


Visual Abstract

You don’t understand anything until you learn it more than one way.
—Marvin Minsky (1927–2016)
Living organisms maintain homeostasis through dynamic multiorgan systemic interactions (1). Considerable energy is needed to fuel these interactions to promptly orchestrate multiple organs to respond to perturbations (allostatic load) (2). For example, inflammation in response to infection or tissue damage is a critical survival mechanism to return to the original homeostatic state. In the case of ill-compensated systemic feedback loops (allostatic overload), persistent disruptions in baseline homeostasis may occur, which gives rise to chronic diseases such as arthritis, cancer, cardiovascular disease, or diabetes (3). These pathologies can, in theory, be characterized by deviations in parameters that describe a normative multiorgan network and that extend beyond their usual range.
Molecular imaging modalities such as PET can provide valuable insights into the underlying homeostasis of living subjects using target-specific radiotracer imaging (4). After the commercial inception of PET, most of its clinical investigations focused on imaging with a single-organ field of view (FOV) (cardiology and neurology). With the introduction of a whole-body (WB) acquisition mode—that is, the successive translation of the subject through the axial FOV of a PET system with slightly overlapping bed positions (5)—the identification of hypermetabolic tumor lesions in oncology patients became the primary application of PET. Such a reductionist “lumpology” approach (6), however, caused a wealth of molecular information available from PET to be overlooked and the concept of human physiology imaging to be discarded.
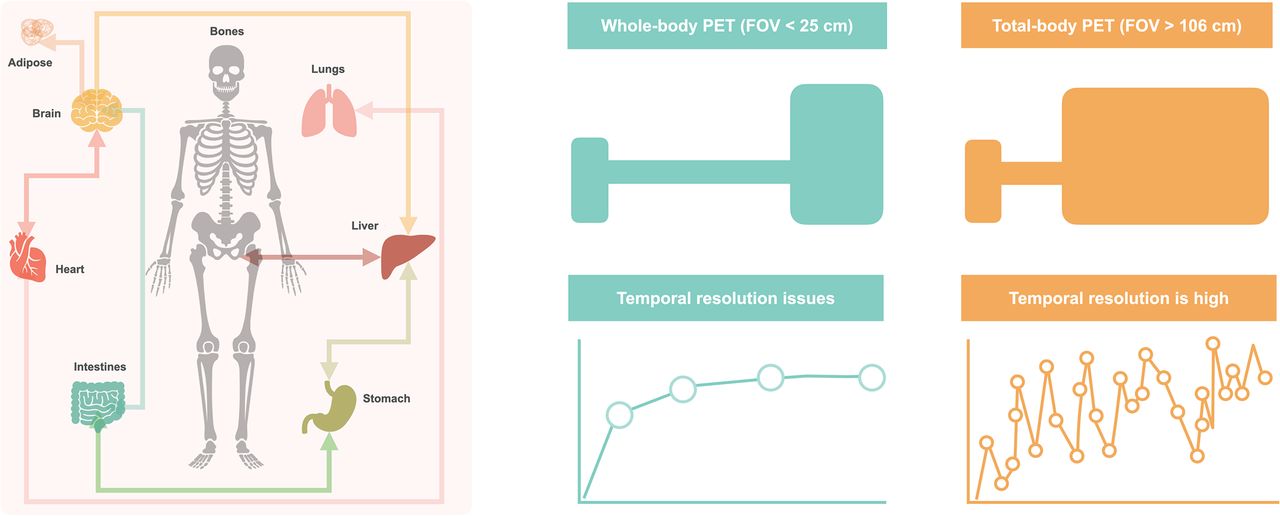
The recent extension of the WB PET concept to extended axial-imaging ranges with larger-FOV systems, colloquially referred to as total-body (TB) PET, has sparked interest in the PET community to conduct multiorgan systemic investigations. TB PET systems cover axial scan ranges of 1 m (7,8) to 2 m (9), allowing synchronous measurement of signals from multiple organs. In addition, the richness of the multiorgan data derived from WB PET notwithstanding (10,11), TB PET is particularly unique as it satisfies 2 critical criteria for such causal investigations: the simultaneous acquisition of signals from multiple investigated distant organs and a high temporal resolution across the FOV (12). The combination of increased sensitivity and subsecond temporal sampling (13) provided by TB PET could potentially aid in probing real-time multiorgan interactions (Fig. 1).

Thanks to markedly increased performance, TB PET allows assessment of multiple organs synchronously, giving way to noninvasive exploration of systemic, interorgan interactions.
MULTIORGAN ANALYSIS WITH STANDARD WB PET
Traditional WB PET with an axial FOV of about 20 cm can already be used for multiorgan analysis. For example, simple intergroup comparisons of organ-based SUV can provide crucial information on the underlying pathology. A recent study demonstrated that in a patient cohort with resected breast cancer, a high metabolic tumor volume and increased spleen glucose metabolism at baseline were associated with poor 5-y recurrence-free survival (14). That study hinted toward a possible interaction between the tumor and the host immune system through upregulation of hematopoiesis. Diseases formerly conceived as focal, such as myocardial infarction, have distributed effects throughout the body that are mediated through disease-specific networks (15). And finally, mental and societal stress triggers have been linked to various diseases associated with chronic inflammation that can already be assessed by WB PET (16).
INTERORGAN NETWORKS THROUGH PET
Current multiorgan network investigations using WB or TB PET are mostly fishing expeditions aiming to pinpoint stable correlations between organs (10,11). In general, correlation analyses explore gross systemic effects between 2 groups without causal explanation. When correlation analyses are performed, the chosen sample should represent the investigated population (e.g., healthy or pathologic) (17). Other factors, such as variability, linearity, and variance of the samples, must also be considered. Since most multiorgan correlation network studies seek to pinpoint monotonic relationships between investigated organs, Spearman correlation should be chosen over Pearson correlation, as the former is nonparametric and insensitive to the linearity and homogeneity of the variance of observed data.
The ultimate goal of interorgan analysis is to identify causal relationships between organs that can facilitate the development of impactful interventions in medicine. Here, structure learning of Bayesian networks (18) in combination with graph models as visual representations of causal links in complex processes can be an attractive approach (19), which, however, still mandates the integration of a clinical expert to denounce spurious causal links.
Both causal and correlation networks should be considered hypothesis-generating tools rather than tools that provide solid endpoints. Such hypotheses must be proven or disproven in rigorous validation studies (Fig. 2) in which investigators should be conscious of the confounders affecting the accuracy of SUV or kinetic parameters as part of a multiorgan analysis (20).

Categoric pathway to adopting WB or TB PET for exploring human connectome: several advanced and automated tools are required to extract robust data for hypothesis building and validation in translational setting. ECG = electrocardiography; EEG = electroencephalography; fMRI = functional MRI.
THE PROMISE OF TB PET
Despite the increasing installed base of TB PET systems, the number of studies that explore TB PET beyond dose reduction and higher throughput for the sake of assessing the human connectome studies is limited. Preliminary studies have demonstrated the potential of using the temporal domain, namely raw time–activity curves, to derive metabolic associations between different bone compartments (21) or to construct normative networks for healthy male and female controls (22). Although neither study explained causality, dynamic TB PET has the potential to create personalized causal networks from a single subject. Such a paradigm requires, however, the subject to be challenged by a task, pharmacologic intervention, or external stressor (e.g., pain or cold). By challenging (perturbing) the system, simultaneous or delayed changes in signals from different organs can be measured and used to establish causality.
For decades, such studies have been performed with functional MRI to derive effectivity connectivity by conducting baseline and task paradigms in a single imaging session (23). Recent innovative brain studies in functional PET have shown the possibility of using 18F-FDG PET to study dynamic changes in glucose metabolism within a single session with the aid of constant-infusion protocols (24). However, conducting such challenge-based studies is nontrivial in a TB PET setting, particularly in view of unknown response times and downstream interactions. Therefore, test studies on well-understood paradigms (25) should be performed before exploratory connectome investigations are conducted using TB PET.
ROAD MAP TO THE FUTURE: CONNECT TO THE CONNECTOME
To date, the PET imaging community is fragmented by vendor, geography, and skill set. There needs to be more meaningful sharing of code, data, and expertise to address the novel challenges and opportunities that arise with this technology. To fully leverage the potential of WB and TB PET alike for health care, new analysis methods are required, and new skills in the workforce are needed (Fig. 2). Automated data analytics pipelines, including automatic WB semantic segmentation (26) as well as WB and TB PET motion correction and spatial normalization, are prerequisites to robust TB PET connectome studies.
The community needs to be open to the repurposing of existing solutions (e.g., Statistical Parametric Mapping, version 12 (27)) and to be prepared to fail in this high-risk–high-gain approach to using PET far from the comfortable notion of a high-sensitivity lesion tracker. Fostering rigorous experiments to prove the validity of correlations and causalities while also sharing negative results must be encouraged. Also, rich data from healthy and pathologic cohorts should be pooled to amass large sample sizes that help us to better understand the actual distribution of the data and, therefore, to arrive at logical conclusions.
CONCLUSION
The introduction of TB PET offers unique opportunities to investigate multiorgan interactions—the organ connectome for understanding human physiology and pathology. Novel study protocols and paradigms, and translational research pipelines, will be required to support causal interpretations of interorgan relationships. As a community, we should unite to prioritize progress over our vanities. The same was said in the early days of PET/CT and PET/MRI, and it still holds true. Novel and open-minded collaborative efforts beyond the nuclear medicine comfort zone are required to unlock the power of WB and TB PET imaging. Adopting this concept requires significant personal and infrastructural investments; the concept may fail, but if it does not, it will benefit our patients and medicine at large.
DISCLOSURE
Research support was received from NIH R01CA29422, EraPErMED PETictCAC, and ANR-FWF I-6174B. No other potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENTS
We sincerely thank Irene Buvat (Paris), Ramsey Badawi (U.C. Davis), Simon Cherry (U.C. Davis), Terry Jones (U.K.), and Stefan Grünert (Vienna) for their continuous input and motivation.
Footnotes
Published online Dec. 2, 2022.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 6, 2022.
- Revision received November 17, 2022.





{kind=link}
{kind=link}
{kind=link}