


Abstract
P607
Introduction: Radium-223 (223Ra) and Lutetium-177–Prostate-Specific Membrane Antigen (177Lu-PSMA) both prolong overall survival (OS) in different metastatic castration-resistant prostate cancer (mCRPC) settings. The observational, retrospective study, RALU, investigated safety and clinical outcomes of sequential 223Ra/177Lu-PSMA therapy in patients (pts) with mCRPC. This post hoc analysis of RALU investigated the safety and clinical effectiveness of 177Lu-PSMA treatment in pts with mCRPC with and without visceral metastases who had received prior 223Ra.
Methods: Retrospective data were collected from German nuclear medicine centres for all pts who received 177Lu-PSMA and who were previously treated with 223Ra therapy (pts were treated between Dec 2014 and Jul 2021). Eligible pts were males aged ≥18 years, with a confirmed diagnosis of mCRPC, who had received ≥1 dose of 223Ra and, in any subsequent therapy line, ≥1 dose of 177Lu-PSMA. Groups included in this analysis were pts with or without visceral metastases prior to 177Lu-PSMA.
Results: At baseline, prior to 177Lu-PSMA therapy, 36 pts had visceral metastases and 97 had no visceral metastases. Of pts with visceral metastases, 50% had liver involvement. Of pts without visceral metastases, 65% had bone and lymph node metastases and 34% had bone metastases without lymph node metastases. Baseline characteristics for pts with and without visceral metastases, respectively, were: median ages of 75 and 73 years; 61% and 62% with Eastern Cooperative Oncology Group performance status (ECOG PS) 1, 39% and 38% with ECOG PS 2; median prostate-specific antigen (PSA) values of 421 and 265 ng/ml, and median alkaline phosphatase (ALP) values of 117 and 146 U/L. Overall, 72% of pts with and 52% of pts without visceral metastases had received ≥4 life-prolonging therapies before starting 177Lu-PSMA; all pts had received prior 223Ra. Prior life-prolonging therapies in pts with visceral metastases were abiraterone (72%), enzalutamide (78%), docetaxel (86%) and cabazitaxel (33%); corresponding values for pts without visceral metastases were 71%, 66%, 70%, and 19%. Overall, 50% of pts with and 51% of pts without visceral metastases received ≥4 177Lu‑PSMA cycles, respectively.
From 177Lu-PSMA start to ≤30 days post-last dose, 83% with and 77% of pts without visceral metastases had treatment-emergent adverse events (TEAEs) of any grade; TEAEs (any grade; excluding laboratory abnormalities) seen in ≥10% of pts were dry mouth (25%, 11%, respectively) and nausea (11%, 8%, respectively). Grade 3–4 TEAEs occurred in 25% and 30% of pts with and without visceral metastases, respectively.
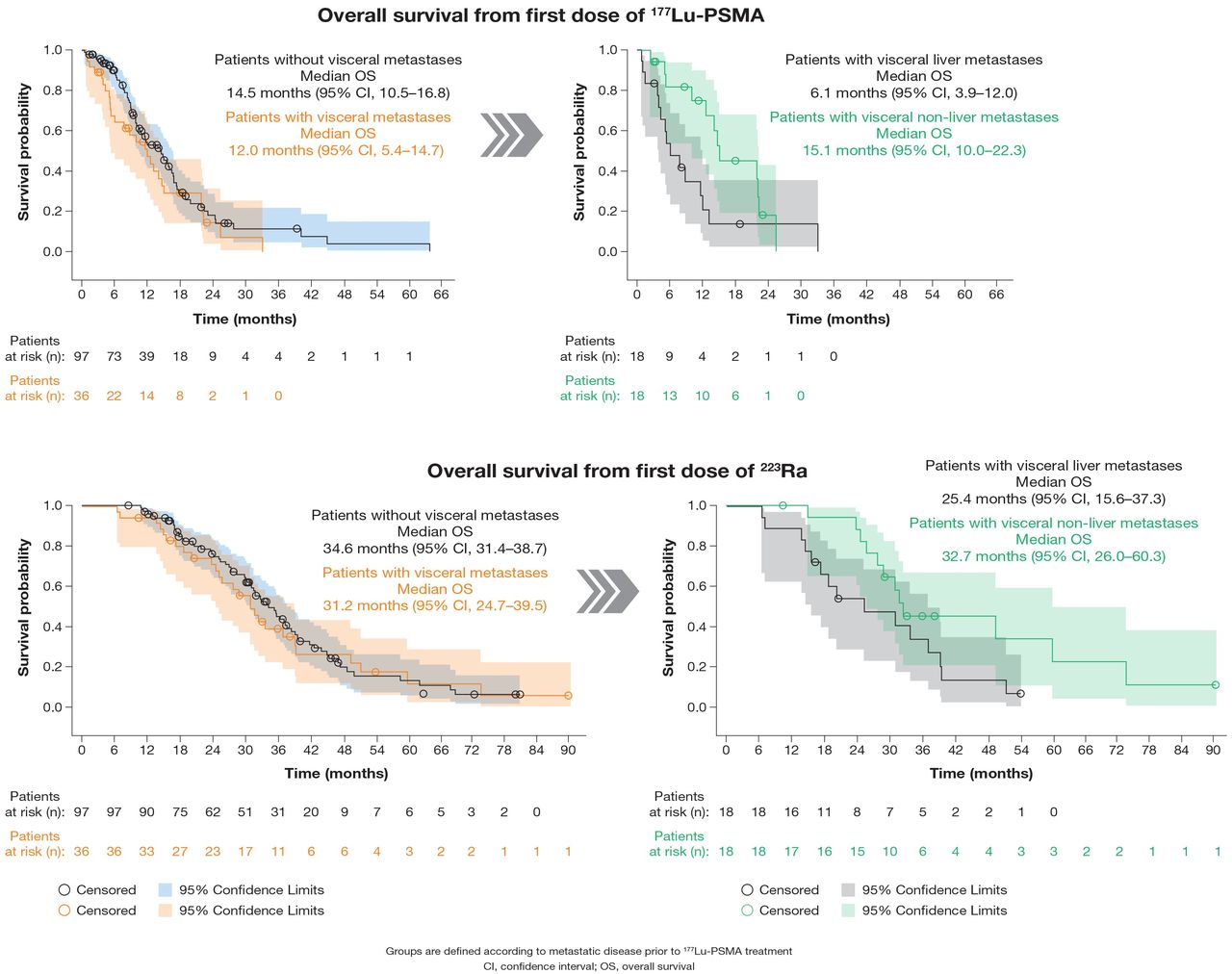
Median OS from start of 177Lu-PSMA was 12.0 months (mo) (95% confidence interval [CI], 5.4–14.7) in pts with visceral metastases and 14.5 mo (95% CI, 10.5–16.8) in pts without (Figure). However, in pts with visceral metastases, median OS was shorter in those who had liver involvement than in those who did not (6.1 mo [95% CI, 3.9–12.0] vs 15.1 mo [95% CI, 10.0–22.3]) (Figure). Median OS from start of 223Ra was 31.2 mo (95% CI, 24.7–39.5) in pts with visceral metastases and 34.6 mo (95% CI, 31.4–38.7) in pts without (Figure). During 177Lu-PSMA therapy, best PSA responses of ≥10%, ≥30%, and ≥50% were seen in 50%, 50%, and 50% of pts with visceral metastases and 59%, 46%, and 39% of pts without, respectively. ALP declines of ≥10%, ≥30%, and ≥50% were seen in 46%, 9%, and 0% of pts with and 44%, 22%, and 11% of pts without visceral metastases, respectively.
Conclusions: In this real-world setting of pts with mCRPC who received sequential treatment with 223Ra and 177Lu-PSMA, the safety profile of 177Lu-PSMA was similar in pts with visceral metastases compared with those without. As expected, survival was the longest in pts without visceral disease and the shortest in patients with liver metastases.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.