


Abstract
P664
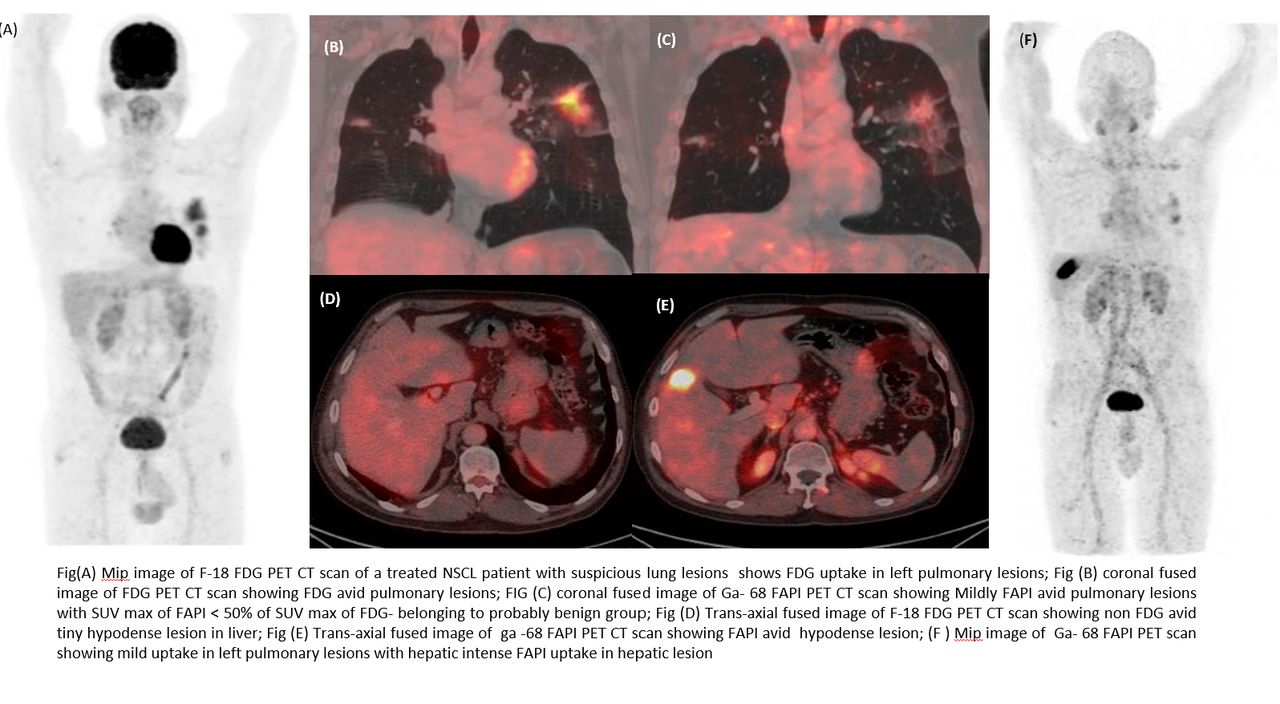
Introduction: F18-FDG PET-CT scan is now the stranded imaging modality for tumor detection. Its major disadvantage is that it is not a tumor specific agent which leads to false positive and false negative findings. We aim to look for the utility of Ga68 FAPI-46 (fibroblast activation protein inhibitor) PET-CT scan in these patients. Additionally, we tried to look for the utility of dual tracer study to differentiate benign from malignant pathologies.
Methods: All the patients who had doubtful mass lesion on conventional imaging to differentiate benign from malignancy, proven metastatic cervical lymphadenopathy with unidentified primary, for staging in proven primary malignant pathology, suspicion disease recurrence on conventional imaging, suspicious recurrence on FDG PET-CT scan were included in this study. All these patients underwent Ga 68 FAPI PET-CT scan.
Results were grouped into 4 categories based on quantification marker SUV max (maximum standard uptake value). Category I: high likely benign (FDG positive, FAPI negative (ve-) or both negative(ve-) ); Category II : Probably benign (both positive but the SUV max of FAPI is < 50% of SUV max of FDG; Category III: indeterminate significance (both positive with SUV max of FAPI ranging from 50-70 % of SUV max of FDG), Category IV: high likely malignant (both positive with SUV max of FAPI ≥70% FDG SUV max or only FAPI positive). Histopathology or follow-up imaging served as the standard for the final diagnosis.
Results: Of 30 patients with indeterminate FDG PET-CT scan findings 14, were treatment naïve and 16 had suspicious disease recurrence.
All the treatment naïve 14 patients had a total of 32 lesions detected on ether of the scans. 10/32 (31%) lesions were in "likely benign group" and all of them turned out to be true negative (ve-). 16/32 (50%) lesions were in "likely malignant group" and all were true positive. The "probably benign group" having 3/32 lesions (9%) were proved to be benign and of the 3/32 (9%) remaining lesions belonging to indeterminate group, 1/3 turned out to be tubercular pathology and rest 2/3 were diagnosed as malignant
FAPI PET-CT scan alone could detect primary lesion in 3/14 (~21%), suspicious lesions as benign in 3/14(~21%), down staged in 4/14 (28%) and upstaged in 1/14(~7%) patients; further dual tracer study reduced false positive rate in 2/14 (~14%) patient. Rest 1 /14 (7%) patient was true positive in both the scans.
All the 16 patients being evaluated for suspicious recurrence showed a total of 30 lesions. All the 9/30 (30%) of "likely benign group" turned out to be true negative, 7/30 (23%) of "likely malignant group" were all true positive. The remaining 10/30(33%) lesion in "probably benign category" also proved to be non-malignant and out of 4/30 (13%) lesions in "indeterminate group" 3/4 were tubercular in pathology and 1/4 had non-specific infection.
FAPI PET -CT scan alone detected true recurrence in 3/ 16 (~19%) patients and prevented false positive in 4/16 (~25%); however dual tracer study additionally prevented false positive cases in 5/16 (~31%) patients. 2/16 (12.5%) patients with belonged to "indeterminate group" turned out to be tubercular in pathology. Rest 2/16 (~12.5%) were true recurrence in both.
Conclusions: Ga 68 FAPI PET -CT scan do have additional great advantage in reducing false negative and positive rate in various oncological scenarios pertaining to solid tumors. However, careful evaluation of may be challenging in some cases. We found that dual tracer study may help in differentiating benign vs malignant in these settings to a substantial extent. Our major limitation is the low study population; so additional studies with larger population groups are further required.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.