


Abstract
241582
Introduction: PET imaging is widely used for detection and staging of cancers as well as evaluation of treatment response. In SCINTIX® biology-guided radiotherapy (BgRT), PET signals are also used to guide external radiation beams from the LINAC to the tumor in real time. The RefleXion® X1 BgRT system consists of two 90o PET arcs, a 6 MV LINAC, a binary multi-leaf collimator, a kVCT and an MV detector mounted on a fast-rotating slip ring gantry with 60 rpm rotation speed. The PET detectors and LINAC are mounted such that they lie in the same transaxial plane. During treatment delivery, the PET data is reconstructed every 100 milliseconds to generate limited time sampled (LTS) data sets to guide radiation delivery to the tumor. In this work, we describe a pre-clinical X1 PET image simulation and BgRT treatment planning system in research mode and demonstrate its ability with diagnostic PET/CT data for patients with hepatic lesions.
Methods: The pre-clinical PET image simulation system uses diagnostic PET/CT data to simulate RefleXion® X1 BgRT system PET data acquired at different stages in the BgRT workflow (treatment planning, pre-scan, and delivery). In clinical BgRT workflow, a treatment planning PET scan is first performed on the X1, which is used to check activity concentration (AC) and normalized target signal (NTS) values for the tumor and generate a BgRT plan. A biological tracking zone (BTZ) is defined to encompass the full range of motion of the tumor plus margin. The BTZ is divided into multiple bed positions, and the treatment planning PET image is acquired using 10 gantry revolutions per bed position and 4 passes. Before each BgRT delivery, a pre-scan PET image is acquired to evaluate AC and NTS on the treatment day. The pre-scan PET image is acquired with 10 gantry revolutions per bed position and a single pass. The emulated BgRT delivery uses LTS PET images acquired in the most recent 500 ms timing window, corresponding to a 180° gantry rotation. For emulated delivery, each LTS PET image was simulated for 500 ms data acquisition. Image degradation factors such as scatter, randoms and detector efficiencies are modelled in the simulator and have been previously validated with measurements. To demonstrate system capability, we used diagnostic PET-CT dataset from a patient injected with 389 MBq of FDG activity as a less-than-ideal scenario, since 555 MBq of injected activity is recommended in clinical BgRT planning and delivery. While an iterative reconstruction algorithm with scatter correction was used in reconstructing the diagnostic PET images resulting in a higher contrast, filtered back-projection was used in the BgRT PET simulation system so that the results are linear and unbiased.
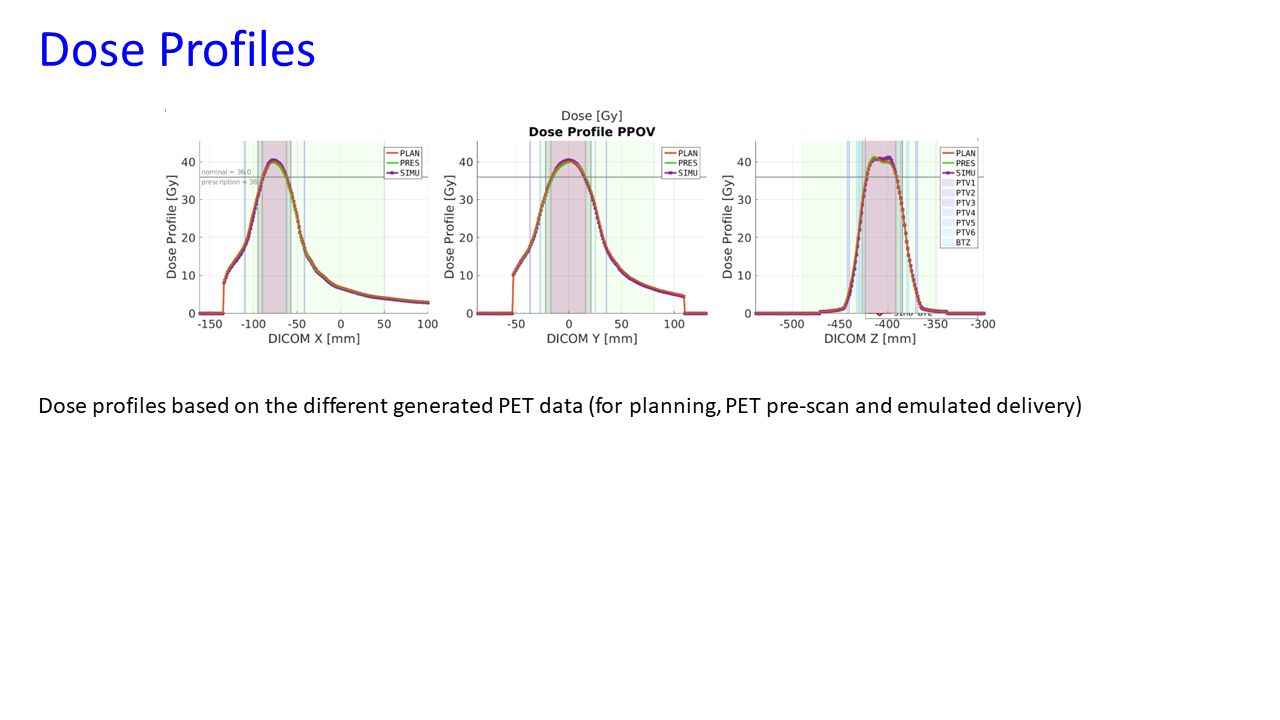
Results: The min, max, and mean activity in the hepatic tumor was 12 kBq/ml, 46 kBq/ml, and 30 kBq/ml in the diagnostic PET while they were 17 kBq/ml, 25 kBq/ml, and 21 kBq/ml in the simulated planning X1 PET images. The mean background activity was 11.4 kBq/ml and 12.4 kBq/ml in the diagnostic and simulated planning PET respectively. The NTS values were 9.83, 8.85, and 9.32 and the AC values were 12.98 kBq/ml, 15.6 kBq/ml, and 13.07 kBq/ml in the simulated treatment planning PET, pre-scan PET, and delivery PET images, respectively. All the AC and NTS values in the simulated PET images met BgRT treatment planning and delivery criteria. Based on the simulated PET image, a BgRT plan was created to deliver 36 Gy in 4 fractions to the tumor. The emulated delivery predicted a treatment time of just under 15 minutes. The conformality index was 1.12, 1.17, and 1.13 while the expected gross target volume (GTV) coverage by the prescription dose was 100% based on simulated treatment planning, pre-scan, and emulated delivery PET images.
Conclusions: This work demonstrates that we can simulate the BgRT planning and delivery workflows using diagnostic PET-CT data. This simulation system could be used to check BgRT feasibility and identify optimization parameters for clinical BgRT planning.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.