


Abstract
242505
Introduction: End-stage renal disease is a substantial contributor to both morbidity and mortality. The primary treatment modalities for this patient population consist of hemodialysis or peritoneal dialysis, as well as graft transplantation from a living or deceased donor. Medical complications manifest in the form of (AR), both of which are parenchymal pathologies. It is critical to diagnose complications associated with renal transplants accurately, as many of these issues may be treatable with early detection. Nuclear medicine, CT, and MR imaging investigations are complementary. The investigation of these two abnormalities in nuclear medicine consists of two primary phases including flow and uptake. The flow phase is quantified by observing the aorta and kidney simultaneously. The uptake phase consists of revealing the extent of radiopharmaceutical absorption in the kidney tissue, the discharge power of the radioactive substance, and the moment the bladder becomes visible. The flow phase is normal in the ATN, but the discharge portion of the second phase is problematic; in the AR, the kidney experiences issues in both phases. The objective of this work is to evaluate a deep learning-based algorithm to a transplanted nuclear medicine scan to detect ATNs and AR.
Methods: In this study, 78 patients (AR: 43 and ATN: 35 patients) with transplanted kidneys were involved. Following the intravenous administration of 740 MBq f Tc-99m ethylene dicysteine (EC), a single-head gamma camera was utilized to acquire an image of the transplanted kidney with a matrix dimension of 128 × 128 in 2 phases. The flow phase was acquired for 1 minute (60 frames) whereas the uptake phase was acquired for 30-60 minutes (30-60 frames). We normalized each phase for individual patients by scaling them to their respective maximum values across all frames. After, uptake phases were padded to 60 frames, and flow and uptake phases were concatenated to a single 120 frames. The patients were allocated into two groups: training (70%) and test (30%). For validation purposes, 20% of the training dataset was utilized. InceptionResNet model was used as neural network architecture. We utilized two density layers (512 and 128) with batch normalization and the ReLU activation function for each layer, as opposed to the top layer of InceptionResNet. A Softmax layer was implemented at the model's conclusion to facilitate binary classification. A batch size of 2 and 300 epochs were utilized to train the models. The f1 score, precision, accuracy, area under the curve (AUC), and recall were employed as performance metrics to evaluate the model on the test data.
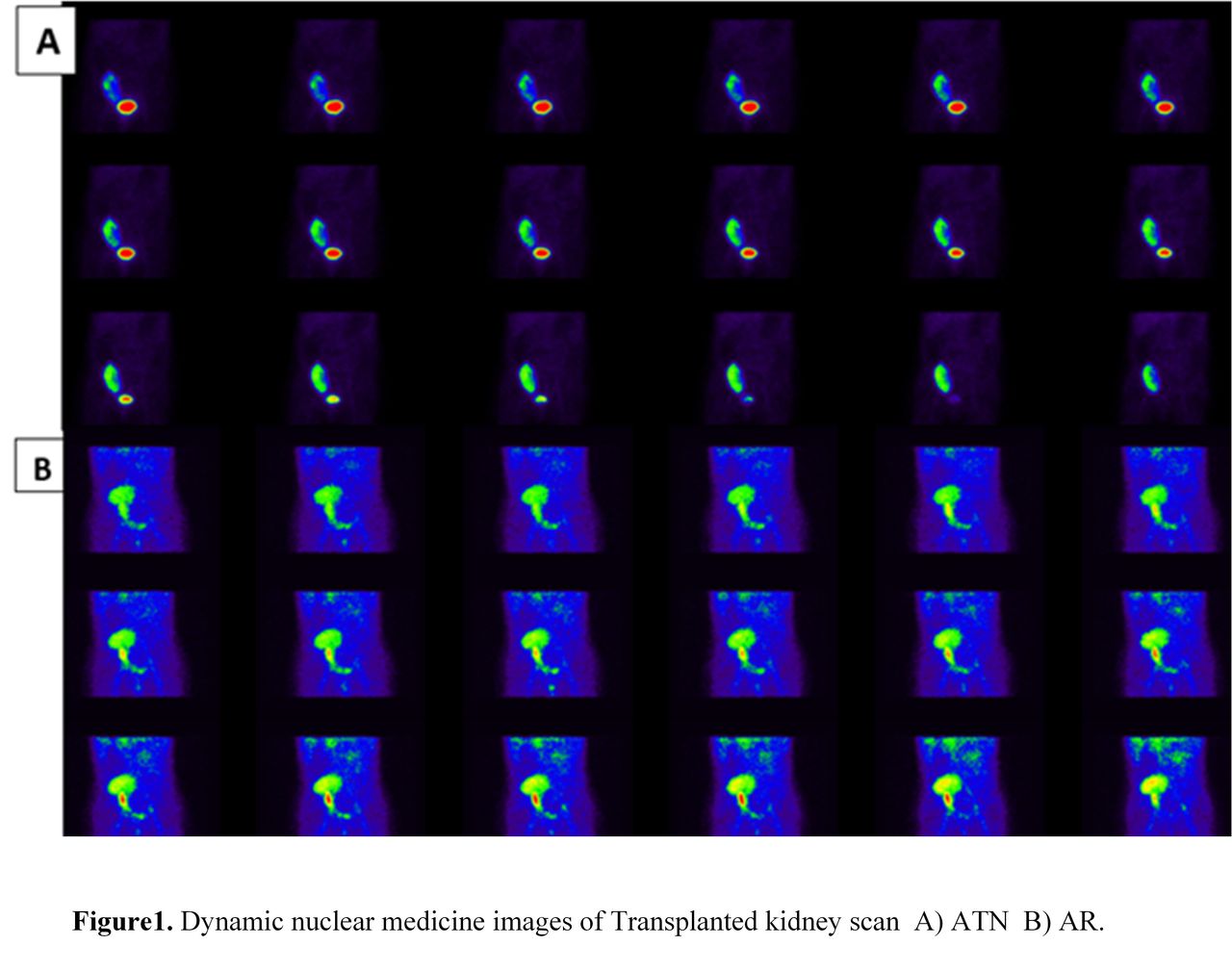
Results: AR and ATN patients are depicted in Figure 1. The results of this study are shown in Figure 2. The accuracy and AUC were 0.67 and 0.72 for the InceptionResNet model. Recall (0.77 and 0.60), precision (0.67 and 0.67), and f1-score (0.71 and 0.60) were achieved for AR and ATN, respectively.
Conclusions: Deep learning models may be useful in the diagnosis of anomalies in renal transplants. Notwithstanding certain constraints, such as the data's singular center and insufficient sample size, it is feasible to attain superior outcomes through the implementation of alternative filtering, using other deep learning algorithms.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.