


Abstract
241370
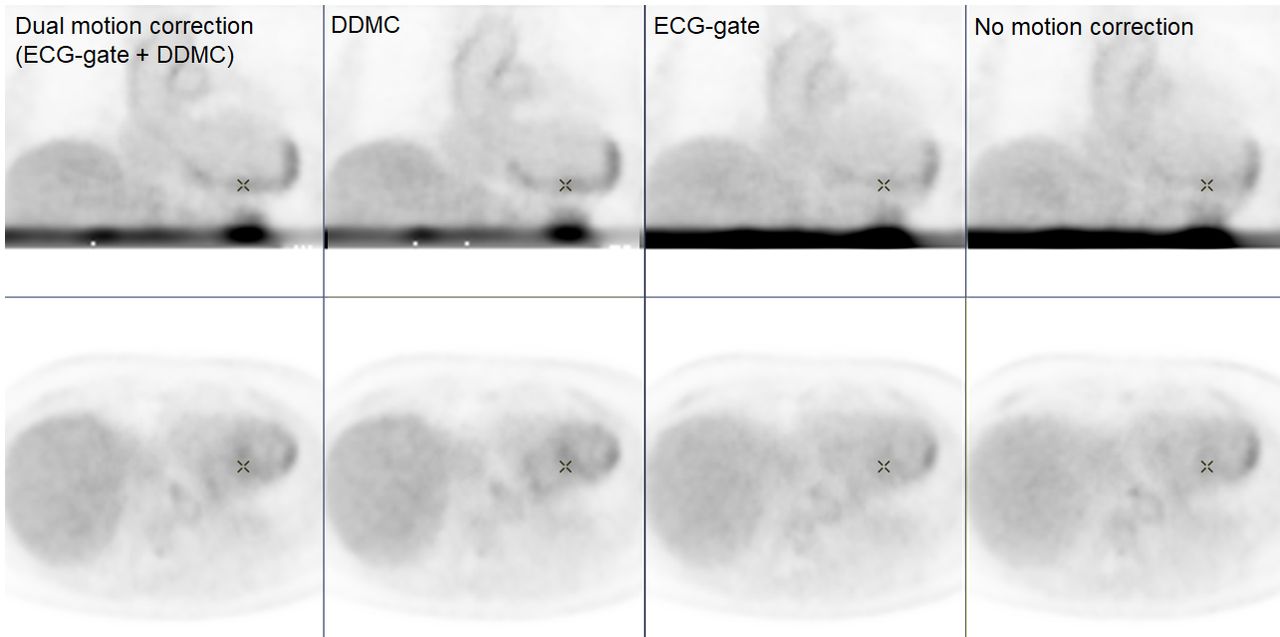
Introduction: We aim to validate the clinical feasibility of the dual motion correction techniques using ECG gating and data-driven respiratory motion correction for cardiac PET.
Methods: This study included the seven patients who underwent cardiac PET under overnight fasting condition using F18-FDG for the evaluation of active cardiac sarcoidosis. One hour after the intravenous injection of 3.7 MBq/kg BW of FDG, 30-minute emission scans were acquired using Discovery MI PET/CT scanner (GE HealthCare) while ECG was acquired with body surface electrodes. All PET data were reconstructed under 4 conditions: "no motion correction (noMC)", "with 3-segment ECG-gating (ECG-gate)", "with data-driven respiratory motion correction (DDMC)", and "with ECG gate and DDMC (ECG+DDMC)". DDMC were performed on a Matlab-based toolbox (Duetto, GE HealthCare). A boundary box was set at lower chest and upper abdomen including the whole heart. A 2-second ultra-fast frame reconstruction was executed from a list data, and respiratory motion was estimated using a volume inside the boundary box by 3D image-based registration. The reference for registration was set to the frame at 30 seconds. The collection time of image data under each condition was standardized to 10 minutes for comparison. Image analysis was performed using AW Server 3.2 Ext 2.0 (GE Healthcare). Spherical region of interest (ROI) covering the whole left ventricular wall was set with reference to CT image. SUVmax of the LV (SUV-LV) and the metabolic target volume of the accumulation in the left ventricular wall with the threshold of SUVmax of the blood pool (MTV-LV) was measured. The SUV-LV and MTV-LV were compared among the 4 conditions using Wilcoxson's signed rank test. P<0.05 was set at statistical significance.
Results: The median (range) of the SUV-LV were 8.9 (6.3 – 15.1) for "noMC", 9.0 (6.4 – 15.8) for "ECG-gate", 9.4 (6.3 – 15.4) for "DDMC", and 9.4 (6.5 – 17.1) for "ECG+DDMC", respectively. The median (range) of MTV-LV were 133.0 (8.6 – 204.0) for "noMC", 97.2 (15.1 – 196.0) for "ECG-gate", 127.0 (6.5 – 203.0) for "DDMC", and 117.0 (13.0 – 226.0) for "ECG+DDMC", respectively. SUV-LV by "ECG+DDMC" was higher than those by "noMC", "ECG-gate" and "DDMC" with statistical significance (p < 0.05). Meanwhile, there was no statistically difference in MTV-LV.
Conclusions: The dual motion correction techniques using ECG gating and DDMC for cardiac PET may reduce an underestimation of myocardial accumulation due to blurring associated with respiration and heartbeat, allowing more accurate assessment of the distribution of myocardial accumulation.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.