


Abstract
The Highlights Lectures at the closing sessions of SNMMI Annual Meetings were originated and presented for more than 30 y by Henry N. Wagner, Jr., MD. Beginning in 2010, the duties of summarizing selected significant presentations at the meeting were divided annually among 4 distinguished nuclear and molecular medicine subject matter experts. The 2022 Highlights Lectures were delivered on June 14 at the SNMMI Annual Meeting in Vancouver, Canada. This month we feature the lecture by Andrei Iagaru, MD, Professor of Radiology–Nuclear Medicine at Stanford University School of Medicine (CA) and Chief of the Division of Nuclear Medicine and Molecular Imaging at Stanford HealthCare, who spoke on general nuclear medicine highlights from the meeting. Note that in the following presentation summary, numerals in brackets represent abstract numbers as published in The Journal of Nuclear Medicine (2022;63[suppl 2]).
Welcome to my favorite part of the SNMMI Annual Meeting, the Highlights Lectures. I want to begin by briefly noting the outstanding work that has been done in nuclear medicine to address issues generated by the COVID-19 pandemic. Our community continues to contribute to the management of these patients through SPECT/CT, PET/CT, and novel imaging techniques. We are also an integral part of the larger effort to expand knowledge about the virus and its short- and long-term effects. A few of the notable presentations at this meeting include those by: Melhem and Keu from the Université de Montréal and the Hôpital Cité-de-la-Santé (Laval, both in Canada), who reported on “SPECT VQ and CTPA agreement for diagnosis of pulmonary embolism during the COVID-19 pandemic: a single-institution experience” [2793]; Khandelwal et al. from the Sanjay Gandhi Postgraduate Institute of Medical Sciences (Lucknow, India), who reported on “A prospective study to investigate the implementation of semiquantitative inflammatory load in post-COVID-19 lung disease to strategize therapy” [2326]; Wang et al. from the University of California–Davis, who reported on “Multiorgan metabolic changes in COVID-19 recovery measured with total-body dynamic 18F-FDG PET” [2329]; Maldonado et al. from University Hospital Quironsalud (Madrid, Spain), who reported on “Molecular imaging PET/CT in oncologic patients with unsuspected asymptomatic infection with SARS-CoV-2: the Spanish experience (Delta and Omicron variants)” [2330]; and Callaud and Bailly from Centre Hospitalier Universitaire Tours and Centre Hospitalier Régional Orléans (both in France), who reported on “Time-reduction for simultaneous dual-isotope lung scintigraphy using 3D-ring CZT SPECT/CT” [2789]. Although time restrictions require that I move on to other topics, I want to congratulate these authors and researchers for the great work they are doing.

Andrei Iagaru, MD
CHANGING PERSPECTIVES IN NUCLEAR MEDICINE AND MOLECULAR IMAGING
The theme this year for this lecture is “How can we look at the same radiopharmaceutical or disease or scan and see things so differently?” This is somewhat analogous to the different perspectives that artists may take on their subjects. The same bowl of fruit would have been presented in radically different ways by, for example, Dalí and Picasso. What we do in nuclear medicine and molecular imaging is art in a different form. We are able to identify what happens in patients and to select tools from our armamentarium that allow us to provide increasingly detailed diagnoses. These tools vary and are continuously replaced by newer and more effective approaches, just as the ways in which we define and understand disease change with growing scientific understanding and experience. Let’s look at some examples from this year’s SNMMI Annual Meeting presentations.
PEDIATRIC IMAGING
My distinguished colleague at Stanford, Helen Nadel, MD, reminds us often that “imaging children is not like imaging small adults.” With adult patients, we often think of digital scanners as enabling faster exams and perhaps higher throughput—a perspective reflecting our work as busy clinicians. In pediatrics, digital scanners also offer the opportunity to reduce administered radiopharmaceutical dosage. Alves et al. from the Cincinnati Children’s Hospital Medical Center (OH) reported on the “Feasibility of reduced count acquisition of whole-body 18F-FDG PET in children and young adults imaged with a digital PET scanner” [2384]. The SNMMI Pediatric Imaging Council recognized Dr. Alves with their Majd–Gilday Young Investigator Award for this work. These researchers looked at various simulated acquisition times (60, 55, 50, 45, 40, and 30 s/bed) for pediatric patients who underwent imaging on a 5-ring 25-cm axial-field-of-view PET/CT system. Reconstructed images were scored on several criteria, including overall image quality, by pediatric radiologists. The resulting data indicated that no qualitative impact was observed down to almost 55 s/bed, suggesting the potential for faster scans with lower radiation (up to 67%) and for reduction or elimination of sedation/anesthesia in some patients. The authors summarized their finding that “for children and young adults receiving 0.12 mCi/kg injected activity of 18F-FDG and imaged with a state-of-the-art extended-field-of-view digital PET/CT system, an acquisition time of 60 s/bed (or 0.8 mCi/kg injected activity imaged at 90 s/bed) shows no significant impact in image quality or quantitative measures.”
In a similar approach with a different scanner, Zhang et al. from the Ohio State University Wexner Medical Center (Columbus), the University of Pennsylvania (Philadelphia), and the University of Cincinnati (OH) reported on “Feasibility of low-dose 18F-FDG PET in pediatric oncology” [2387]. This study evaluated low-dose PET via an intraindividual comparison using both data simulation and actual scan validation. Body mass index (BMI)–adapted 18F-FDG administration was proposed and validated. This approach showed a 30%–70% dose reduction for pediatric imaging and up to 92% reduction for infants and small children, without compromising image quality and SUV quantification. Figure 1 shows comparisons of whole-body 18F-FDG PET in children with different BMI values. Lesions were identifiable across all reconstructed datasets, and equivalent image quality was maintained with robust semiquantitative measurements. Pediatric patients deserve not only the lowest achievable dose from CT (about which we have heard much more) but also from PET, and it is clear that with advances in technology this can be achieved.

Feasibility of low-dose 18F-FDG PET in pediatric oncology. Comparison of whole-body imaging in pediatric patients (BMI = 17, top row of images, and 26, bottom row) at (far left) actual full-dose scan (180 s/bed) and (left to right) simulated reduced doses (range, 33%–92% reduction). Lesions are identifiable across all PET datasets, and equivalent image quality was maintained with robust SUV quantification achieved with substantial 18F-FDG dose reduction.
Is it possible to look at lymphoma and see things quite differently from different perspectives? Some imaging physicians believe that 18F-FDG PET is the best approach. MR experts believe that diffusion-weighted (DW) imaging with MRI is best. Baratto et al. from Stanford University (CA), Children’s Hospital of Philadelphia (PA), and Yale University (New Haven, CT) reported on these perspectives by “Comparing 18F-FDG PET/MRI and DW MRI for staging and restaging of Langerhans cell histiocytosis (LCH) in children” [2386]. In the study, 23 children and young adults with biopsy-proven LCH underwent simultaneous 18F-FDG PET/MRI with DW MRI (n = 20) or sequential 18F-FDG PET/CT plus DW MRI (n = 3), including 23 baseline scans and 16 follow-up scans after chemotherapy. Comparing SUV semiquantitative data on PET and mean apparent diffusion coefficient map data from MR, they found highly similar accuracy, specificity, and sensitivity in staging and restaging LCH. This tells us that in order for PET/MRI to be more widely adopted in routine practice, we need to shorten the duration of these exams. Patients with multifocal LCH are usually very young and will require multiple follow-up imaging throughout their lives. PET/MRI in pediatric patients makes perfect sense, because substituting MRI for the CT removes one portion of the radiation dose and the high quality of the PET component lowers the other. This raises several questions: How do we make it faster? Do we really need all the MR sequences? If not, which ones are needed? These authors showed that it is possible to optimize PET/MR workflow in a way that can make it faster and perhaps more widely available and used.
What perspectives can PET and MRI provide in differentiating posttransplant lymphoproliferative disorder (PTLD) from lymphoma? Jayapal et al. from the Lucile Packard Children’s Hospital at Stanford School of Medicine (CA) reported on “Predictive patterns of pediatric PTLD on PET/MRI” [2786]. In this retrospective study, the authors identified unique patterns of whole-body 18F-FDG PET/MRI metabolic activity in 38 children with PTLD. In 17 of the 21 (81%) patients with PTLD with abnormal PET/MRI but without transformation to lymphoma, a characteristic pattern of diffuse and symmetric uptake with involvement of symmetric lymph node stations was noted (Fig. 2). Asymmetry in this pattern seemed to predict transformation to lymphoma. As the authors concluded, “these findings may help the clinician in patient management to determine need for biopsy and therapy versus continued observation.” Management and treatment decisions diverge significantly over time after transplantation depending on this diagnostic differentiation. Looking for this imaging symmetry provides a different and very useful perspective in this setting.

Predictive patterns of pediatric posttransplant lymphoproliferative disorder (PTLD) on PET/MRI. Assymmetry in lymph node involvement on PET/MRI correlated with progression to lymphoma. (A) 7-y-old boy after heart transplant with diffuse nonnodal and asymmetric pattern with renal, bone, and spinal cord lesions with B-cell lymphoma; and (B) 16-y-old girl after stem cell transplantation with symmetric nodal pattern of PTLD.
In the oncology world, we are familiar and experienced with sodium fluoride for evaluation of bony metastases. Unfortunately, we are not always reimbursed for these studies, so the use of sodium fluoride has diminished over time. Paravastu et al. from the National Institutes of Health (Bethesda, MD) and the Foundation for Research and Technology Hellas (Heraklion, Greece) reported on “Quantitative analysis of 18F-NaF PET/CT imaging: evaluation of denosumab treatment in fibrous dysplasia” [2771]. These authors looked at potential utility of the tracer in predicting responses to treatment, and the resulting images were exquisite (Fig. 3). With data from SUVmax, SUVmean, and total lesion activity changes from baseline to 6 mo posttreatment in 8 patients with fibrous dysplasia, they showed that successful treatment with denosumab was associated with a marked reduction in bone turnover, as quantified by 18F-NaF PET/CT. Findings like these have the potential to open new incentives for reintroduction of sodium fluoride in wider clinical use. As a community we should not be intimidated by repeated denials from the Centers for Medicare & Medicaid Services and should work together to obtain appropriate coverage that could benefit a range of patients.

Quantitative analysis of 18F-NaF PET/CT evaluation of denosumab treatment in fibrous dysplasia (FD). (A) Maxillary lesion in patient with monoostotic FD. (B) Marked improvement visualized by 18F-NaF PET/CT after 6 mo treatment. (C and D) Representative images of treatment response on 18F-NaF PET/CT in 2 patients with polyostotic FD.
Our perspectives on radiopharmaceuticals often depend on our practice settings. I am accustomed to seeing 18F-FDOPA, for example, from the glioma/brain tumor/motion disorder viewpoint, because it is the main referral pattern at my institution. In pediatrics, the focus with this radiopharmaceutical is on congenital hyperinsulinism. Navarantha et al. from Children’s Hospital of Philadelphia (PA) asked “18F-FDOPA PET imaging in congenital hyperinsulinism [CHI] for localization of a focal pancreatic lesion: do medications interfere with radiotracer uptake?” [2388]. Patients with CHI who are unresponsive to initial insulin secretion medication undergo genetic testing to predict the focal form, as well as 18F-FDOPA PET imaging to localize focal pancreatic lesions. Current imaging protocols call for discontinuation of CHI medications for 2 d before the scan. Evaluating imaging and other results with a variety of relevant medications, the authors showed that the most common drugs administered to CHI patients do not seem to interfere with pancreatic uptake of 18F-FDOPA. Even with glucagon, which produced differences in head-to-liver SUV ratios, no differences were noted in pancreatic uptake. This is important and useful information that we can all take home and use clinically if we have access to 18F-FDOPA.
Sathya Murthi et al. from Manchester University Hospitals and the Christie Hospital (both in Manchester, UK, and part of the National Health Services Trust) reported on the “Role of 18F-DOPA PET/CT in suspected CHI” [2392]. These authors compared uptake values of focal lesions detected with 2 different reconstruction techniques to identify the superior reconstruction method. After initial visual assessment by physicians, focal lesions were assessed by semiquantitative analysis of SUVratio of focal disease (SUVmax in lesion/SUVmean of pancreatic tissue) and by SUVratios calculated using both ordered-subset expectation maximization (OSEM) and ultra-high definition (UHD) reconstructions. They concluded that 18F-DOPA PET/CT with contrast-enhanced CT had high sensitivity in focal lesion detection (95.2%), resulting in successful surgical and clinical outcomes offering complete cure. They noted that this avoids potential long-term complications of total pancreatectomy. The finding that the UHD reconstruction method may be superior to OSEM reconstruction in this setting makes the case that we should not be reluctant to embrace new technologies that clearly improve patient care.
WIDENING PERSPECTIVES
Obesity is a well-recognized health risk. Nuclear medicine and molecular imaging tools have potential to provide meaningful information to these patients. Bini et al. from Yale University/Yale University School of Medicine (New Haven, CT) reported on “Liver and brain levels of 11β-hydroxysteroid dehydrogenase type 1 (11β-HSD1) enzyme in obesity: preliminary results from PET imaging studies” [2801]. 11β-HSD1 catalyzes the conversion of inactive cortisone to active cortisol. In this study, 9 individuals (ages, 29–64 y) with a range of BMIs (22.6–34.4 kg/m2) underwent PET/CT imaging with arterial sampling after injection of 18F-AS2471907, a novel PET tracer for 11β-HSD1. The preliminary results suggested that obesity is associated with increased levels of 11β-HSD1 in the liver but decreased levels in the brain (although aging may increase brain 11β-HSD1 levels). They noted that additional studies are needed to clarify the correlation of brain and liver 11β-HSD1 with obesity. This has clear implications for obesity treatment strategies, including those associated with nonalcoholic fatty liver disease.
Obesity was also the focus of work by Muzik and Jiang from the Karmanos Cancer Institute at Wayne State University (Detroit, MI), who reported on “Decreased sympathetic innervation of cold-activated brown and white fat [BAT and WAT, respectively] in obese subjects using 11C-HED PET imaging” [2238]. They investigated the relationship between sympathetic innervation and energy expenditure in both BAT and subcutaneous/visceral WAT in a group of obese and lean subjects during cold exposure. All patients underwent 11C-HED and 15O2-water PET imaging at rest and after exposure to mild cold (16°C). In addition, 18F-FDG images were obtained during the cold stress condition to assess the presence of activated BAT. Relative measurements of daily energy expenditure under both baseline and cold stress were obtained. They found that whole-body energy expenditure decreased in obese subjects during cold as a result of decreased sympathetic innervation (blood flow) in subcutaneous WAT, suggesting that the primary function of WAT in obese individuals is insulatory and not heat generating. This is an example of a new tracer that can be applied to a clinical question for which answers have direct implications for both understanding the physiology of a widespread health challenge and for potential therapeutic interventions.
At this meeting we have heard about applications of fibroblast-activation protein inhibitor (FAPI) in almost every possible indication—it has gone from being a pan-cancer tracer to a pan-disease agent. Song et al. from Wuhan Union Hospital and Tongji Medical College of the Huazhong University of Science and Technology (both in Wuhan, China) reported on “Noninvasive visualization of liver fibrosis with 68Ga-labeled FAPI” [2234]. The authors of this interesting study addressed an unmet need: identifying the presence of liver fibrosis early in the course of the disease so that we can consider ways to arrest or slow progression. In addition to reporting on serial 68Ga-DOTA-FAPI-04 imaging in a mouse model of progressive liver fibrosis, the authors showed related imaging in humans. Figure 4 illustrates correlations between 68Ga-DOTA-FAPI-04 uptake and histology in 5 example patients with escalating degrees of fibrosis. The authors concluded that this tracer “has the potential to display activated fibroblasts involved in the fibrotic process and to assess different stages of liver fibrosis…with promising applications in the accurate assessment and potential prediction of the prognosis of liver fibrosis.” The next question is whether, now that we have a tracer to assess progression in liver fibrosis, we can change the course of the disease? Perhaps we will hear more about this at future meetings. It is remarkable that this tracer, developed for cancer imaging for which it was recognized as the 2019 SMMMI Image of the year, was again the focus of the 2022 Image of the Year, this time for predictive cardiac assessments. We are seeing it applied in an extraordinary number of other new applications by our community to improve patient care.

Noninvasive visualization of liver fibrosis with 68Ga-DOTA-FAPI-04. Example correlations between 68Ga-DOTA-FAPI-04 uptake and histology in 5 example patients with (left to right) escalating degrees of fibrosis.
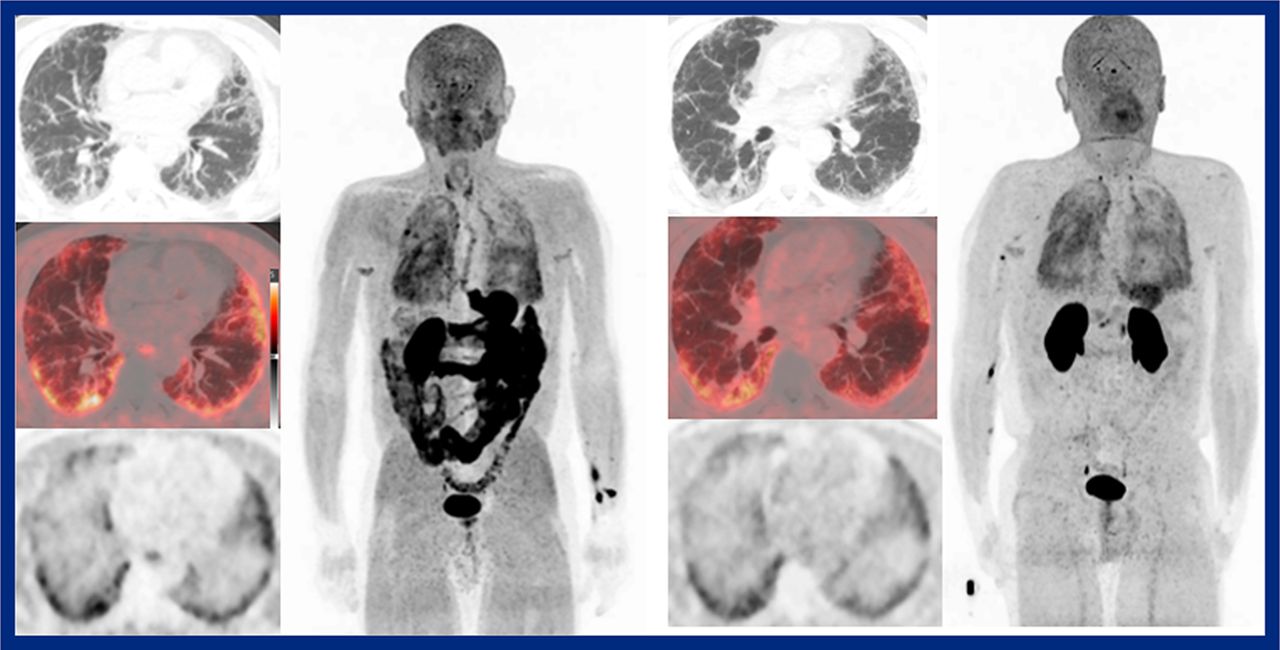
Wardak et al. from Stanford University/Stanford University School of Medicine (CA), Pliant Therapeutics (South San Francisco, CA), and Invicro, LLC (Boston, MA) reported on “Phase 2 drug target engagement study of PLN-74809 in patients with idiopathic pulmonary fibrosis (IPF) using a novel αvβ6 cystine knot PET imaging tracer” [2236]. The aim of this study was to evaluate the in vivo αvβ6 receptor occupancy of PLN-74809, an oral small-molecule dual-selective inhibitor of integrins αvβ6 and αvβ1, as assessed by [18F]FP-R01-MG-F PET/CT. This cystine knot radiopharmaceutical was originally developed for cancer. However, its target is not so much the cancer cells themselves as the tumor-associated fibrosis, making it a logical candidate for assessing pulmonary fibrosis. The authors compared kinetic modeling of uptake pre- and postdrug administration in IPF lungs to assess drug target engagement. They found that not only could target engagement of PLN-74809 with αvβ6 integrin receptors in the lungs of IPF patients be quantified using [18F]FP-R01-MG-F2 PET/CT imaging (Fig. 5), but that PLN-74809 achieved a dose-dependent target engagement of up to 98% in the lungs of these patients. These preliminary data provide insights into the potential mechanism and clinical benefits of PLN-74809 as an antifibrotic therapeutic in IPF. This is also an example of the important role our field can play in working with the pharmaceutical industry to apply new markers to advance development of novel treatments.

Imaging PLN-74809 in patients with idiopathic pulmonary fibrosis (IPF) with a novel αvβ6 cystine knot PET tracer. Example [18F]FP-R01-MG-F PET/CT images acquired at baseline (left) and after administration of the antifibrotic drug (right). PET/CT enabled target engagement of PLN-74809 with αvβ6 integrin receptors in the lungs of IPF patients, showing dose-dependent target engagement of up to 98%.
Wilks et al. from Massachusetts General Hospital/Harvard Medical School (Boston, MA) reported on “PET imaging of neutrophil trafficking fungal infection” [2511]. Imaging infection and the immune system was the focus of much interest at this year’s meeting, again an area of unmet needs. These authors have designed a neutrophil precursor cell line that can be expanded ex vivo and transfused into neutropenic subjects to allow them to successfully combat fungal infections. In this study, they quantified the kinetics of these infused cells using PET imaging in healthy and neutropenic mice. With an 89Zr-labeled agent, they were able to track exogenous neutrophils quantitatively and noninvasively in healthy, ablated, and fungal-infected mice for up to 7 d after infusion. Lower splenic uptake was observed in Candida-exposed animals, suggesting an active immune response to fungal infections. This work opens the door not only to enhanced understanding of the response of specific elements of the immune system to infections (fungal and bacterial) but also to development and optimization of neutrophil transfusion therapies in neutropenic patients. We look forward to seeing associated clinical data in the not-too-distant future.
Tremendous interest across all scientific and technical tracks at this meeting continued to focus on total-body PET imaging. In his Cassen Lecture, Simon Cherry, PhD, told us that it is only a matter of time until total-body PET is even faster, and the images his group is producing are truly remarkable. In one of these studies, Omidvari et al. from the University of California Davis/University of California Davis Medical Center (Sacramento), Imperial College (London, UK), and ImaginAb (Inglewood, CA) reported on “Total-body imaging of CD8+ T cells in patients recovering from COVID-19: a pilot study using the uEXPLORER total-body PET” [2327]. Their goal was to obtain an in vivo quantitative measure of tissue distribution of CD8+ T cells by imaging with 89Zr-Df-crefmirlimab-berdoxam, a minibody with high affinity to human CD8. In this pilot study, they aimed to quantify pathophysiologic changes in CD8+ T cell distribution in patients recovering from COVID-19 to illuminate the immunologic response and role of T cells in COVID-19 morbidity and immunity. The authors should be congratulated on the beautiful images they were able to acquire up to 48 h after submillicurie (0.5 mCi) doses (Fig. 6). This imaging resulted in high definition of the expected distribution of T cells in lymphoid organs and derivation of high-quality Patlak parametric maps, along with a preliminary observation that recovering COVID-19 subjects in the study had higher T cell mass than controls. They concluded that “This study makes a compelling case to explore such in vivo functional aspects of T cells across a wide range of COVID-related conditions, vaccine response, and in clinical immunologic research in general, using the unique tools that total-body PET provides.”

Imaging CD8+ T cells in patients recovering from COVID-19. 89Zr-Df-crefmirlimab-berdoxam total-body PET with the uEXPLORER, showing SUV maximum-intensity projection images at (left to right in each image set) 30–90 min, 6–7 h, and 48–49 h in a post-COVID patient (left set) and a control subject (right set). High-definition tracking of T cell distribution in lymphoid organs was achieved, with a preliminary observation that recovering COVID-19 subjects had higher T cell mass than controls.
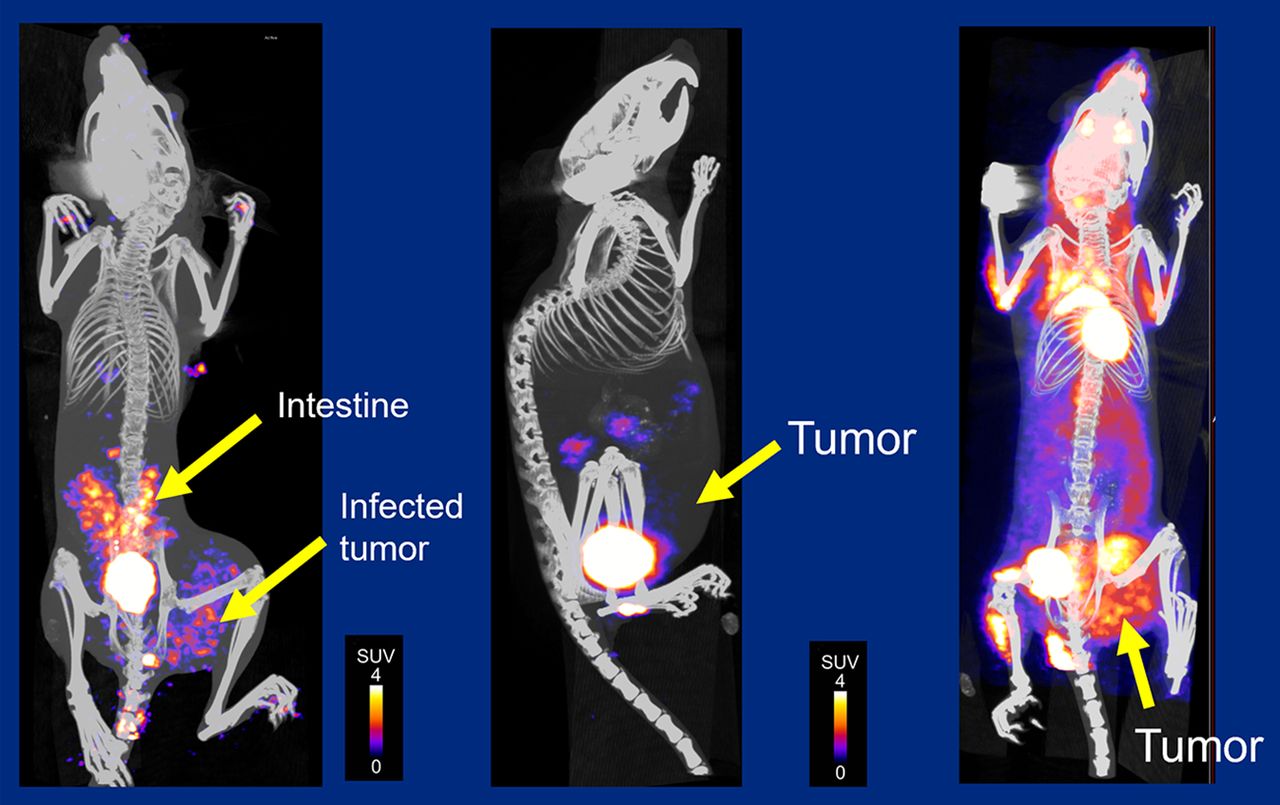
Tumor-targeting bacteria are being investigated as therapeutic tools for solid tumors, and PET may have a role in the development and translation of these agents by providing data to confirm localization and proliferation of bacteria at the tumor site and to monitor off-target effects. Ordoñez et al. from T3 Pharmaceuticals AG (Basel, Switzerland) and Johns Hopkins University School of Medicine (Baltimore, MD) reported on “Imaging tumor-targeting bacteria using 18F-fluorodeoxysorbitol [18F-FDS] PET” [2510]. This is an interesting application of the concept of bacteria targeting. They evaluated in a murine model whether 18F-FDS PET could accurately monitor colonization of breast cancer tumors by a genetically modified strain of Y. enterocolitica (T3P-Y004) that is currently being evaluated for clinical trials. The researchers found that PET was able to differentiate sites of bacterial infection with low background in most organs, including the tumor site (Fig. 7). They concluded that “given that 18F-FDS is available for clinical use, bacteria-specific PET could be a valuable tool to support the development and implementation of tumor-targeting bacteria therapeutics.”

Imaging tumor-targeting bacteria in a mouse model using 18F-FDS PET. PET was able to differentiate sites of bacterial infection with low background in most organs, including the tumor site (left and right) compared with uninfected controls (middle), pointing to the potential for other applications of bacteria-specific PET to support development of tumor-targeting bacteria therapeutics.
From a very different but no less important global perspective, Giammarile et al. from the International Atomic Energy Agency (IAEA; Vienna, Austria) reported on “The IAEA Quality Management Audits in Nuclear Medicine Practices (QUANUM) program: a practical tool for quality audits in nuclear medicine” [2776]. A key question as we leverage the power of aggregated data from clinical trials throughout the world is: How do we ensure that the quality of what we do and the protocols we use are similar and consistent? Through QUANUM, the IAEA supports implementation of effective quality systems while integrating all aspects of quality management into modern nuclear medicine services in its member states. The QUANUM program provides a tool to perform independent quality audits of nuclear medicine departments through comprehensive reviews of organizations and their clinical practice, as well as offering multidisciplinary team site visits. In their report, the IAEA authors described integration of the program in 73 nuclear medicine centers in 46 countries and detailed outcome analyses of the impact on practice quality. This is an important take home message for all of us: We need quality programs using protocols that can be reproduced from one institution to another, so that we all speak the same language about reports and images from our patients.
Another area increasingly emphasized by SNMMI and very important to all of our clinical practices and trials is that of diversity and representation. How do we make sure that the research we do is representative of the populations we serve? How do we encourage enrollment of patients who reflect the diversity of the areas in which we practice? Badawi et al. from the University of California Davis (Sacramento) reported on “Diversifying the subject cohorts in total-body PET research: a feasibility study” [2780]. In this pilot effort, the uEXPLORER group targeted trial recruitment of healthy subjects from underrepresented racial/ethnic groups in their catchment area. They consulted with their community advisory board to review existing trial/treatment publicity material for inclusivity and arranged for TV and radio spots, advertisements, and news articles. The result was more than 155 inquiries, and the underrepresented recruitment goal was met. This study offers a template for outreach and recruitment in studies that aim to be more representative of the diversity of the local community.
CONCLUDING THOUGHTS
I will end with an editorial thought: my own perspective on all these perspectives. As the saying goes, “the stone age did not end because humans ran out of stones”; similarly, the age of photomultiplier tubes did not end for lack of photomultiplier tubes. It ended because industry, academia, and private practice put a great deal of effort into continued innovation and clinical adoption. I am confident that the end of the age of planar imaging in general nuclear medicine will not come about because of a lack of standard scanners. It will be because the technology has advanced, so that we do not need to do planar all the time—we will have protocols adapted to target the specific organ of interest or to survey the whole body. As a community, we should strive to be early adopters. We should not be so busy with what we do on a routine basis that we fail to see the benefits of new technologies. I believe that we will continue to see new and even more innovative ways through which general nuclear medicine contributes to the advancement of both our field and the wider world of medical knowledge and health care.
Footnotes
Published online Apr. 13, 2023.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.