


Abstract
P1175
Introduction: The bone marrow (BM) represents the main organ-at-risk for 177Lu-PSMA radiopharmaceutical therapy of prostate cancer. The patient-specific active BM distribution is difficult to image, making dosimetry for BM a time-consuming and challenging process due to complicated quantitative measurements that include various contributors to the absorbed dose. The aim of this study was to assess and compare BM dosimetry using blood-based, image-based, and whole-body skeleton (WBS)-based methods for patients treated with 177Lu-PSMA-617.
Methods: Nineteen patients (4 without bone metastases (b-mets), 6 with high burden of b-mets) were included. The injected activity was 7.40±0.74 GBq for each treatment cycle. SPECT/CT scans were performed at 24 and 48 h post injection (p.i.) to estimate the organ biodistribution. Three blood samples were collected at 15 min p.i., and 15 min before each of the SPECT/CT scans to evaluate the BM self-dose using the blood-based method (DBM <-blood) by considering bi-phase clearance kinetics. The self-dose was also calculated using two imaging methods. (i) First, small VOIs (1 cm diameter) located at patient lumbar vertebrae (L1-L4), femora and humeri, while trying to avoid b-mets,were drawn to estimate the BM self-dose (DBM <-img). (ii) For the second imaging method, i.e. WBS-based method, two regions of WB low-uptake in the skeleton (luWBS) were used to evaluate the BM self-dose (DBM <-luWBS). Those luWBS regions were defined based on the WB skeleton with < 1% (luWBS-1%) and 0.5% (luWBS-0.5%) of the whole body activity uptake. Cross-dose contributions from high uptake organs (i.e. kidneys, salivary glands, spleen and liver) (DBM<-organs), and remainder of the body (ROB) (DBM <-rob) were further estimated based on whole organ and WB segmentation. Lastly, the total BM dose (DBM) was calculated by summing the self-dose and cross-dose contributions. Values obtained with different methods were compared.
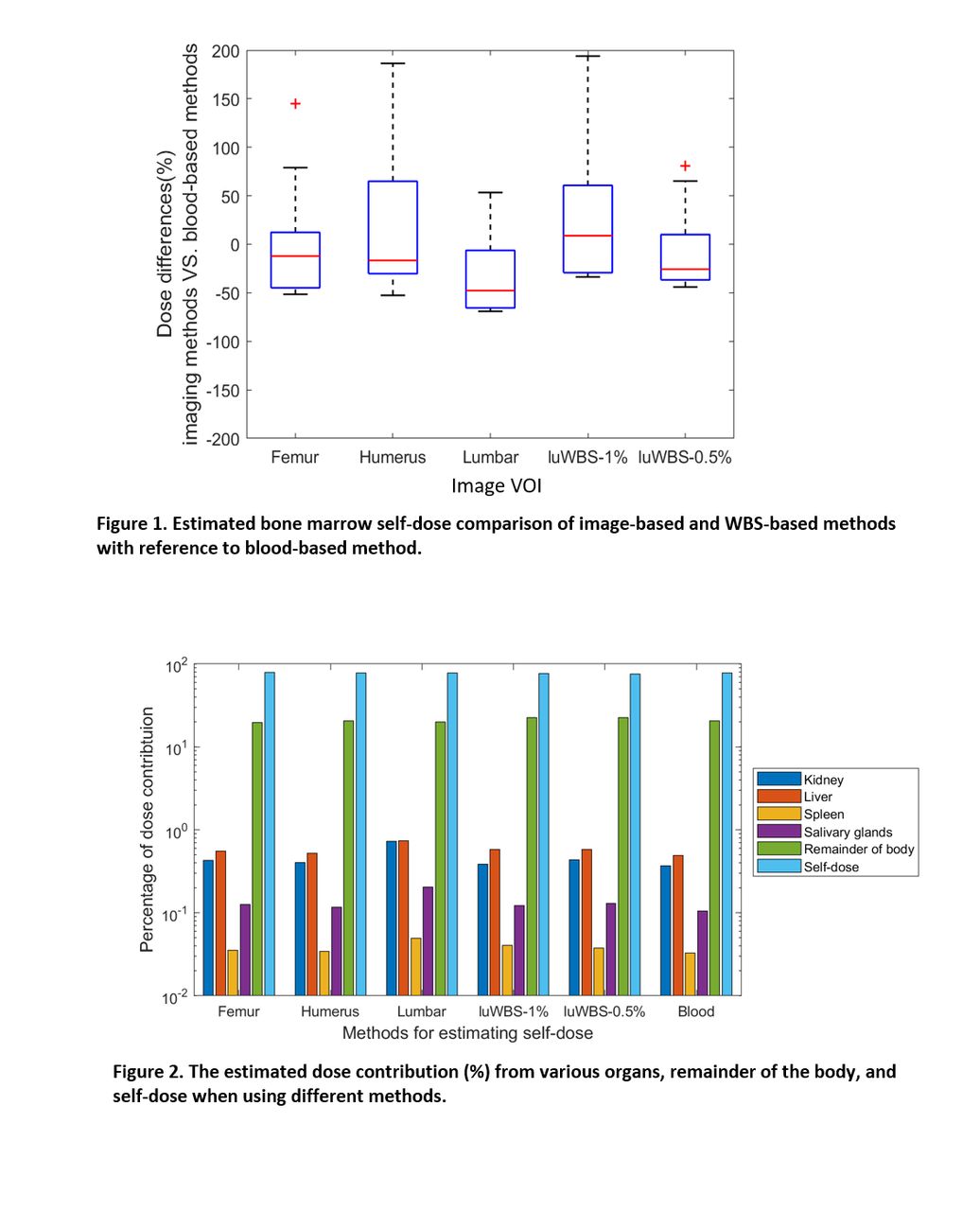
Results: The BM self-dose from the image-based method highly depended on the localization of the different VOIs. The differences of DBM <-img(L1-L4), DBM <-img(femur), DBM <-img(humerus) against DBM <-blood were -31.6±43%, -3.6±57% and 17.6±70%. Although large variations were observed, the femur could potentially be considered as an alternative for self-dose estimates when blood samples are not present (especially as most b-mets were either close or located on lumbar region). DBM <-luWBS-0.5% showed a lower variability against DBM <-blood with a difference of -8.3%±37%, while DBM <-luWBS-1% differed by -23.4%±62%. WBS with <0.5% of WB uptake should be considered for BM dose calculation and provided more comparable results than those from the regions with small volumes. Considering the cross-dose contributions, >90% of cross-doses were from DBM <-rob, because of the high tumor burden being included in the ROB. DBM <-rob and accumulated activity uptake of total tumor burden were found to have a correlation coefficient of 0.73 with high significance (p<0.005). The total cross-dose contribution accounted for 21.7±12% of total BM dose.
Conclusions: Patient-specific bone marrow dosimetry was performed and compared using different approaches. Our results suggest that using VOIs in the femur or taking the BM luWBS-0.5% lead to small deviations when compared to blood-based methods. However, efforts to reduce the variability of image-based methods still need to be further developed.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.