imaging. During this process of development, CT became preferable to MRI because CT is easier to perform, faster, and less expensive.
In daily clinical routine, every clinical question mandates a tailored CT protocol that defines the scan direction, the collimation, the field of view, the potential administration of intravenous or oral contrast material, and the use of dedicated breathing instructions. This review focuses on CT protocols for PET/CT of tumors of the chest and abdomen.
DEFINING DIAGNOSTIC CT
From the radiologist's point of view, fully diagnostic CT requires the following: sufficient spatial resolution with an acceptable signal-to-noise ratio, the administration of an appropriate amount of oral or intravenous contrast material if there are no contraindications, and a radiation dose as low as reasonably achievable to allow diagnostic information to be obtained (requires tube current modulation).
Sufficient spatial resolution with an acceptable signal-to-noise ratio mandates the use of appropriate detector collimation. Given the fact that most PET/CT scanners currently in use are equipped with at least 2 or 4 detector rows, the chosen detector collimation should be as large as possible (1.5–2.5 mm) to enable the acquisition of a whole-body scan in a reasonable time frame (<60 s). Nevertheless, the collimation should not exceed 2.5 mm to enable the reconstruction of datasets at 2.5-mm increments suitable for 3-dimensional postprocessing.
Lesion detection by CT is based on attenuation differences between the lesion and its surrounding structures. Most parenchymal organs and most pathologic conditions are characterized by attenuation values of 30–80 HU. Thus, on nonenhanced CT datasets, tumor detection can be compromised because of similar attenuation values for the lesion and its harboring organ. To overcome this limitation, contrast agents have been introduced to CT. On the basis of long experience with contrast-enhanced CT in the imaging of oncology patients (1,2), the use of intravenous or oral contrast material also may be of benefit for PET/CT in many situations. The advantages include the detection of additional lesions with no or only minor tracer uptake, the characterization of focal lesions on the basis of specific contrast material dynamics, and the more accurate localization of small lesions in the vicinity of blood vessels, the intestine, or parenchymal structures (3). However, the use of intravenous contrast material in PET/CT is rather controversial. Some studies have indicated an overestimation of the standardized uptake value (SUV) in the presence of CT contrast material after CT-based attenuation correction of PET data (4,5). The magnitude of SUV overestimation attributable to intravenous contrast material depends on the density of the administered contrast material (5). Only small differences in SUVs have been found in comparisons of nonenhanced and enhanced CT data (6). In clinical practice, the effect of intravenous contrast material on attenuation correction tends to be negligible and makes the routine use of intravenous contrast material in PET/CT practical (7).
A way to minimize potential PET artifacts is to tailor the contrast material administration protocol to the needs of the PET/CT scan. This can be achieved by modifying the CT scan direction from craniocaudal to caudocranial and adjusting the phasing and timing of the contrast material injection (5). The most important issue in adapting the CT protocol to the needs of PET/CT is to avoid contrast material–associated artifacts caused by a contrast bolus in thoracic veins. This goal can be properly achieved by scanning caudocranially rather than craniocaudally. Another method for avoiding a CT contrast bolus is to use a saline chaser immediately after the contrast material injection. Of course, the contrast agent administration needs to be adjusted to the CT scanner specifications, such as the tube heat capacity, rotation time, and number of detector rows. Therefore, a higher tube heat capacity and a shorter rotation time allow for faster scanning of a given extended imaging range in the z-axis. Like scanning protocols for CT alone, protocols with intravenous contrast material in PET/CT will have to be modified continuously as new scanners become available (8,9). It is important to state that patients who have recently undergone contrast-enhanced CT before being referred for PET/CT may not need additional contrast-enhanced PET/CT if the previous dataset is available for image correlation.
The radiation dose must be considered an issue in CT. Except for indications such as tumor screening, CT alone is usually performed in a full-dose manner, especially for tumor staging. When integrating full-dose CT in PET/CT, the radiation dose from CT may amount to approximately 15–20 mSv for a scan from the head to the upper thighs. Therefore, the major portion of radiation exposure in PET/CT can be attributed to the CT component in such an imaging scenario (10). If CT is performed in a low-dose manner, the radiation burden can be reduced 5-fold to 3–4 mSv. A low-dose CT component may be used for attenuation correction and anatomic localization of focal tracer uptake in PET. However, there is ongoing debate as to how much additional information may be derived from low-dose CT compared with full-dose CT as part of PET/CT (11,12). On the one hand, low signal-to-noise ratios and streak artifacts may limit the diagnostic value of low-dose CT; on the other hand, diagnostic CT may not be required in all PET/CT examinations. In younger patients with a potentially curative malignant disease, radiation exposure must be considered an issue. Furthermore, assessment of the response of a tumor to therapy is mainly based on functional data rather than morphology. In this situation, low-dose, nonenhanced CT will be sufficient. Thus, the decision as to how much CT is required in PET/CT should be based on the PET/CT indication rather than on a rigid concept influenced by the pride of place.
PROTOCOL CONSIDERATIONS FOR TUMOR STAGING
For the staging of tumors of the chest and abdomen, all potential sites of metastases need to be evaluated. Therefore, whole-body coverage is needed. On the basis of scanner limitations, whole-body PET/CT was initially performed in a “non-whole-body” manner, covering the head and neck, the chest, the abdomen, the pelvis, and the upper thighs. The lower legs were scanned only in specific situations. Modern PET/CT scanners have an axial field of view of more than 2 m, offering a “real” whole-body scan from head to toe without patient repositioning. However, even today, most PET/CT examinations are performed from the head to the upper thighs to reduce examination times under those of a real whole-body protocol.
The current standard protocol used for whole-body PET/CT at our institution with a PET/CT scanner with dual-slice helical CT (Biograph Duo; Siemens Medical Solutions) is shown in Table 1. The CT protocol was adjusted to meet the needs of the PET scan by maintaining the capability to perform diagnostic CT. This protocol includes the use of negative oral contrast material (13), iodinated intravenous contrast material (14), a breathing protocol to reduce breathing artifacts, and an adequate tube current.
Whole-Body PET/CT Protocol
In patients with tumors of the chest and abdomen, we normally limit our whole-body scan to an examination of the base of the skull, neck, chest, and abdomen down to the upper thighs. In patients with malignant melanoma or peripheral sarcoma, the upper extremities and lower extremities are included in the scan, but at the cost of an increase in examination time. The arms and hands can be examined positioned above the head by extending the CT scan cranially. Fixation of the arms and patient cooperation are required to avoid motion artifacts. Positioning aids such as foam molds or vacuum-lock bags are used in addition to the standard arm rest to ensure less patient motion and better image coregistration (Fig. 1) (15).
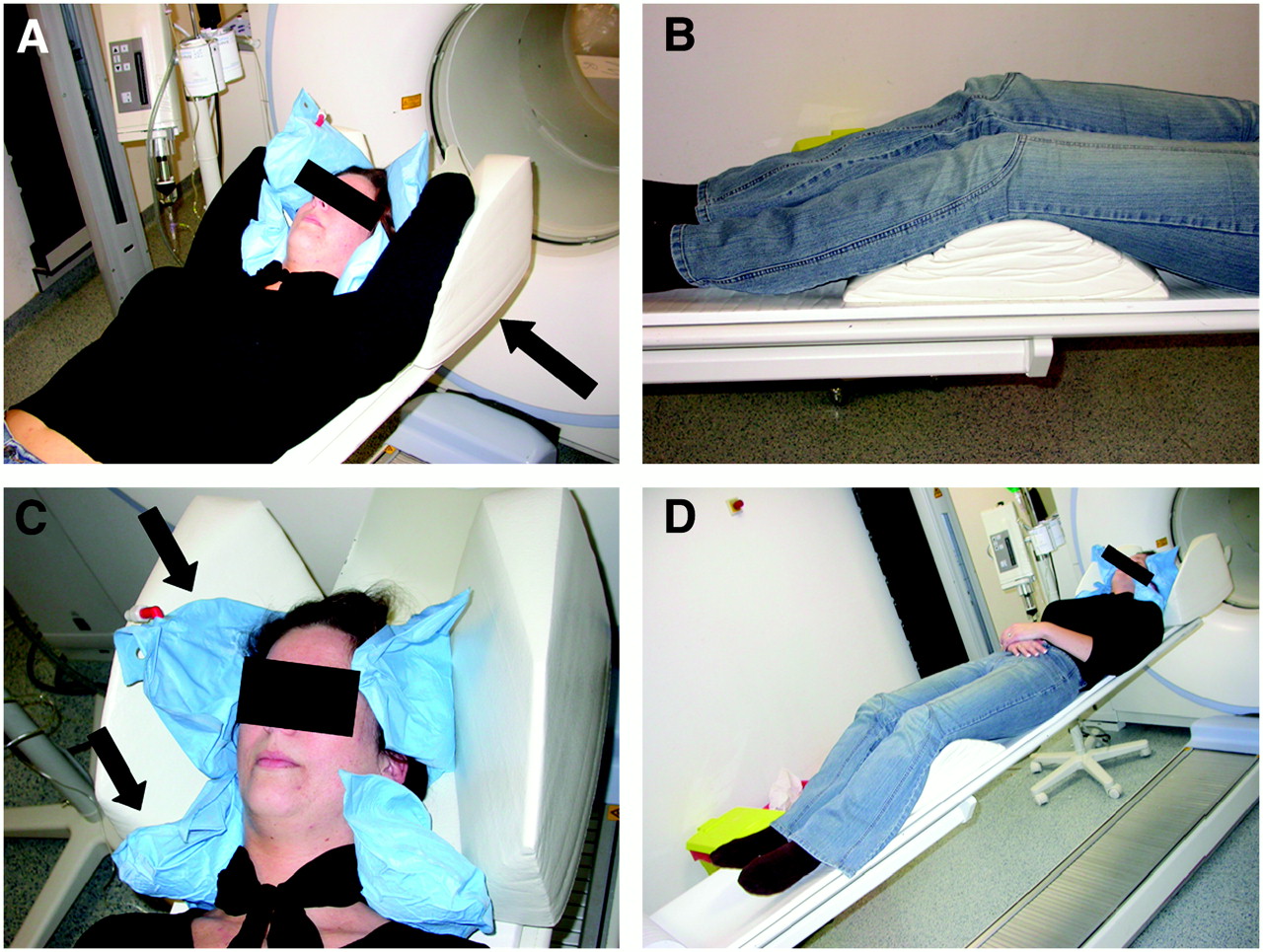
Patient supported with different positioning aids on PET/CT table. (A) For whole-body PET/CT, arms are raised above head and supported by foam cushion to avoid truncation artifacts during scanning of thorax and abdomen (arrow). Furthermore, head is placed within foam cushion and may be additionally supported with vacuum-lock bag to prevent head motion (blue vacuum-lock bag). (B) Legs are supported by another foam mold to inflect patient's knees and to ensure comfortable positioning during scanning. (C) For head and neck scanning, vacuum-lock bag is deflated to fix head and neck within foam cushion (arrows). Thus, possible moving artifacts can be avoided. (D) Additionally, arms are placed on or beside patient's trunk to avoid truncation artifacts in head and neck area.
The examination of the lower limbs requires an additional examination after repositioning of the patient. For scanning of the patient from head to toe, we use a divided protocol, starting with a whole-body scan including the arms and the head in the supine, head-first position. After that, the patient is repositioned in the supine, feet-first position. Both scans are performed with intravenous contrast material and a small overlap in the groin (Table 2). Like the 2 whole-body protocols (Tables 1 and 2), all other protocols listed in Tables 3–7⇓⇓⇓ have been optimized for dual-slice CT.
Whole-Body PET/CT with Examination of Lower Limbs
Whole-Body PET/CT with Additional Low-Dose CT of Chest
Combined Head–Neck and Whole-Body Protocol
Whole-Body PET/CT for Optimized Breast Scanning
PET/CT Colonography Protocol
Multiphase Scan of Liver
PROTOCOL CONSIDERATIONS FOR THERAPY ASSESSMENT
In contrast to whole-body PET/CT tumor staging, the use of low-dose, nonenhanced CT for attenuation correction can be recommended in most cases when PET/CT is performed for the follow-up of patients who have thoracic and abdominal tumors and who are undergoing therapy. This approach seems feasible because the functional parameter of glucose metabolism is far more sensitive than morphologic measurements for assessing treatment response. We do, however, recommend initial full-dose, contrast-enhanced PET/CT with an adequate tube current for staging before the start of therapy to ensure detection and accurate localization of all lesions. Especially with the use of nephrotoxic chemotherapy (i.e., cisplatin and mitomycin), the aspect of renal protection is of clinical importance and further supports the use of nonenhanced CT.
IS THERE A NEED FOR PET/CT OF BRAIN?
There are protocols including the brain (16) in the field of view as well as protocols starting the scan at the base of the skull (14). 18F-FDG is the PET tracer most often used in oncologic staging. On the basis of the inherent tracer characteristics of 18F-FDG, physiologic uptake within the brain is strong. Therefore, small brain metastases may be difficult to detect by 18F-FDG PET. PET/CT can increase the sensitivity over that of PET alone for the detection of small brain metastases if performed in a full-dose manner and with contrast agents. However, the detection of brain metastases by CT alone is usually performed with a delay of approximately 10 min after contrast medium injection to allow for high lesion-to-background contrast. In addition, a higher tube current is required for this scenario than for a normal whole-body PET/CT scan to provide a sufficient contrast-to-noise ratio in the brain, because the contrast-to-noise ratio is typically reduced by the skull with a lower tube current. Neither a long delay of approximately 10 min nor a higher tube current is currently implemented in any whole-body protocol. An additional PET/CT scan of the brain after a whole-body protocol may be another option. However, even contrast-enhanced CT of the brain has been found to be less sensitive than contrast-enhanced MRI (17) for detecting cerebral lesions; therefore, an additional MRI scan of the brain may be the best solution if brain metastases are suspected. Nevertheless, elective inclusion of the brain in whole-body PET examinations has been recommended, depending on the clinical context (18). The inclusion of the brain in the field of view of whole-body PET/CT should be based on the individual patient history, the known extent of malignant disease, and clinical findings.
ADDITIONAL LOW-DOSE CT FOR DETECTION OF PULMONARY NODULES
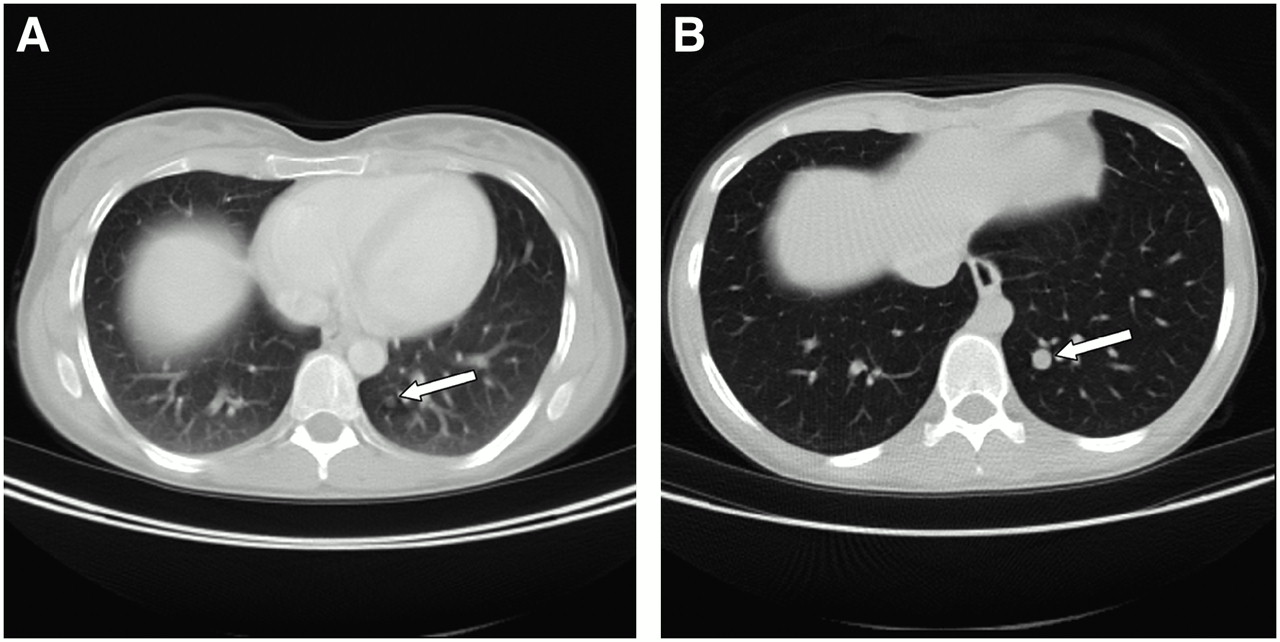
The detection of small pulmonary nodules and the correct classification as either benign or malignant must still be considered a challenge for whole-body 18F-FDG PET/CT. PET regularly misses these small lesions because of its limited spatial resolution and the fact that small hypermetabolic nodules may not be identified because of constant movement of the lungs during the emission time per bed position. If CT is performed during shallow breathing, breathing artifacts may hamper lesion detection by CT. The use of an additional low-dose CT scan during maximal inspiration after a PET/CT scan may be advantageous (19), because it allows for better delineation of small perivascular lesions, especially in the lower lungs (Fig. 2). In this context, we currently perform an additional 40-mA low-dose CT examination during inspiration after a PET/CT examination (Table 3). The number of pulmonary lesions detected is increased with this protocol. However, just as with stand-alone CT, the differentiation of a granuloma from a metastasis is considered difficult in most cases. Thus, further radiologic follow-up of these small, 18F-FDG PET–negative CT-positive lesions is required. In radiology, low-dose CT is widely used as a tool for lung cancer screening. There is evidence that CT detects earlier-stage and smaller lung cancers with higher sensitivities than other screening methods, such as conventional chest radiography. However, so far there is no consensus about the use of low-dose CT as a screening tool. Up to now, no CT screening trial has been able to demonstrate a reduction in lung cancer mortality (20). An important issue in the use of CT for tumor screening is the additional radiation exposure, resulting in an increased risk for lung tumors even with low-dose protocols (21). Therefore, a reduction in the tube current to the lowest reasonable level of milliamperes is necessary for performing an additional CT scan of the chest. A reduction in the tube current to 60 mA was found to result in satisfactory quality of the chest CT images (22). In the thorax, a further reduction in the tube current to 40 mA may yield satisfactory image quality and reduce the overall radiation exposure (23).
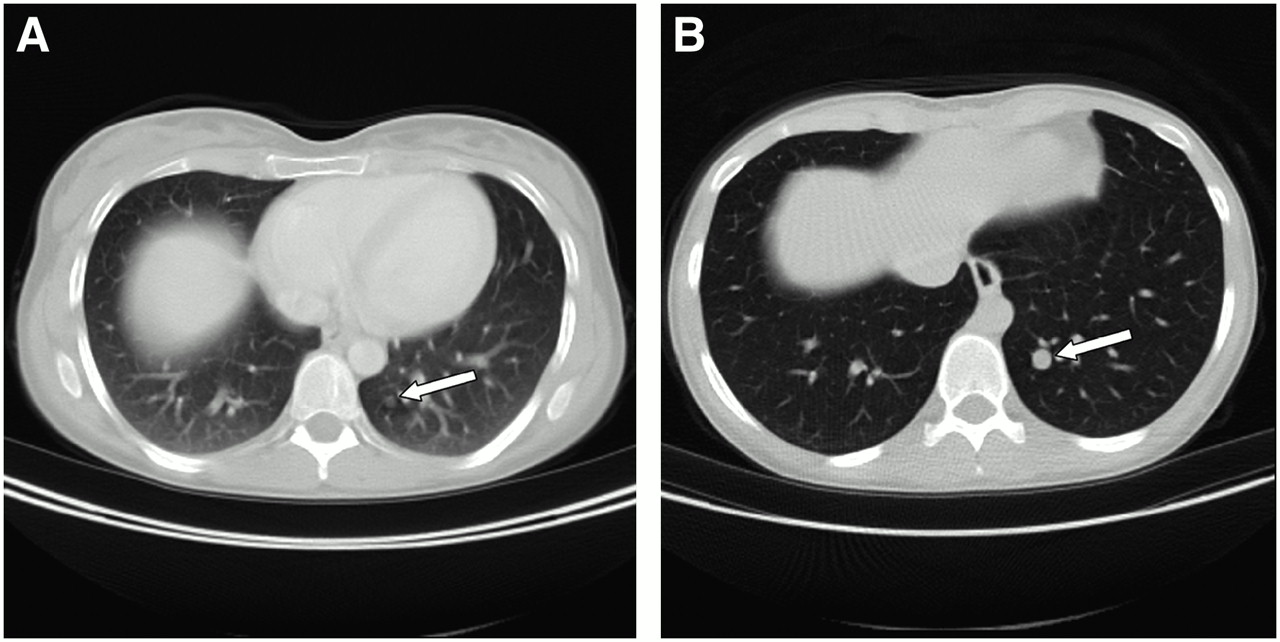
Comparison of chest scanning during shallow breathing (A) and chest scanning with additional low-dose CT during maximal inspiration (B). (A) Lung metastasis from colorectal cancer is only barely visible during shallow breathing (arrow). Also note blurred lung vessels and congested lung parenchyma in this image. (B) Metastasis can be clearly detected by low-dose CT during maximal inspiration (arrow). Additionally, lung parenchyma is well inflated, and lung vessels are displayed sharply.
BREATHING PROTOCOL FOR WHOLE-BODY PET/CT
The need for a special breathing protocol for CT acquisition depends on the body region evaluated. When only areas away from the diaphragm are scanned, the patient can breathe shallowly during CT. Continuous shallow breathing may also be used for CT acquisition as part of a whole-body PET/CT scan; however, image coregistration has been found to be most accurate if the CT scan is acquired during normal expiration (24). Thus, whole-body staging of tumors of the chest and abdomen with PET/CT benefits from a CT breath-hold protocol (25,26). An optimal protocol would include CT data acquired for the whole body during normal expiration, but this goal may be difficult to achieve with CT scanners that have fewer than 64 detector rows. Even with 64-slice scanners, such a protocol may not be feasible in uncooperative or severely sick patients. A compromise is to ask the patient to hold his or her breath during normal expiration for the time that is needed to scan the upper abdomen (liver and spleen) and lower lungs. The required scan time is typically less than 20 s.
IS IT NECESSARY TO ADJUST CT PARAMETERS TO NUMBER OF CT SCANNER DETECTOR ROWS?
The number of detector rows in a helical CT scanner correlates with the temporal and spatial resolutions of the acquired CT dataset. The high temporal resolution of multidetector scanners, which is based on a short tube rotation time and a large number of detector rows, allows for either functional scanning or scans of large body areas along the z-axis. Depending on the time required for a specific CT examination in a whole-body scan, the user needs to adjust the breathing protocol. If the scanner characteristics enable a whole-body CT scan in 20 s or less, then the whole body can be examined in 1 normal expiration breath-hold (27). Otherwise, a breath-hold protocol seems desirable. Furthermore, if CT contrast is desired, then the contrast agent administration protocol needs to be adjusted to the imaging system to avoid artifacts attributable to highly concentrated intravenous contrast material in the central thoracic veins. The contrast agent administration protocol needs to be timed appropriately to ensure that the contrast bolus has passed the thoracic veins when the CT spiral reaches the thorax. This goal can be achieved by fast contrast injection, by the use of a dual-lumen injector with a saline flush, and by scanning caudocranially rather than craniocaudally (17). In addition, the delay between the start of the intravenous contrast agent administration and the start of the CT scan must be tailored to the clinical question. For most tumor entities, a portal–venous phase of the liver will be the appropriate enhancement, whereas for hepatocellular carcinoma (HCC) or neuroendocrine tumors, an arterial phase will be preferable.
IMAGING CANCER OF CHEST AND ABDOMEN
Non–Small Cell Lung Cancer (NSCLC)
Lung cancer is currently the leading cause of cancer deaths in both men and women in the Western Hemisphere (28). Much worse, the expected 5-y survival rate for all patients is 15%; in contrast, the survival rates are 61% for patients with colon cancer, 86% for those with breast cancer, and 96% for those with prostate cancer (29). Accurate definition of the tumor stage is desirable in each patient to provide the best available therapy according to the given extent of the disease. Several studies in the literature have reported a benefit of PET/CT for staging of and therapy response monitoring for NSCLC (30–32). Given the different treatment options and problems connected with the stage of NSCLC, investigators face many challenges in the use of PET/CT for primary staging, treatment planning, therapy response monitoring, and follow-up.
Initial Staging of NSCLC.
18F-FDG PET is recommended in the official American College of Chest Physicians guidelines for noninvasive staging (33) because of the limited value of chest CT in identifying malignant disease in mediastinal lymph nodes. Because 18F-FDG PET/CT has been found to be significantly more accurate in pretherapeutic staging (34), the use of PET/CT for the initial staging of NSCLC is more than justified. The PET/CT staging protocol should include the chest and abdomen for local staging and identification of distant metastases. In addition, the neck should be included in the field of view to stage spread to supraclavicular lymph nodes. Inclusion of the brain to stage potential cerebral metastases may be desired. Thus, a whole-body PET/CT protocol must be considered mandatory for initial tumor staging. We use the protocol listed in Table 1 for the initial staging of NSCLC. When cervical metastases are suspected, small lymph node metastases may be better visualized by decreasing the slice thickness of the CT component to 3 mm. Separate scanning of the head and neck with a collimation lower than that used for the rest of the body may be used in this situation (Table 4). In some instances, a lower CT collimation may also be of benefit for staging of spread to mediastinal lymph nodes. Intravenous contrast material helps to better delineate potential lymph node metastases from adjacent vascular structures in the pulmonary hilum and mediastinum and offers more accurate assessment of tumor infiltration into mediastinal structures. Therefore, contrast-enhanced CT is used for initial tumor staging at our institution. The use of a breathing protocol to minimize coregistration artifacts is recommended.
Treatment Planning for NSCLC Therapy.
In PET/CT examinations used for radiotherapy treatment planning, the positioning of the patient is of utmost importance. The normal examination table should be replaced with a table dedicated for radiotherapy purposes. This table allows for additional fixation with radiotherapy masks or positioning aids. In addition, external fiducial CT markers, if necessary even with small tracer probes, are helpful. To overcome the problem of breathing artifacts, the protocol for radiation treatment planning can be changed to a divided protocol, as follows. The patient is placed on the flat table, and the whole-body scan starts with a dedicated neck and chest scan during a midexpiration breath-hold (adjusted to the parameters of the CT scanner) (Fig. 3). The rest of the trunk, that is, the abdomen and pelvis, is examined in a second step with a second dose of intravenous contrast material. In the future, 4-dimensional therapy planning with respiration-gated PET acquisition to reduce smearing will improve the accuracy of PET/CT coregistration and may increase the accuracy of the measured SUV. These steps should result in improved tumor assessment in patients with lung malignancies (35) and may enable intensity-modified radiotherapy.

Patient with NSCLC, positioned for radiotherapy planning, and wearing combined chest–neck–head mask. Patient rests on flat radiotherapy planning table, and mask is fixed at both sides of table (arrows). Arms are raised above head to avoid truncation artifacts on chest images. Arms are supported by triangular cushion to avoid motion artifacts.
Assessment of Therapy Response.
Because metabolism is a more sensitive marker for response to therapy than morphology, PET and PET/CT have clear advantages over CT alone in assessing adjuvant chemotherapy or radiotherapy in patients with NSCLC (32,36). When PET/CT is performed in a therapy response monitoring setting, that is, within 4–8 wk after the start of adjuvant or neoadjuvant therapy, the scan protocol can be adjusted to the body area of interest. We schedule a PET/CT scan of the chest that will be acquired with the arms raised above the head to avoid truncation artifacts. When the data are to be used for further radiotherapy planning, the patient is positioned on the dedicated flat therapy planning table; otherwise, the regular scanner table is used. As described above, functional data are most important for assessment of the therapy response. Therefore, CT can be performed nonenhanced. However, for tumors invading mediastinal structures or the thoracic wall, we prefer data obtained with contrast enhancement at follow-up for better delineation of the tumor and adjacent organs. The CT scan is acquired during a normal expiration breath-hold. Because the radiation dose to the chest of repeated diagnostic CT scans is minimal compared with the doses applied in radiation therapy, CT should be performed in a full-dose manner with sufficient tube current and tube voltage parameters so that infiltration of the primary tumor into adjacent structures can be assessed in detail.
Follow-up for NSCLC.
In patients with a suspected recurrence of NSCLC, PET/CT provides better anatomic localization of suspected lesions than side-by-side PET and CT. This improved diagnostic performance of PET/CT has an impact on the clinical management of patients (37). The diagnostic advantages of PET/CT in this clinical situation are not limited to local disease but also include the identification of distant metastatic spread. In this setting, we recommend that PET/CT be performed in a full-dose manner with contrast agents to ensure detection and accurate localization of all metastases. An additional low-dose scan of the chest during a deep-inspiration breath-hold will be useful for the detection of pulmonary metastases.
Breast Cancer
Although in many countries institutions are being reimbursed for 18F-FDG PET in patients with breast cancer, the use of 18F-FDG PET or PET/CT has not been generally recommended in these patients. Current guidelines for the diagnosis of early-stage breast cancer do not include extensive imaging procedures for staging (38). In these early stages, the diagnosis of breast cancer is based on clinical palpation, bilateral mammography, and ultrasound. Routine staging includes physical examination and various blood tests. Even after the primary treatment of early-stage breast cancer, recommended follow-up imaging includes mammography and conventional staging methods, such as chest radiographs only (39). Nevertheless, 18F-FDG PET and 18F-FDG PET/CT have been found to be valuable in patients with breast cancer and are widely used for tumor staging, for assessment of the therapy response, and for follow-up (40–44). The potential advantages of PET/CT over PET alone are currently under discussion (45).
18F-FDG PET/CT can be used for whole-body staging of breast cancer in a single session. A whole-body imaging protocol like that shown in Table 1 offers the detection of lymph node metastases as well as distant metastases. To improve T staging with 18F-FDG PET/CT and for potential correlation of the PET/CT dataset with MRI mammography (MRM), an additional PET/CT scan in the prone position with a breast positioning aid can be performed. The shape of this positioning aid is equivalent to the shape of conventional MRM coils (Fig. 4). Noncompressed visualization of the breast enables better delineation of small lesions adjacent to the thoracic wall and allows for comparison of MRM and PET/CT findings. A possible protocol for breast scanning with 18F-FDG PET/CT is shown in Table 5.

(A) Foam mold for dedicated PET/CT breast imaging with 2 breast cups. (B) For greater patient comfort, breast imaging device is covered with cotton drapery during examination. (C) Patient positioned for breast PET/CT in prone position with arms raised above head. (D) Corresponding 18F-FDG PET/CT image of patient with suspected breast cancer revealed elevated glucose metabolism in left breast; finding was verified during surgery to be breast cancer. (E) Corresponding MRI showing mass (arrow).
For follow-up and staging of metastatic or recurrent breast cancer, 18F-FDG PET has been found to have lower sensitivity than 99mTc-methylene diphosphate bone scanning because of the various levels of 18F-FDG uptake by osteoplastic and osteolytic bone metastases (46,47). An option for solving this problem may be the use of 18F-fluoride as a radioactive tracer for PET and PET/CT (48). Furthermore, whole-body MRI may serve as an alternative and has been found to be slightly more sensitive than whole-body 18F-FDG PET as well as 18F-fluoride PET for the detection of osseous metastases (49).
Colorectal Cancer
Colorectal cancer is one of the most common malignant diseases in the Western Hemisphere and the most common type of malignancy causing liver metastases. The number of new patients in the United States exceeds 145,000 per year, with the number of estimated deaths exceeding 55,000 (50). Given the fact that the number of tumor-related deaths increased from 20.8% to 22.8% over the last 25 y, effective treatment remains a challenge (51,52). Apart from resection of the primary tumor, surgical resection of colorectal liver metastases still remains the method of choice for curative treatment. However, only 10%–25% of all patients are candidates for metastasectomy. One of the most important contraindications for hepatic resection is extrahepatic disease (53,54), making correct tumor staging necessary.
At our institution, whole-body PET/CT with intravenous contrast material and full-dose CT acquisition is used for initial tumor staging. Contrast enhancement and a regular tube current obviate additional diagnostic CT of the liver. Recently, the value of diagnostic CT as part of the PET/CT examination was reported for the detection of liver metastases. Contrast-enhanced PET/CT was able to detect more hepatic lesions than nonenhanced PET/CT (55). It is a well-known limitation of 18F-FDG PET that small liver metastases may not be detected because of smearing of 18F-FDG uptake caused by respiratory motion during PET acquisition. Thus, this limitation may be solved by the CT component of PET/CT. Because tumors of colorectal origin may metastasize to mesenteric and retroperitoneal lymph nodes, the identification of paraluminal small tumor nodes is essential. The application of an oral contrast agent will aid in the differentiation of mesenteric lymph nodes from adjacent small-bowel loops. We use a water-equivalent oral contrast agent to avoid contrast-associated PET artifacts. This contrast agent distends the small bowel without increasing HU (13). A limitation associated with this type of contrast material can be found in patients with necrotic lymph node metastases, which present as hypodense and round lesions on CT. These necrotic lymph node metastases may be difficult to differentiate from the water-filled bowel.
To improve tumor staging with respect to the detection of primary lesions and more accurate T staging, the PET/CT protocol can be further optimized to whole-body PET/CT colonography. For this procedure, the whole-body protocol (field of view: skull to upper thighs) is divided into 2 parts, as follows. First, data from the upper-body region (skull to diaphragm) are acquired during a normal expiration breath-hold in a caudocranial direction with the patient in the supine position. This PET/CT acquisition is followed by a PET/CT acquisition from the diaphragm to the upper thighs with the patient in the prone position. Before the second scan, a rectal water enema of 2–3 L is administered in conjunction with pharmacologic bowel relaxation (Table 6) (56). All patients scanned with this protocol undergo bowel cleansing the night before the examination. Initial results evaluating the PET/CT colonography protocol have shown improved T staging compared with that provided by CT colonography (our unpublished data; January 2006). In contrast to normal CT colonography, this protocol uses a water enema rather than air to maintain bowel distension. Resorption of air from the bowel in between CT and PET would require additional air application while scanning, and this air application might induce bowel motion. Thus, the water enema seems more practical for PET/CT colonography.
As for other tumor entities, therapy response monitoring scans in patients with colorectal cancer may be limited to the body region of interest. Because functional data are most relevant for therapy assessment and because functional changes frequently precede morphologic changes, we perform the CT component without contrast material and in a low-dose manner in this clinical setting.
Gastrointestinal Stromal Tumors (GIST)
For the initial staging of GIST, a whole-body examination seems advisable to detect all potential metastases. It has been shown that hepatic metastases from GIST may be masked on contrast-enhanced CT scans because of similar enhancing characteristics for the metastasis and its harboring organ. This scenario applies specifically to CT images acquired in the portal–venous contrast phase, the phase typically used in whole-body PET/CT to image the liver. On nonenhanced CT scans, GIST metastases usually show as hypodense lesions surrounded by normal liver parenchyma. Therefore, a nonenhanced CT component of a PET/CT examination may be of benefit for initial GIST staging. More lesions may be detected by nonenhanced CT than by 18F-FDG PET. Therefore, these imaging modalities complement each other for GIST staging.
Although intravenous contrast agents may obscure GIST metastases from detection, oral contrast agents will improve lesion detection and localization within the abdomen and should be part of the PET/CT examination. These contrast agents may be either positive or water equivalent for initial tumor staging. However, in patients undergoing imatinib therapy, cystic changes in peritoneal metastases may make these lesions difficult to differentiate from bowel loops if a water-equivalent contrast agent is used. In these cases, a positive contrast agent may be preferable.
18F-FDG PET and 18F-FDG PET/CT have been shown to more accurately differentiate responders and nonresponders than morphology alone in assessments of the response of GIST to therapy (57–59). In patients responding to imatinib therapy, 18F-FDG uptake by the tumor and its metastases will decrease. GIST metastases are well known to liquefy when patients undergo imatinib therapy, leading to a decrease in lesion density on CT. This change in lesion density may unmask small hepatic metastases previously not detected because of similar densities for the lesion and the surrounding liver parenchyma. Thus, the CT portion of the PET/CT examination must be analyzed critically to avoid false characterization of these unmasked lesions as newly developed metastases.
Patients who have tumor recurrence and who are undergoing therapy will show an increase in 18F-FDG uptake on 18F-FDG PET. The corresponding CT image often shows a nodule within a mass (Fig. 5) (60). This nodule-within-a-mass pattern represents a newly developed, small contrast material–enhanced lesion within a liquefied metastasis. It serves as an important indicator of tumor progression on CT and may be identified earlier than increased 18F-FDG uptake in smaller lesions. To detect such a nodule within a mass, contrast-enhanced CT is required and should be included in the PET/CT protocol during the follow-up of patients with GIST.
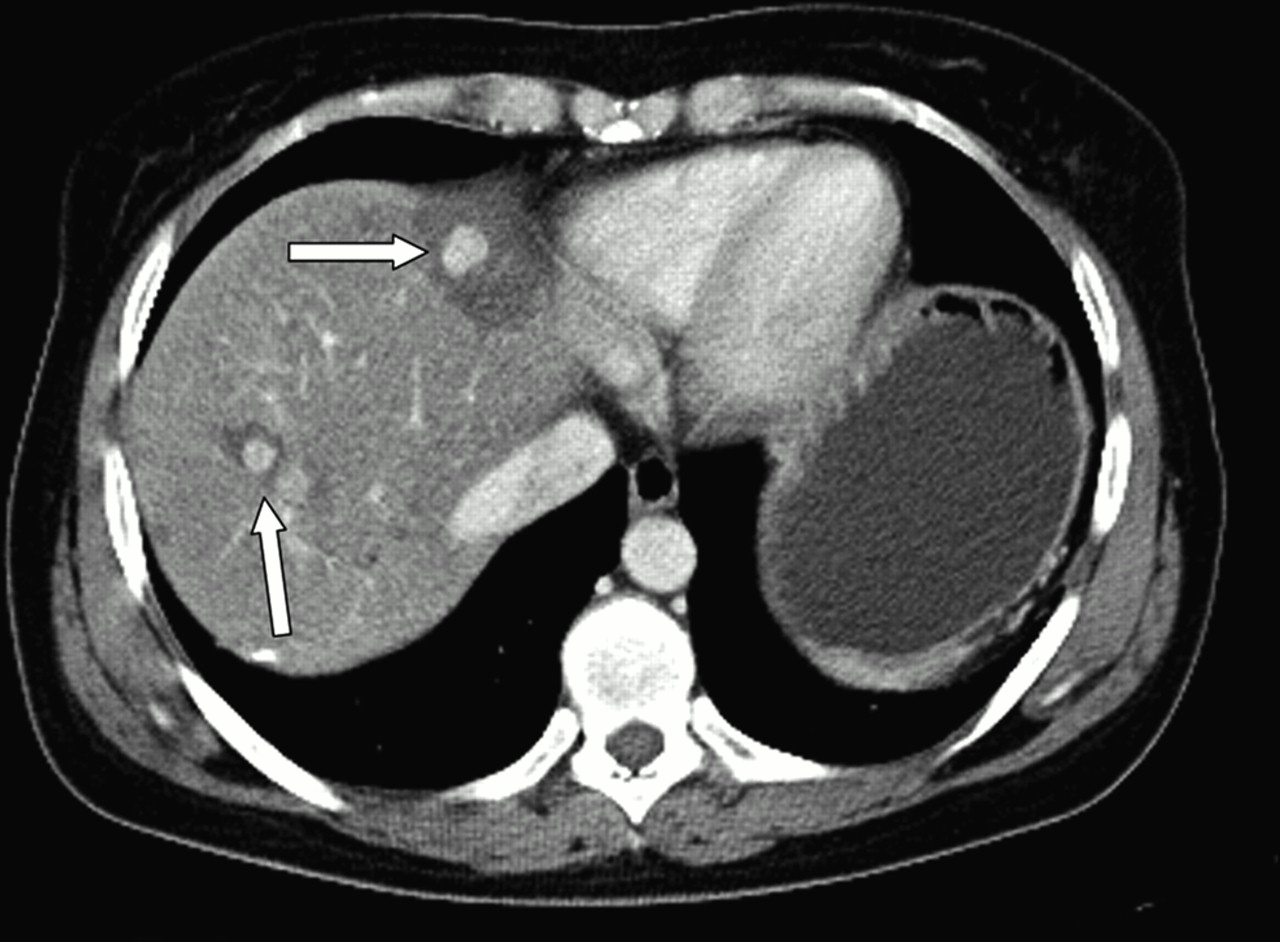
Male patient with GIST 1 y after initiation of imatinib treatment. CT image shows newly developed, round, contrast-enhancing nodules (arrows) within liquefied metastatic remnants. This nodule-within-a-mass pattern is typical CT appearance of GIST recurrence during imatinib treatment.
PET/CT for Image-Guided Locally Ablative Therapy
Within the last decade, a variety of local treatment options have been introduced and evaluated for focal tumor manifestations, such as HCC and liver metastases from colorectal carcinoma. Even for bronchial carcinoma and bone metastases from different primary tumors, locally ablative techniques have been established. Methods include intravascular approaches, such as chemoembolization and intrahepatic arterial infusion therapy, and locally ablative therapies, such as interstitial laser therapy, cryotherapy, and radiofrequency ablation (61). Although 18F-FDG PET has been shown to be a very sensitive and accurate tool for the diagnosis of hepatic tumor manifestations in patients with colorectal carcinoma (62,63), its diagnostic value for HCC staging is low (64,65). Remarkably, the detection of extrahepatic HCC manifestations by 18F-FDG PET has been shown to be more accurate than primary tumor visualization (66).
The clinical routine staging of suspected liver malignancies is based on contrast-enhanced imaging modalities. Despite recent improvements in radiologic imaging, surgeons find undetected intra- and extrahepatic tumors during laparotomy in as many as 55% of cases (67), resulting in a change in therapy. These data make additional staging information mandatory. Furthermore, an extrahepatic tumor manifestation is a clear contraindication for locally ablative therapies for malignant liver lesions (53,54). Whole-body PET/CT with contrast-enhanced CT (Table 1) can reliably detect patients amenable to locally ablative therapies for colorectal liver metastases and has proved superior to PET alone (68).
Depending on the primary tumor, an additional multiphase CT examination of the liver can be added immediately before the PET/CT examination to identify the full extent of intrahepatic tumors, especially for adenocarcinoma of the pancreas, HCC, and neuroendocrine tumors of the gastrointestinal tract. These tumors and their metastases typically enhance in the early arterial phase. The multiphase CT examination is performed during normal expiration immediately before the PET/CT examination. The patient is positioned on the PET/CT table with arms raised above the head. PET/CT data can be fused with CT data from the separate CT spiral after the examinations are complete. Table 7 summarizes the CT protocol in use for multiphase scanning of the liver. If this liver CT protocol is used, then a whole-body CT scan for attenuation correction of the whole-body PET scan can be performed without additional contrast agents.
The optimal time to perform postinterventional imaging to evaluate therapy response or tumor recurrence is still controversial. Because rimlike enhancement patterns caused by postinterventional hyperperfusion and tissue regeneration are frequently found by contrast-enhanced morphologic imaging procedures, 18F-FDG PET or 18F-FDG PET/CT may be advantageous if performed within 24 h of ablation (69). After this short time interval, tissue regeneration may lead to a rimlike area of 18F-FDG uptake surrounding the ablation necrosis. Just as on contrast-enhanced CT and MRI scans, this rimlike area of tracer uptake may hamper the detection of residual tumors. For patients with complete tumor ablation on the 24-h follow-up scan, we currently perform the next follow-up scan 3 mo after the intervention. Both the initial scan after ablation and the 3-mo follow-up scan are limited to the liver, and data obtained with contrast enhancement are acquired. The next follow-up scan is scheduled for 6 mo after the intervention and includes whole-body PET/CT to stage potentially new distant metastases. These follow-up protocols may differ at other institutions. For 18F-FDG PET–negative lesions, contrast-enhanced CT or MRI (if necessary with both gadolinium and iron oxide) is performed for follow-up (70).
CONCLUSION
Different clinical situations require custom-fit CT protocols in PET/CT. Although the accuracy of tumor staging may benefit from a fully diagnostic CT component, low-dose, nonenhanced CT may be sufficient for assessment of the therapy response. Of course, PET/CT will not be able to fully replace CT in cancer imaging; however, PET/CT performed with dedicated CT protocols may be able to reduce the number of additionally required CT scans. Thus, the question to be asked is not whether PET/CT can replace CT for cancer imaging but whether PET/CT can replace additional diagnostic CT for cancer imaging. If adapting the CT protocol of PET/CT to the clinical situation, this question must be answered with a clear “yes.”
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.
- 42.
- 43.
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- Received for publication January 30, 2006.
- Accepted for publication May 8, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- DEFINING DIAGNOSTIC CT
- PROTOCOL CONSIDERATIONS FOR TUMOR STAGING
- PROTOCOL CONSIDERATIONS FOR THERAPY ASSESSMENT
- IS THERE A NEED FOR PET/CT OF BRAIN?
- ADDITIONAL LOW-DOSE CT FOR DETECTION OF PULMONARY NODULES
- BREATHING PROTOCOL FOR WHOLE-BODY PET/CT
- IS IT NECESSARY TO ADJUST CT PARAMETERS TO NUMBER OF CT SCANNER DETECTOR ROWS?
- IMAGING CANCER OF CHEST AND ABDOMEN
- CONCLUSION
- Footnotes
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Weight-Based Protocols Offer Significant Reduction in Radiation Dose Without Affecting PET-CT Image Quality
- Variations in Clinical PET/CT Operations: Results of an International Survey of Active PET/CT Users
- Integrated PET/CT in the staging of nonsmall cell lung cancer: technical aspects and clinical integration
- SPECT/CT
- Introduction