


Abstract
241065
Introduction: 18F-PSMA-1007 PET/CT plays an important role in the assessment of prostate cancer patients, more over bone is the most common site of metastases in prostate cancer. It is considered that 18F-PSMA-1007 is expressed in benign conditions.
Extrapolating this principle, the present study aimed to describe different patterns of benign skeletal 18 F-PSMA-1007 avid PET/CT findings in our center patient population. It is of utmost importance to uncover those lesions masquerading as metastatic disease with subsequent accurate patient management and better outcomes.
Methods: Enrollment of 100 18-F PSMA-1007 PET/CT studies for patients with prostate cancer, database is maintained within the department that comprises de-identified patient information, primary prostate malignancy, and stage-defined findings on PSMA PET/CT, also any unusual PSMA osseous uptake. An observation of non-metastatic osseous PSMA uptake was documented, described, and followed up.
Results: All those non-metastatic osseous uptakes were then subdivided into the following 2 categories: benign pathological uptake and primary osseous neoplasm.
Benign Pathological PSMA Uptake:
We identified mild to moderate focal uptake at sites of healing
Fractures, degenerative arthritis, osteophytes in the spine, and schmorl's nodule. Also, diffuse variable PSMA uptake in Paget’s disease of the bone and fibrous dysplasia.
This may be misinterpreted as metastatic disease or overlooked underneath metastatic disease. We reported a case of bone marrow edema (early traumatic insult), to the best of our knowledge it wasn't reported before. (fig.1)
Primary osseous neoplasm PSMA Uptake:
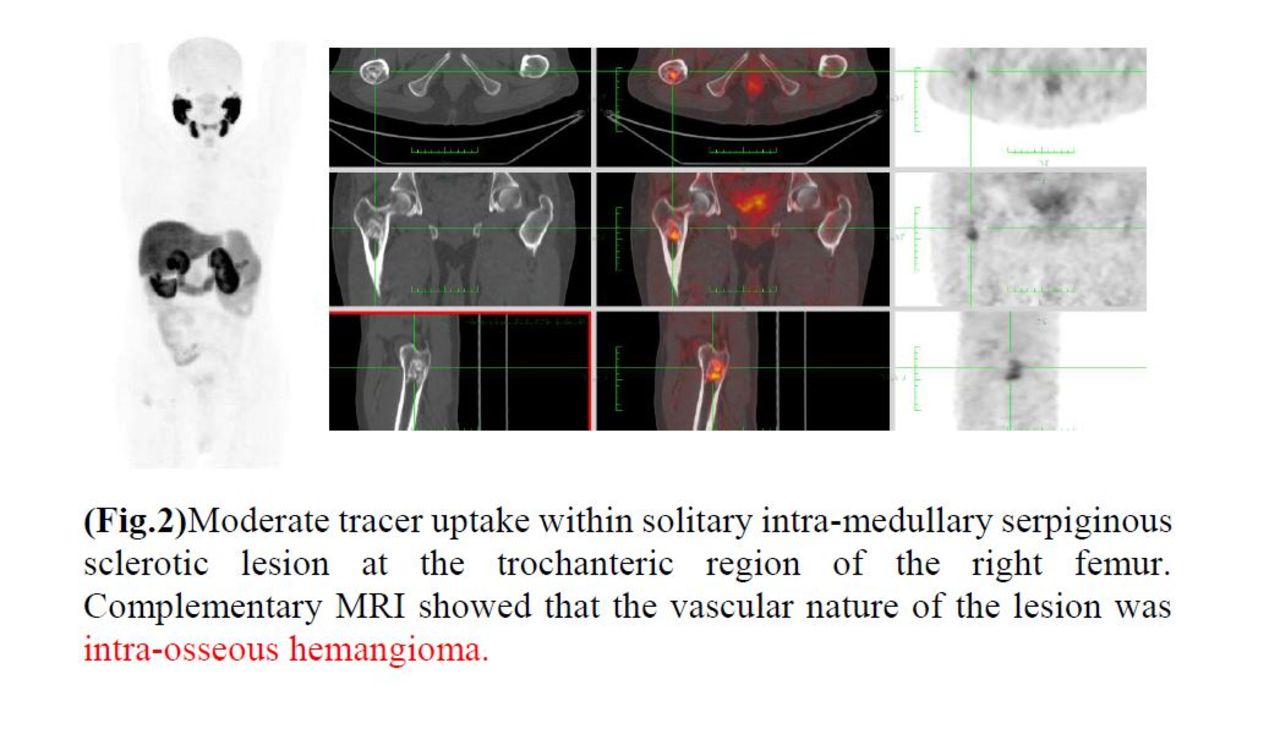
The incidental intense PSMA-radiotracer uptake in patients with benign vascular tumors such as benign hepatic and vertebral hemangiomas and subcutaneous capillary hemangioma have been shown in several case reports. (7) In our study we described a moderate grade of PSMA-uptake in intra-osseous hemangioma at the femoral shaft (Fig.2) and vertebrae.
Paying attention to benign non-metastatic skeletal lesions leads to avoiding erroneous identification of metastatic bone which is considered (Stage cM1b); so correlation with clinical history, the CT portion of the PET/CT, or other advanced imaging usually allows better differentiation of prostate cancer two aforementioned bone entities. (3)
Conclusions: It is important to be aware of confounding PSMA uptake in non-prostatic skeletal pathologies to optimize interpretation, moreover accurate implementation of patient management by avoiding significant false upstaging or false down-staging.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.