


Abstract
24103
Introduction: Evaluating the ability and effectiveness of Selective Internal Radiation Therapy (SIRT) Treatment with hepatic renal metastasis. Liver metastasis is the most common form of malignant liver disease and is associated, in general, with a poor prognosis. Metastasis comes most frequently from primary colorectal cancers, and about 20% of patients present with liver metastases(1).SIRT is an effective treatment for hepatic metastasis in hepatocellular carcinoma (HCC), and the evaluation of other cancer types needs to be evaluated. Early analysis of metastatic renal cancer treatment with SIRT appears to be a promising treatment option. 90Y (SIRT) radioembolization has grown in popularity over the past few years. Using 90Y SIRT enables physicians to deliver a high-absorbed dose directly to the tumor with a precisely placed catheter; this allows for selective lesion radiation therapy (2).
Methods: After intra-arterial injection of 3.14 mCi Tc-99m MAA macro aggregated albumin into the replaced right hepatic artery distribution and 2.0 mCi Tc-99m MAA macro aggregated albumin into the middle hepatic artery distribution, this patient weighing 240 lbs. and 69 inches tall was transferred to the nuclear medicine department. Planar imaging was performed over the upper abdomen and thorax. AP images of the chest and abdomen were performed for ten minutes each, and lateral abdominal views were performed for five minutes. See (Table 1.) for contour densities and volumes from the computerized tomography (CT) collected during the mapping procedure.
SPECT imaging was also performed over the same area for dosimetry purposes. This data was then used to calculate a lung shunting percentage from the liver. Images demonstrate activity within the injection distribution into the replaced right and middle hepatic arteries. Mild gastric activity seen is likely related to free technetium. The lung shunt is calculated at 5.12%. 4D-CT imaging was fused with SPECT MAA imaging to evaluate lung shunting and calculated tumor to normal tissue ratio (TNR) to calculate specific patient SIRT activity to deliver. See (Table 2.) for the 2D lung shunt calculation statistics.
After the TNR calculation was performed, a dose reduction of 50% was applied to the SMAC to optimize the tumor absorbed dose and reduce normal liver tissue or not target absorbed dose. It was determined that a prescribed dose of 0.69 GBq (18.64 mCi) was needed to treat the target tumors.
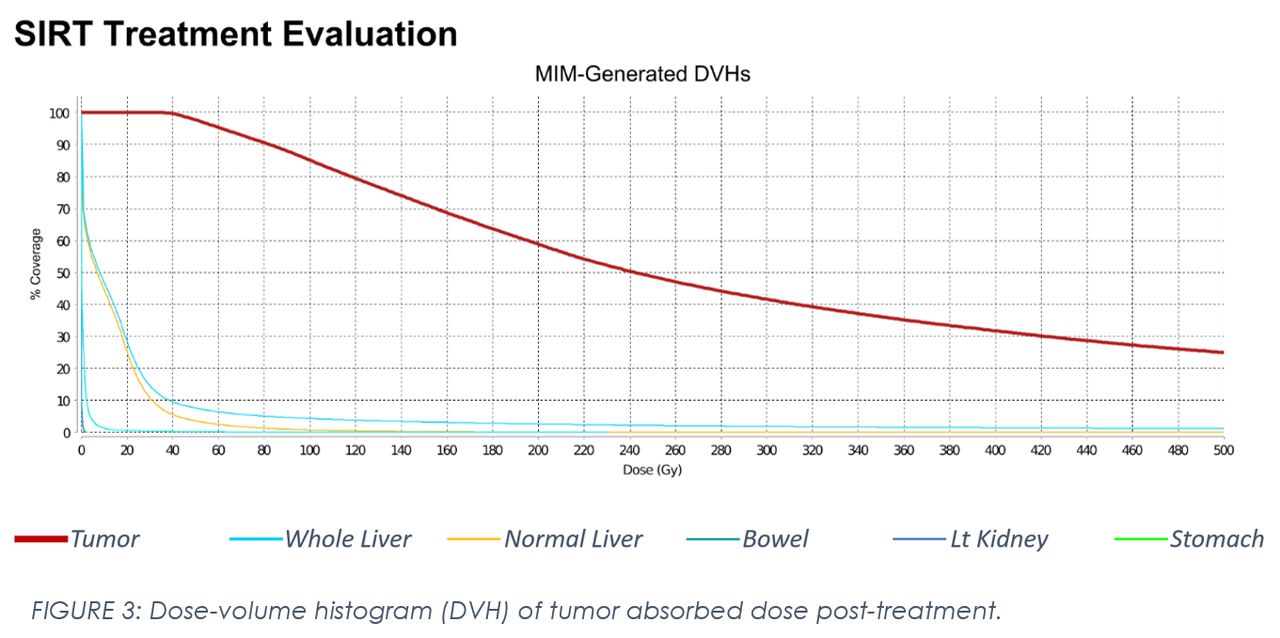
Results: After SIRT treatment, the tumors located in the right lobe of the liver received an average absorbed dose of 374.43 Gy while keeping the normal liver absorbed dose to 13.14 Gy. It was determined before treatment that an absorbed dose was more significant than 120 Gy to the tumors while limiting the absorbed dose to the normal liver tissue to 30 Gy. See (Table 3.) for dose volume histogram results and (Figure 2.) for axial PET/CT fusion images post treatment. This treatment delivered an absorbed dose of 3.12 times more to the tumor and 43.8% less dose to the normal or non-target liver tissue. Treatment response is predicted to be extremely well; post-treatment, the patient had only minimal abdominal discomfort for a few days, see (Figure 3.) for the DVH curve. Continued follow-up on treatment area will continue at three- and six-month increments. Treatment of the left lobe is scheduled to alleviate the tumor burden on the opposite side of the liver.
Conclusions: This study demonstrated a feasible Renal Cell Carcinoma (RCC) treatment option. Tumoricidal absorbed dose was easily achieved while normal liver tissue was kept below 30 Gy. This treatment is felt to show a complete to near complete response in the future. The RCC tumor’s vasculature affinity for the resin spheres leads to a potentially highly effective SIRT treatment on hepatic metastasis. Additional data must be collected comparing the results from this single patient study to a larger body of RCC patients.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.