


Visual Abstract

Abstract
We report the dosimetric evaluation of prostate-specific membrane antigen–based radioligand therapy (RLT) for metastatic prostate cancer in a patient with autosomal-dominant polycystic kidney disease. Methods: The patient received hemodialysis during each of 6 RLT cycles while staying as an inpatient. We used voxel dosimetry and blood sampling for the dose calculation. Results: The patient responded well to the RLT, as indicated by the prostate-specific antigen level decreasing from 298 to 7.1 ng/mL. The doses per cycle ranged from 0.19 to 0.4 Gy/GBq for the parotid gland, 0.14 to 0.28 Gy/GBq for the submandibular gland, 0.03 to 0.11 Gy/GBq per kidney, and 0.10 to 0.15 Gy/GBq for the red bone marrow. Conclusion: This case suggests that [177Lu]Lu-PSMA–based RLT can be applied successfully and safely to a patient with chronic kidney disease undergoing hemodialysis.
- chronic kidney disease
- kidney failure
- dosimetry
- 177Lu
- prostate-specific membrane antigen
- radioligand therapy
Prostate-specific membrane antigen (PSMA) is a glycoprotein with high expression on healthy prostate epithelial cells but is extremely upregulated in prostate cancer (1–3). This makes PSMA an ideal target for diagnostic and therapeutic applications. As a third-line treatment of metastatic castration-resistant prostate cancer, radioligand therapy (RLT) with [177Lu]Lu-PSMA-617 or analogs has proven to be effective, imparting substantial benefits for the overall survival of patients (4,5).
The international guidelines for PSMA-based RLT do not include recommendations for patients with comorbid chronic kidney disease (CKD), who need hemodialysis during RLT. In theory, impaired kidney function could alter the pharmacokinetics of the radiopharmaceutical. In this paper, we report on the treatment with [177Lu]Lu-PSMA-617 of a metastatic castration-resistant prostate cancer patient with comorbid stage 4 CKD according to the Kidney Disease: Improving Global Outcomes scale. His RLT was performed under a compassionate-use program. Apart from exploring the practical aspects of performing hemodialysis in a nuclear medicine ward, we present the organ dosimetry and effective half-life of [177Lu]Lu-PSMA-617 in the patient. To the best of our knowledge, this is the first description of radiation dosimetry for a CKD patient underdoing PSMA-based RLT.
MATERIALS AND METHODS
Informed consent was obtained from the patient presented in this brief communication.
Clinical Status of the Patient
A 63-y-old patient with metastatic castration-resistant prostate cancer was referred to our hospital for [177Lu]Lu-PSMA-617 RLT after all available options of first- and second-line treatments had been exhausted.
We established the indication for RLT on the basis of the high binding of the PSMA ligand [18F]F-PSMA-1007 in the metastases. During the 4 y before RLT, the patient had received hemodialysis 3 times per week because of CKD with autosomal-dominant polycystic kidney disease. Supplemental Table 1 reports the renal-function data before each RLT cycle (supplemental materials are available at http://jnm.snmjournals.org).
RLT Procedure with Hemodialysis
The patient underwent 6 RLT cycles at our department between October 2021 and August 2022. In each cycle, the patient received between 7.71 and 8.07 GBq of [177Lu]Lu-PSMA-617 (cumulative activity, 47.3 GBq), which was administered by intravenous injection. He stayed in the therapy ward for approximately 72 h after each cycle.
During the first RLT cycle, the patient received 3 hemodialyses while in the therapy ward. In the subsequent cycles, the patient maintained his regular hemodialysis schedule, corresponding to 2 hemodialyses during each ward visit (Table 1). With no access to treated water for dialysis at our facility, we replaced regular dialysis sessions with hemodiafiltration sessions using a Prismaflex device (Baxter International Inc.). We compensated for the lower clearance with an increased treatment time of 6.2–7.6 h, resulting in a clearance time per volume of 0.9 (6). The dialysate volume ranged from 40.3 to 57.0 L (Table 1). To assess the 177Lu clearance from the blood, we measured the radioactivity concentration in the blood samples collected at the beginning of every hemodialysis and before the patient was discharged from the clinic.
Therapy and Hemodialysis Data
Dosimetry
We performed the dose calculation for the organs at risk with the voxel dosimetry application of Hermes (Hermes Medical Solutions) (7) using SPECT/CT images (Siemens Healthineers Intevo Bold; medium-energy collimator, 128 × 128 matrix; Siemens Healthineers xSPECT reconstruction) acquired at 1, 2, 3, and 10 d after injection for 30 min of scan time in each session. A nuclear medicine resident physician segmented the parotid gland, submandibular gland, left colic flexure, and right kidney on the dose maps obtained from Hermes.
Following previous work (8,9), we used blood sampling to estimate the red bone marrow (RM) radioactivity dose. We opted for a Bayesian fit of a single-exponential function to the data (Gaussian likelihood, Gaussian priors of 0.1 ± 0.025 h−1 for a mean half-life and 0.89 ± 0.38 MBq/mL for the amplitude) to determine the time-integrated activity from which we performed the dose calculation according to previous data (8).
Radiation Protection
The therapy was conducted according to the standard radiation protection requirements for [177Lu]Lu-PSMA-617 (10). While the nurse performed the hemodialysis, we monitored the whole-body effective dose with an electronic personal dosimeter to assess the additional radiation burden (11). We measured the dose rate of the patient before each discharge from the clinic and instructed him to follow radiation protection measures according to the Swiss regulations (www.bag.admin.ch/str-wegleitungen). Furthermore, we advised the personnel routinely performing the hemodialysis to follow standard radiation protection measures outside the therapy ward for 9 d after injection (use of disposable gloves and exclusion of pregnant women from performing the hemodialysis). We measured the residual activity in the dialysate at the beginning and at end of each hemodialysis with a calibrated γ-counter.
RESULTS
Therapy
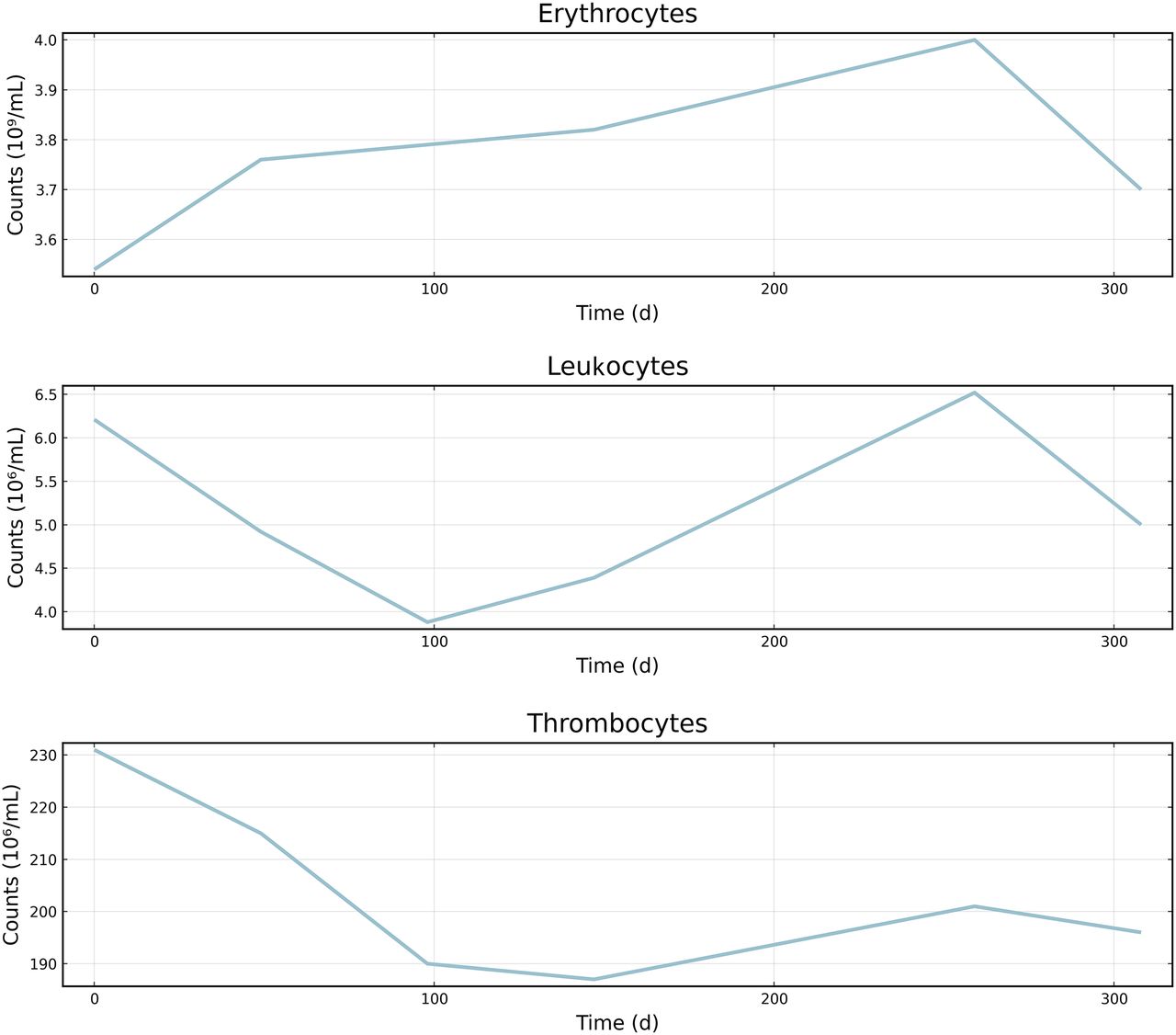
During each RLT, a nephrologist closely monitored the patient’s hemodialysis. The patient tolerated the [177Lu]Lu-PSMA-617 RLT well. There were no adverse events according to the Common Terminology Criteria for Adverse Events (https://ctep.cancer.gov/protocolDevelopment/adverse_effects.htm). The prostate-specific antigen trend indicated a good tumor response for up to 4 cycles, with serum prostate-specific antigen levels decreasing from 298 to 7.1 ng/mL. However, after a longer intercycle time of 16 wk between the fourth and fifth cycles (due to a global shortage of [177Lu]Lu-PSMA-617), the prostate-specific antigen values rose again to 157 ng/mL, suggesting a relapse of the prostate cancer. There were no abnormalities found in the blood cell count data (Fig. 1).

Time course of blood cell count data throughout 6 RLT cycles.
Dosimetry
We report the organ doses of the patient in Table 2 and illustrate them in Figure 2. We do not report the dose of the left kidney because of its vicinity to the left colic flexure, which showed a much higher value in the dose map. The activity in the blood samples and the fit predictions are shown in Supplemental Figure 1. The blood effective half-life by cycle ranged from 13.8 ± 2.3 to 17.5 ± 4.1 h; Supplemental Table 2 shows the complete fit results.
Doses for Organs at Risk for Each Therapy Cycle

Visualization of cumulative organs-at-risk doses to patient with corresponding dose limits according to European Association of Nuclear Medicine guidelines (10). We multiplied single-exposure dose limit of 2 Gy for RM by factor of 6 to reflect all therapy cycles.
Radiation Protection
The Prismaflex device was releasable from the controlled area immediately after the last hemodialysis because of the absence of detectable radioactive contamination. Therefore, only solid waste (i.e., tubing and dialysis fluid bags) showed detectable contamination with 177Lu and was placed in a decay storage room for safe disposal.
The dose rate at 1 m at chest height before the patient’s release (about 72 h after injection) ranged from 4.5 to 13.3 μSv/h. The individuals who performed the hemodialysis accumulated an effective dose between 8 and 42 μSv, which is consistent with previous results (11). For the first hemodialysis of each cycle, 24.8 ± 12.0 μSv were registered, whereas the hemodialysis performed 2 d after injection led to an effective dose of 12.7 ± 8.6 μSv. We report the radioactivity concentration in the dialysate medium at the beginning and at the end of each hemodialysis cycle in Table 1.
DISCUSSION
There is prior documentation of successful [177Lu]Lu-PSMA-617 treatment of patients with reduced renal function, including a dosimetric evaluation (12) and, more recently, a report on hemodialyzed patients (11). However, these latter references focused on the practical implementation of a hemodialysis, without providing any dosimetry or blood and renal clearance data.
The doses to the salivary glands reported in Table 2 are very much comparable to those reported in the literature for typical RLT patients (11), but the kidney doses are almost an order of magnitude lower than the literature values (10). The values for the blood effective half-life somewhat exceed the 10.8 ± 2.5 h previously reported (2), whereas the RM doses are higher than the reported literature values (8). This scenario is consistent with the expectations of stage 4 renal failure and consequently slower clearance of 177Lu due to the intermittent hemodialysis.
The dose limits for the salivary glands, kidney, and RM specified in the European Association of Nuclear Medicine guidelines (10) safely exceed what we observed in our patient (Fig. 2). The maximal RM dose was 1.1 Gy (in cycle 1), which still falls below the specified limit of 2 Gy for a single exposure (10). The absence of changes in the blood cell counts (Fig. 1) does not suggest an excessive radiation exposure of the RM.
On the basis of a preliminary organs-at-risk dose analysis, we reduced the number of hemodialyses in the therapy ward from 3 to 2. Across all therapy cycles, the intercycle variability of the organs-at-risk doses did not indicate any significant dependence on the number of hemodialyses performed during the RLT. Dosimetry of the hemodialysis practitioners did not indicate any untoward radiation exposure.
CONCLUSION
We report the successful treatment with [177Lu]Lu-PSMA-617 of a prostate cancer patient with comorbid stage 4 CKD according to the Kidney Disease: Improving Global Outcomes scale. There were no adverse events, and the RLT was tolerated well by the patient. The organs-at-risk doses consistently fell within the dose limits of the European Association of Nuclear Medicine guidelines. This case suggests that hemodialysis treatment for chronic renal failure should not exclude metastatic castration-resistant prostate cancer patients from obtaining RLT and that the procedure presents little radiation exposure for hemodialysis staff.
DISCLOSURE
Axel Rominger has received research support and speaker honoraria from Siemens. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can [177Lu]Lu-PSMA-617 therapy be applied to a patient with stage 4 CKD according to the Kidney Disease: Improving Global Outcomes scale while undergoing hemodialysis in the therapy ward?
PERTINENT FINDINGS: We applied 6 RLT cycles successfully and safely to a patient with stage 4 CKD according to the Kidney Disease: Improving Global Outcomes scale. The organ doses were well below the recommended dose limits.
IMPLICATIONS FOR PATIENT CARE: The case suggests that [177Lu]Lu-PSMA-617 treatment of a patient with stage 4 CKD according to the Kidney Disease: Improving Global Outcomes scale can be performed effectively and safely and without exceeding organ dose limits.
Footnotes
Published online Aug. 24, 2023.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 8, 2023.
- Revision received June 12, 2023.





{kind=link}
{kind=link}
{kind=link}