


Visual Abstract

Abstract
Understanding which patients with human epidermal growth factor receptor 2 (HER2)–negative or –low metastatic breast cancer (MBC) benefit from HER2-targeted strategies is urgently needed. We assessed the whole-body heterogeneity of HER2 expression on 89Zr-trastuzumab PET (HER2 PET) and the diagnostic performance of HER2 PET in a large series of patients, including HER2-negative and -low MBC. Methods: In the IMPACT-MBC study, patients with newly diagnosed and nonrapidly progressive MBC of all subtypes were included. Metastasis HER2 status was determined by immunohistochemistry and in situ hybridization.89Zr-trastuzumab uptake was quantified as SUVmax and SUVmean. HER2 immunohistochemistry was related to the quantitative 89Zr-trastuzumab uptake of all metastases and corresponding biopsied metastasis, uptake heterogeneity, and qualitative scan evaluation. A prediction algorithm for HER2 immunohistochemistry positivity based on uptake was developed. Results: In 200 patients, 89Zr-trastuzumab uptake was quantified in 5,163 metastases, including 186 biopsied metastases. With increasing HER2 immunohistochemistry status, uptake was higher (geometric mean SUVmax of 7.0, 7.6, 7.3, and 17.4 for a HER2 immunohistochemistry score of 0, 1, 2, or 3+, respectively; P < 0.001). High uptake exceeding 14.6 (90th percentile) was observed in one third of patients with a HER2-negative or -low metastasis biopsy. The algorithm performed best when lesion site and size were incorporated (area under the curve, 0.86; 95% CI, 0.79–0.93). Conclusion: HER2 PET had good diagnostic performance in MBC, showing considerable whole-body HER2 heterogeneity and uptake above background in HER2-negative and -low MBC. This provides novel insights into HER2-negative and -low MBC compared with standard HER2 immunohistochemistry on a single biopsy.
In metastatic breast cancer (MBC), performing a biopsy of a metastasis to assess human epidermal growth factor receptor 2 (HER2) expression with immunohistochemistry is the reference standard (1). A biopsy with an immunohistochemistry score of 3+ or 2+/in situ hybridization amplified is the conventional method to identify patients for HER2-targeting therapy (1,2). However, biopsies are invasive and provide information about only a part of a single lesion. Moreover, the whole-body heterogeneity of HER2 expression within and between lesions affects tumor response to conventional HER2-targeting therapy (3,4). Whether this also plays a role in responses to new-generation HER2-targeting antibody–drug conjugates such as trastuzumab-deruxtecan in part of the patients with HER2-low disease (5,6) is unclear. Whole-body HER2 heterogeneity is of interest to improve insight and potentially to optimize patient selection.
Noninvasive visualization of HER2 presence in all metastases within the patient can be performed with molecular imaging, such as 89Zr-trastuzumab PET (HER2 PET) (7–9). However, the diagnostic performance of HER2 PET, particularly in HER2-negative and -low disease, is unknown. Furthermore, whereas whole-body HER2 heterogeneity has been reported in smaller studies, it has not, to our knowledge, been assessed with HER2 PET in HER2-negative and -low MBC (10–12). Therefore, the present substudy of the prospective IMPACT-MBC study was performed (13). In the IMPACT-MBC study (NCT01957332), the clinical utility of extensive baseline molecular imaging was assessed in patients with newly diagnosed and nonrapidly progressive MBC regardless of breast cancer subtype (including HER2-negative, -low, and -positive disease). For the present substudy, we assessed the diagnostic performance of HER2 PET to assess the HER2 status of a metastasis biopsy and evaluate whole-body heterogeneity in HER2-negative, -low, and -positive MBC.
MATERIALS AND METHODS
Patients and Study Design
Patients with the first presentation of nonrapidly progressive MBC were enrolled in the multicenter IMPACT-MBC study between August 2013 and May 2018. All patients provided written informed consent. The study was approved by the Medical Ethical Committee of the University Medical Center Groningen (UMCG) (approval MREC#2013/146), according to the Central Committee on Research Involving Human Subjects. The study was performed at 4 Dutch academic centers: UMCG, Amsterdam University Medical Center, Radboud University Medical Center, and Erasmus Medical Center (ClinicalTrials.gov identifier NCT01957332). Patients underwent extensive standard diagnostic assessment at baseline with contrast-enhanced CT, 99mTc bone scintigraphy, [18F]FDG PET, and a biopsy of a metastasis. Additional MRI scans were made if indicated or when brain metastases were suspected. Besides these conventional diagnostics, experimental molecular imaging was performed, including 16α-[18F]fluoro-17β-estradiol PET, HER2 PET, and early repeated [18F]FDG PET after 2 wk. Baseline HER2 PET and standard clinicopathologic data were used for the present substudy. Actual treatment decisions and patient outcomes are currently being analyzed and will be reported separately.
Biopsied Metastases
For each patient, a histologic biopsy from a suspected metastasis, apart from skin lesions, was performed by a radiologist guided by conventional imaging according to standard clinical care procedures. HER2 PET and 16α-[18F]fluoro-17β-estradiol PET were not used to guide the biopsy. Biopsies were obtained before HER2 PET. An experienced breast pathologist, masked to the imaging results, reviewed the formalin-fixed and embedded biopsy samples centrally. Immunohistochemistry for estrogen receptor (SP-1; Ventana/Roche) and HER2 (SP3; Thermo Fisher Scientific, Inc.) were performed on an automated staining platform (Ventana Benchmark Ultra; Ventana/Roche) according to the manufacturer’s protocols. Estrogen receptor status was considered positive if at least 10% of the tumor cells stained positively (14). HER2 staining was scored as 0 to 3+ according to the guidelines of the American Society of Clinical Oncology and the College of American Pathologists (1). A tumor lesion was considered HER2-positive with a score of 3+ and HER2-negative with a score of 0 or 1+. In the case of an immunohistochemistry score of 2+, HER2 dual-brightfield in situ hybridization (INFORM dual BRISH; Ventana/Roche) was performed and scored according to the guidelines of the American Society of Clinical Oncology and the College of American Pathologists.
HER2 PET Imaging
Clinical-grade 89Zr-trastuzumab was produced as described previously at UMCG and Amsterdam University Medical Center and used locally or shipped to Radboud University Medical Center and Erasmus Medical Center (15). Patients received 37 ± 3.7 MBq (10%) of 89Zr-trastuzumab intravenously, supplemented with 50 mg of unlabeled trastuzumab (7,9). Four days after injection, patients were scanned from head to upper thigh at up to 9 bed positions at a rate of 5 min/bed position, combined with a low-dose CT scan for attenuation correction and anatomic reference. Scans at UMCG, Radboud University Medical Center, and Erasmus Medical Center were obtained on a Biograph mCT 64-slice PET/CT camera or a Biograph mCT 40-slice PET/CT camera (Siemens/CTI), and scans at Amsterdam University Medical Center were obtained on an Ingenuity TF or a Gemini TF (Philips). PET images were reconstructed using the harmonized reconstruction algorithm recommended for multicenter 89Zr-monoclonal antibody PET trials (16).
Quantitative Whole-Body HER2 PET Evaluation
89Zr-trastuzumab uptake was quantified in all metastases, including the biopsied metastasis, and in healthy background tissue. The 89Zr-trastuzumab uptake was quantified by 2 trained observers using AMIDE software version 0.9.3 (17). Metastases were identified on CT (including metastases < 1 cm), bone scanning, or [18F]FDG PET. Subsequently, a 3-dimensional elliptic or circular volume of interest was drawn closely around the anatomic substrate on a CT image of the metastasis to generate the SUVmax. To calculate the SUVmean in healthy background tissue, 16 different predefined anatomic locations with a fixed volume (ranging between 0.5 and 10 cm3) were placed in each patient. For comparison between uptake in tumor and healthy tissue, the SUVmax of the tumor was matched with the SUVmax of the predefined background location within the same organ or a nearby structure whenever this was not possible (i.e., not enough tissue without tumor available or measuring uptake in a nonmalignant lymph node). This correction was done to account for the variation in physiologic 89Zr-trastuzumab uptake between patients and organs observed previously (7,9).
Qualitative Whole-Body HER2 PET Evaluation
Qualitative whole-body HER2 PET evaluation involved visual assessment of all scans by experienced nuclear medicine physicians. The assessment and central review of the scans were performed through an online central reviewing system designed by the Center for Translational Molecular Medicine translational research IT or Syngo.via VB20/30 imaging software (Siemens Healthineers). A HER2 PET scan was considered visually positive when all or the dominant part of all tumor load identified on baseline [18F]FDG PET and contrast-enhanced CT had visual uptake unequivocally higher than physiologic uptake in the liver (9). Brain metastases were considered HER2-positive when their uptake exceeded brain background uptake, allowing clear identification of the metastases.
Statistical Analysis
Descriptive statistics were applied for baseline characteristics. When the results were normally distributed, continuous variables were expressed as mean ± SD; otherwise, the median was reported. Categoric variables were expressed as numbers and percentages. More details on quantitative HER2 PET evaluation, the whole-body heterogeneity of 89Zr-trastuzumab uptake in metastases, and the development of an algorithm to predict biopsy HER2 positivity from HER2 PET information are provided in the supplemental materials (supplemental materials are available at http://jnm.snmjournals.org) (18,19).
The specificity, sensitivity, positive predictive value, and negative productive value of the qualitative whole-body HER2 PET assessment to assess the HER2-positive or -negative immunohistochemistry of the biopsied metastasis were calculated. CIs for the whole-body qualitative analysis were determined with the Wilson method (20).
Statistical significance was defined as a P value of 0.05 or less based on 2-sided tests not corrected for multiple testing. Statistical analyses were performed using SPSS Statistics version 23 (IBM Corp.) for Microsoft Windows and R version 4.2.2 for Apple macOS.
RESULTS
Patients and Metastasis Biopsies
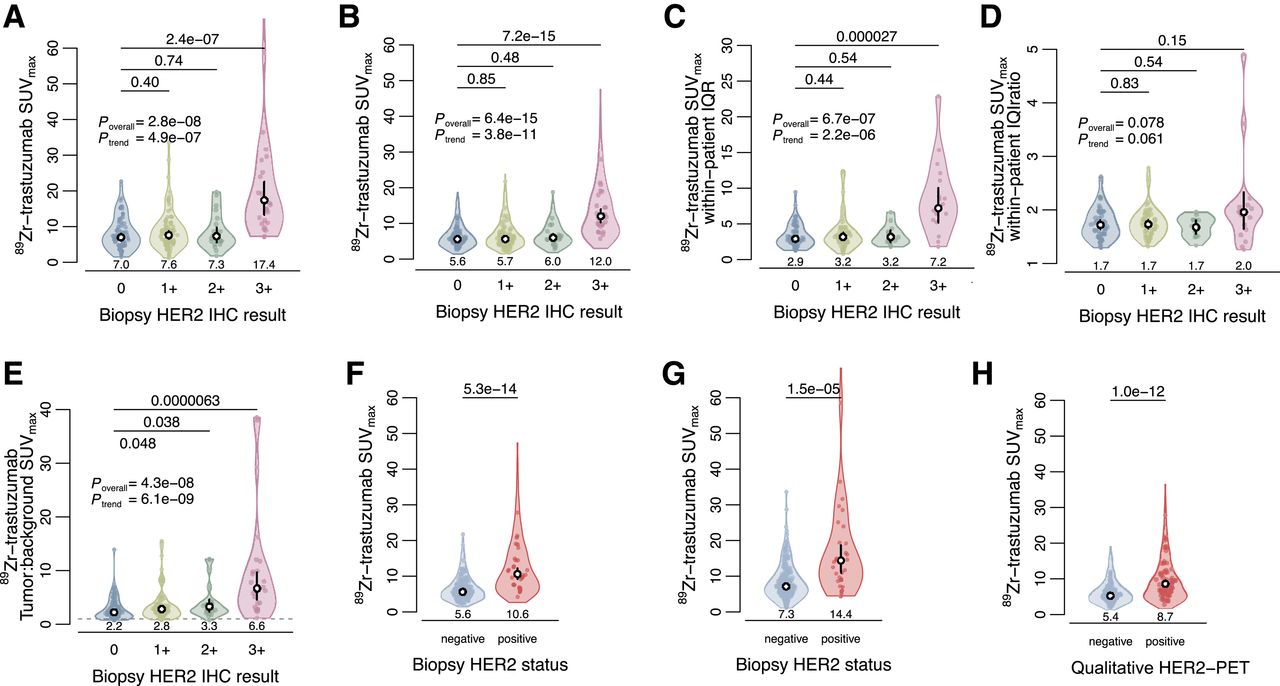
In 189 of 200 enrolled patients, HER2 expression in a biopsied metastasis could be compared with qualitative whole-body HER2 PET and quantitative 89Zr-trastuzumab uptake of any lesions. Patient and tumor characteristics from these 189 patients are shown in Table 1. In 186 of these 189 patients, biopsy results could be directly compared with local quantitative 89Zr-trastuzumab uptake in the corresponding biopsied metastasis (Fig. 1). From 186 biopsies, HER2 immunohistochemistry results were 0, 1, 2, or 3+ in, respectively, 71, 71, 20, and 24 patients, with a tumor geometric mean SUVmax of 7.0 (range, 6.0–8.0), 7.6 (range, 6.5–8.8), 7.3 (range, 5.5–9.7), and 17.4 (range, 13.4–22.6) (Fig. 2A; P < 0.001 between an immunohistochemistry score of 0 and 3+). Most biopsies were performed within 14 d of the HER2 PET (77.8%). Five patients experienced a temporary hypersensitivity reaction after 89Zr-trastuzumab tracer administration, for which 3 received steroids.
Baseline Characteristics (189 Participants)

Flow diagram showing patients included in IMPACT-MBC study and eligible for this analysis. **Necrotizing granulomatous inflammation in axillary lymph node.

89Zr-trastuzumab uptake absolute values and geometric mean by HER2 result. (A) Violin plot of tumor SUVmax according to HER2 immunohistochemistry status for 186 biopsied lesions in 186 patients. (B) Violin plot of tumor SUVmax according to HER2 immunohistochemistry status, for all 5,163 lesions in 189 patients. (C and D) Violin plot of within-patient variation in tumor SUVmax according to HER2 immunohistochemistry status based on within-patient interquartile interval as absolute difference (i.e., interquartile range [C]) or as ratio (i.e., 75th-to-25th percentile ratio [D]) for 128 patients with at least 10 measured lesions. (E) Violin plot of tumor-to-background SUVmax according to HER2 immunohistochemistry status based on 186 biopsied lesions in 186 patients. (F and G) Violin plot of tumor SUVmax according to biopsy HER2 status for all 5,163 lesions in 189 patients (F) or only 186 biopsied lesions in 186 patients (G). (H) Violin plot of tumor SUVmax according to HER2 PET scan assessment for all 5,163 lesions in 189 patients. Violin plots show either entire distribution (A, C–E, and G) or distribution with bottom and top 1 percentile omitted (B, F, and H). Colored dots within violin plots show either individual lesions (A, E, and G) or patient-level data (geometric means are shown in B, F, and H; other aggregation is shown in C and D). Values above x-axis and white dots in violin plots show geometric means per category, and vertical black lines show corresponding 95% CIs (A–H). P values comparing individual categories are based on independent-sample t tests (A, C–E, and G), Wald tests (B), or likelihood ratio tests (F and H) from linear mixed models taking clustering within patients into account using random intercepts. Overall P values are based on 1-way ANOVA (A, C–E) or likelihood ratio tests from linear mixed model (B). P values for trend are based on likelihood ratio tests from simple linear regression (A and C–E) or linear mixed model (B) evaluating HER2 immunohistochemistry categories as numeric variable. IHC = immunohistochemistry; IQR = interquartile range.
Whole-Body HER2 PET: Quantitative Evaluation
89Zr-trastuzumab uptake was quantified for 5,163 metastases in 189 patients (Fig. 3A). Lesions were located in bone (74.6%), lymph nodes (16.0%), lung (3.0%), liver (3.0%), breast (1.2%), and other sites (2.2%). 89Zr-trastuzumab uptake varied per anatomic location and size of metastases (Fig. 3B; Supplemental Fig. 1). The HER2 immunohistochemistry score correlated positively with the 89Zr-trastuzumab uptake of all metastases (Fig. 2B), as well as with biopsied metastases (Fig. 2A), regardless of lesion site and size (Supplemental Table 1).

Whole-body 89Zr-trastuzumab uptake absolute values and mean or geometric mean. (A) Overview of 89Zr-trastuzumab SUVmax at day 4 after injection in 5,163 tumor lesions in 189 patients grouped per HER2 immunohistochemistry status, visualizing tumor site and ordered by increasing geometric mean SUVmax per patient (horizontal bars). Delineated dots represent biopsied lesions. Gray dashed reference line depicts 90th percentile of SUVmax across all tumor lesions. *Lesion with SUVmax of 75.9. (B) Violin plot of SUVmax according to tumor site in 189 patients; number of lesions is according to site. (C) Violin plot of background SUVmean according to organ; number of patients is according to organ. Values above x-axis and white dots in violin plots show means (C) or geometric means (A and B) per category, and vertical black lines show corresponding 95% CIs (B, C).
The SUVmax of all metastases varied between 0.4 and 75.9 (10th–90th percentile, 3.0–14.6) and was heterogeneous within and between patients for all HER2 immunohistochemistry groups (Fig. 3A; intraclass correlation coefficient, 0.47). The within-patient heterogeneity of tumor SUVmax was larger for the groups with a metastasis immunohistochemistry score of 3+ than for the group with a score of 0 in an absolute (Fig. 2C) but not in a relative sense (Fig. 2D), based on the 128 patients with at least 10 metastases. Of note, 27.8% of patients with an immunohistochemistry score of 0 on biopsy had at least 1 metastasis exceeding the overall 90th SUVmax percentile of 14.6, which was 31.9%, 30.0%, and 84.0% for, respectively, the groups with immunohistochemistry scores of 1+, 2+, and 3+ (Fig. 3A). This could only partly be explained by differences in tumor uptake between locations (Fig. 3B).
In healthy background tissue, 89Zr-trastuzumab uptake varied per anatomic region, similar to metastases (Fig. 3C). The geometric mean tumor-to-background ratio based on SUVmax was higher with increasing HER2 immunohistochemistry score of the metastases, with also the HER2-low groups with an immunohistochemistry score of 1+ and 2+ being higher than the group with a score of 0 (Fig. 2E). This difference in 89Zr-trastuzumab uptake was more pronounced for HER2-low than -negative metastases when comparing it to the non–background-corrected uptake (Fig. 2A). The geometric mean tumor SUVmax was higher for HER2-positive than -negative immunohistochemistry disease at the patient and biopsied-metastasis levels (respectively, Figs. 2F and 2G).
Diagnostic Performance of Algorithm to Predict HER2 Positivity of Biopsied Metastasis
With the prediction algorithm (details are provided in the supplemental materials), the discriminative value of HER2 PET to predict the HER2 status of a metastasis had an area under the curve of 0.85 (95% CI, 0.77–0.92) when 89Zr-trastuzumab uptake in the biopsied metastasis was standardized for lesion site. The area under the curve improved slightly to 0.86 (95% CI, 0.79–0.93) after standardization for site and size (Supplemental Figs. 2A–2C). The algorithm was well calibrated, albeit with some uncertainty (Supplemental Figs. 2B and 4). Compared with the prediction algorithm, the 89Zr-trastuzumab uptake (SUVmax) of the biopsied metastasis without standardization for site or size predicted HER2 status in the corresponding metastasis with a lower area under the curve of 0.76 (95% CI, 0.66–0.85; Supplemental Fig. 2A).
Whole-Body HER2 PET: Qualitative Evaluation
With qualitative evaluation, whole-body HER2 PET was negative in 130 (69%) patients and positive in 59 (31%) patients. Qualitatively positive HER2 PET scans had a higher geometric mean tumor SUVmax than qualitatively negative scans (Fig. 2H). The sensitivity of the qualitative scan assessment to predict the HER2 status of the biopsied metastasis was 81% (95% CI, 63%–93%), specificity was 78% (95% CI, 71%–85%), positive predictive value was 42% (95% CI, 34%–51%), and negative productive value was 95% (95% CI, 91%–98%) (Table 2). Asymptomatic brain metastases were detected during qualitative evaluation on HER2 PET and confirmed with MRI in 4 patients. Three had a HER2 immunohistochemistry score of 3+, and 1 had a score of 1+. In this latter patient, the brain metastasis was clearly visible on HER2 PET (Fig. 4).
Correspondence of Qualitative Whole-Body 89Zr-Trastuzumab-PET and HER2 Status of Biopsied Metastases

Imaging examples. (Top row) Brain metastasis detected by MRI (performed because of HER2 PET findings), [18F]FDG PET, and HER2 PET in patient with HER2-negative disease (metastasis biopsy immunohistochemistry score, 1+) showing 89Zr-trastuzumab uptake in frontal right brain metastasis. (Bottom row) Bone metastasis in left femur detected by [18F]FDG PET and HER2 PET in patient with HER2-negative disease (metastasis biopsy immunohistochemistry score, 1+) showing 89Zr-trastuzumab uptake.
On this basis, a flowchart for the probability of HER2 positivity based on HER2 PET for clinical application was designed (Fig. 5).

Flowchart for probability of HER2-positive disease based on HER2 PET. *Supplemental Figure 3. aNegative productive value, 95%. bPositive predictive value, 42%.
DISCUSSION
In this prospective multicenter study, baseline HER2 PET was performed on patients with newly diagnosed HER2-positive, -low, and -negative MBC. HER2 PET had good diagnostic performance in determining HER2 positivity in the metastasis. Furthermore, HER2 PET identified HER2-positive metastases in HER2-negative disease and HER2-negative metastases in HER2-positive disease. In addition, HER2 PET uptake exceeded background uptake in HER2 immunohistochemically low and even negative metastases. This is in line with profound whole-body HER2 heterogeneity already in untreated MBC previously regarded as HER2-positive as well as -negative.
This is the largest prospective series assessing the diagnostic performance of HER2 PET in patients with HER2-positive, -low, and -negative breast cancer, as determined by immunohistochemistry of a metastasis biopsy. Our study design included a representative group of patients of the general nonrapidly progressive MBC population, mainly comprising patients with HER2-negative disease.
Tracer uptake in background tissue was as expected, given the known physiologic presence of HER2 expression in healthy cells (21,22). However, we observed that tumor uptake exceeded background uptake also in HER2-negative and -low disease. The recent European Society for Medical Oncology guideline states that it is still unclear whether HER2 expression is strictly required for trastuzumab-deruxtecan to be active or whether other factors may be implicated in its activity against tumors lacking HER2 overexpression or ERBB2 amplification (23). However, the findings in our study, with uptake exceeding background even in HER2-negative and -low disease, suggest that tumor-specific responses can be elicited by HER2 targeting of these MBC entities (5,24,25). In addition, the lesions with very high uptake (nearly 40% of metastases of patients with HER2-low and -negative disease) are likely to respond to antibody-drug conjugates and can also induce bystander effects (4). Our findings are in line with HER2 whole-body heterogeneity observed in a postmortem study of patients with alleged HER2-negative MBC (26). Remarkably, HER2 heterogeneity also affects patients with HER2-positive disease, with low uptake in the nonbiopsied metastases. This indicates that biopsy HER2 status does not, by definition, correspond to whole-body targetable HER2 (25–27). We hypothesize that this low uptake also corresponds to nonresponse, which is currently being evaluated. HER2 PET results could, therefore, potentially be applied in future studies as a refined biomarker to identify relevant treatment populations for novel HER2-targeting strategies. Whole-body HER2 heterogeneity could potentially be used to select patients for novel therapies to reduce unwarranted toxicity and costs by selecting those patients with 89Zr-trastuzumab uptake despite HER2-negative or -low disease.
Our study had limitations. In most patients, in line with current guidelines, a single biopsy was available to assess HER2 status, and therefore, whole-body HER2 heterogeneity observed on HER2 PET was not confirmed with immunohistochemistry on multiple tumor biopsies. Prior adjuvant trastuzumab treatment could have theoretically influenced whole-body HER2 heterogeneity as most patients with HER2-positive disease in this study were treated with trastuzumab in the first-line setting. The fact that we did not include patients with rapidly progressive disease could hamper the generalizability of our results. Regarding the technique, the assessment of HER2 PET is complex compared with other standard-of-care PET scans because of the background and size-dependent uptake, which precludes defining a universal threshold. Although we developed a prediction algorithm to address this concern, external validation is preferable before further implementation. Administering the 89Zr tracer with 50 mg of cold trastuzumab, based on our previous dose-finding study (7), allowed discrimination of metastases with a HER2 immunohistochemistry score of 3+ from the others, but whether this is the optimal dose in HER2-low disease, in light of aspecific uptake (28), remains to be studied further. Furthermore, other smaller-compound tracers targeting HER2 with lower blood-pool activity such as those labeled with 68Ga might be better suited to distinguish HER2-low from -negative disease (29,30). We observed a few mild hypersensitivity reactions to the tracer, and these reactions match the known safety profile of trastuzumab. The strengths of this study are the nationwide multicenter design, the standardization of all imaging, including tracer manufacturing, histopathologic procedures and protocols, and the central review of metastasis biopsies and HER2 PET scans. This all supports the validity of our findings. Furthermore, our study included a representative, homogeneous group of patients with the first presentation of MBC, including, as expected, mainly patients with HER2-negative disease. Our recommendations on how to interpret HER2 PET in clinical practice are shown in Figure 4.
CONCLUSION
The present study shows that HER2 positivity can adequately be assessed with HER2 PET when a biopsy cannot be safely obtained. Furthermore, this study increases insight into whole-body HER2 expression, showing considerable heterogeneity in HER2-positive, -low and -negative MBC. These findings support the reconsideration of a single-biopsy-based HER2 status as standard and may ultimately contribute to optimal patient selection for novel HER2-targeting strategies.
DISCLOSURE
The Dutch Cancer Society grant IMPACT (RUG 2012-5565) funded the study. Bert van der Vegt reports expertise or scientific advisory board/consultancy (on request) for Visiopharm, Philips, MSD/Merck, and Daiichi-Sankyo/AstraZeneca and speaker’s fee from Visiopharm, Diaceutics, and MSD/Merck. All honoraria are to UMCG, and all were outside the submitted work. C. Willemien Menke-van der Houven van Oordt reports speaker’s fee from Novartis, Eli Lilly, and Pfizer; travel fees from Daiichi; and institutional financial support for clinical trials or contracted research grants from AstraZeneca, Byondis, Pfizer, and GE, all outside the submitted work. Elisabeth de Vries reports institutional financial support for advisory boards/consultancy from NSABP, Daiichi Sankyo, and Crescendo Biologics and institutional financial support for clinical trials or contracted research grants from Amgen, Genentech, Roche, Servier, Regeneron, and Crescendo Biologics, all outside the submitted work. Carolina Schröder reports institutional support for clinical trials or unrestricted research grants from Pfizer, Seagen, Siemens, Roche, and Gilead, all outside the submitted work. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the diagnostic performance of HER2 PET to assess the HER2 status of a metastasis biopsy, and how does it evaluate whole-body heterogeneity in HER2-negative, -low, and -positive MBC?
PERTINENT FINDINGS: In this prospective multicenter study, HER2 positivity could be adequately assessed with HER2 PET in MBC, using an algorithm incorporating lesion size and site. Furthermore, considerable whole-body HER2 heterogeneity in HER2-positive, -low, and -negative breast cancer was demonstrated, with high HER2 PET uptake (in nonbiopsied metastases) in one third of patients with a HER2-negative or -low metastasis biopsy.
IMPLICATIONS FOR PATIENT CARE: HER2-positive disease on HER2 PET can support clinical decisions, particularly when a biopsy cannot be safely performed. HER2 PET heterogeneity in HER2-positive but also HER2-negative and -low disease could be a potential biomarker for novel HER2-targeting strategies and urges reconsideration of the current single-biopsy-based HER2 status.
ACKNOWLEDGMENTS
We thank all patients, the DSMB, and all research personnel who made this study possible. The IMPACT BREAST consortium includes Frederike Bensch, Suzanne van Es, Bertha van Essen-Eisses, Jorianne Boers, Jasper J.L. van Geel, Geke A.P. Hospers, Carolina P. Schröder, Elisabeth G.E. de Vries, Andor W.J.M. Glaudemans, Adriënne H. Brouwers, Johan R. de Jong, Erik F.J. de Vries, Marjolijn N. Lub-de Hooge, Annelies Jorritsma, Martijn den Dekker, Theo Kok, Thomas Kwee, Ton Velleman, Monique Dorrius, Gonda de Jonge, Shekar Mahesh, Jelle Overbosch, Mieke Zwager, Bert van der Vegt, Erik Buskens, Truuske de Bock (UMCG); Evelien J.M. Kuip, Sarah Verhoeff, Carla van Herpen, Eline Boon, Winette T.A. van der Graaf, Jolien Tol, Wim Oyen, Lioe-Fee de Geus-Oei, Eric Visser, Otto Boerman, Marcel Janssen, Anne I.J. Arens, Katja van Rij, Peter Bult (Radboud University Medical Center); Erik J. van Helden, Sophie L. Gerritse, C. Willemien Menke-van der Houven van Oordt, Henk M.W. Verheul, Otto S. Hoekstra, Marc C. Huisman, Guus Van Dongen, Ronald Boellaard, Daniëlle J. Vugts, Daniela E. Oprea, Ben G.J.C. Zwezerijnen, N. Harry Hendrikse, Ellis Barbé (Amsterdam University Medical Center location VUMC); Lindsay Angus, Agnes Jager, Stefan Sleijfer, Jaco Kraan, Astrid A.M. van der Veldt, Jasper Emmering, Özgül Ekmekcioglu, Anieta Siewerts, John Martens (Erasmus Medical Center); and Sjoerd G. Elias and Karel G.M. Moons (UMC Utrecht).
Footnotes
Published online Sep. 5, 2024.
- © 2024 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 19, 2024.
- Accepted for publication July 10, 2024.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.