


Abstract
Our objective was to evaluate the feasibility, additional benefit, and toxicity of extending prostate-specific membrane antigen (PSMA)–targeted radioligand therapy in patients with metastatic castration-resistant prostate cancer. Methods: From 208 patients treated with 177Lu-PSMA every 6–8 wk, 26 who had not progressed and not experienced grade 3 or higher toxicity after 6 cycles continued to receive 177Lu-PSMA until disease progression, complete remission, or removal from treatment because of toxicity or patient preference. Response rates, the additional benefit of treatment extension, and toxicity were assessed. Results: During treatment extension (≤13 cycles), 50% of patients achieved an additional prostate-specific antigen decline (−52% ± 34%; range, −1% to −100%), with 8% of patients achieving a congruent prostate-specific antigen–based and imaging-based complete response. Median progression-free survival was 450 d. Acute toxicity, including myelosuppression, was mild (≤grade 2). Xerostomia and chronic kidney disease became more common with repetitive dosing. Conclusion: Extension of 177Lu-PSMA treatment is feasible and effective in metastatic castration-resistant prostate cancer.
Prostate-specific membrane antigen (PSMA)–targeted radioligand therapy (RLT) has been shown to induce high prostate-specific antigen (PSA) response rates and to prolong imaging-based progression-free survival and overall survival when added to standard care in patients with advanced metastatic castration-resistant prostate cancer (mCRPC) (1,2). The standard RLT regimen consists of intravenous infusions of 177Lu-PSMA for 4 cycles, with 2 additional cycles (≤6 cycles in total) administered to patients having evidence of response (1,3). This standard 4-cycle regimen was chosen empirically, on the basis of limited experience and in the absence of individual dosimetry (4,5).
In a post hoc analysis of the Mainsail study, the total number of delivered docetaxel cycles was an independent factor for overall survival. Patients who received more than 10 cycles of docetaxel had a higher median overall survival (6). In other therapies for mCRPC, such as second-line hormonal therapy, reasons for any treatment discontinuation pertain either to disease progression or to unacceptable adverse events (7). Moreover, the safety and efficacy of extended treatment with 177Lu-DOTATATE in other entities has recently been reported (8).
To our knowledge, there are limited data evaluating whether extended treatment beyond 6 cycles is feasible and can enhance PSA response rates. Here, we retrospectively analyzed the feasibility, additional benefit, and toxicity of extended treatment in all patients who had undergone extended 177Lu-PSMA therapy at our institution.
MATERIALS AND METHODS
The full version of the materials and methods is provided as a supplemental file at http://jnm.snmjournals.org.
Study Population
Twenty-six patients with advanced mCRPC and referred for 177Lu-PSMA RLT between November 2016 and May 2021 were included in this retrospective analysis (Table 1). Before the start of 177Lu-PSMA RLT, all patients had demonstrated progression after standard systemic therapies (2). 177Lu-PSMA-617 was administered in compliance with the Declaration of Helsinki, §37, and the German Medicinal Products Act, AMG §13.2b. The institutional review board at Hannover Medical School approved this study (approval 9182_BO_S_2020). All patients provided written informed consent to the data analysis.
Characteristics of Study Population (n = 26)
Assessment of 177Lu-PSMA RLT Treatment Response and Toxicity
Patients received 6.0–7.4 GBq of a 177Lu-PSMA ligand every 6–8 wk (2,9). They proceeded to the next cycle if they did not show PSA progression at about 2 wk before the next administration, and they continued to receive 177Lu-PSMA until disease progression or death; complete remission; or removal from treatment because of toxicity, deterioration in performance status, or patient preference. Of 208 mCRPC patients, 26 continued to receive 177Lu-PSMA beyond 6 cycles. These patients received 177Lu-PSMA-617 (n = 8) (2,9), 177Lu-PSMA I&T (n = 7) (10), or both ligands (n = 11). PSA levels and additional laboratory parameters (including full blood count, liver function parameters, and serum creatinine levels) were reevaluated every 2 wk. Treatment response was defined as PSA response rate according to the criteria of Prostate Cancer Clinical Trials Working group 2 (11), in conjunction with PSMA-targeted PET/CT. Toxicity was assessed according to the Common Terminology Criteria for Adverse Events (version 5.0).
Statistical Analysis
Continuous variables are expressed as mean ± SD and range. Waterfall plots were used to visualize PSA response. Survival curves were created using the Kaplan–Meier method. Statistical significance was established for P values of 0.05 or less. Statistical analysis was performed using Prism (version 9.0 for Microsoft Windows; GraphPad Software).
RESULTS
Twenty-six (12.5%) of 208 patients continued to receive 177Lu-PSMA after 6 cycles. Supplemental Figure 1 shows the reasons for treatment discontinuation in the other patients. Patients received up to 13 cycles of 177Lu-PSMA (9 ± 2; range, 7–13). Patients were treated until disease progression (n = 18), complete remission (n = 2), or removal from treatment because of toxicity (n = 1) or patient preference (2 in near-complete response [CR], 1 after stroke, and 1 after radiation of cerebral metastases). Treatment was ongoing in 1 patient at the time of analysis.
Extended Treatment May Deepen the Response to 177Lu-PSMA, but Only in a Subset of Patients
Efficacy of 6 Cycles
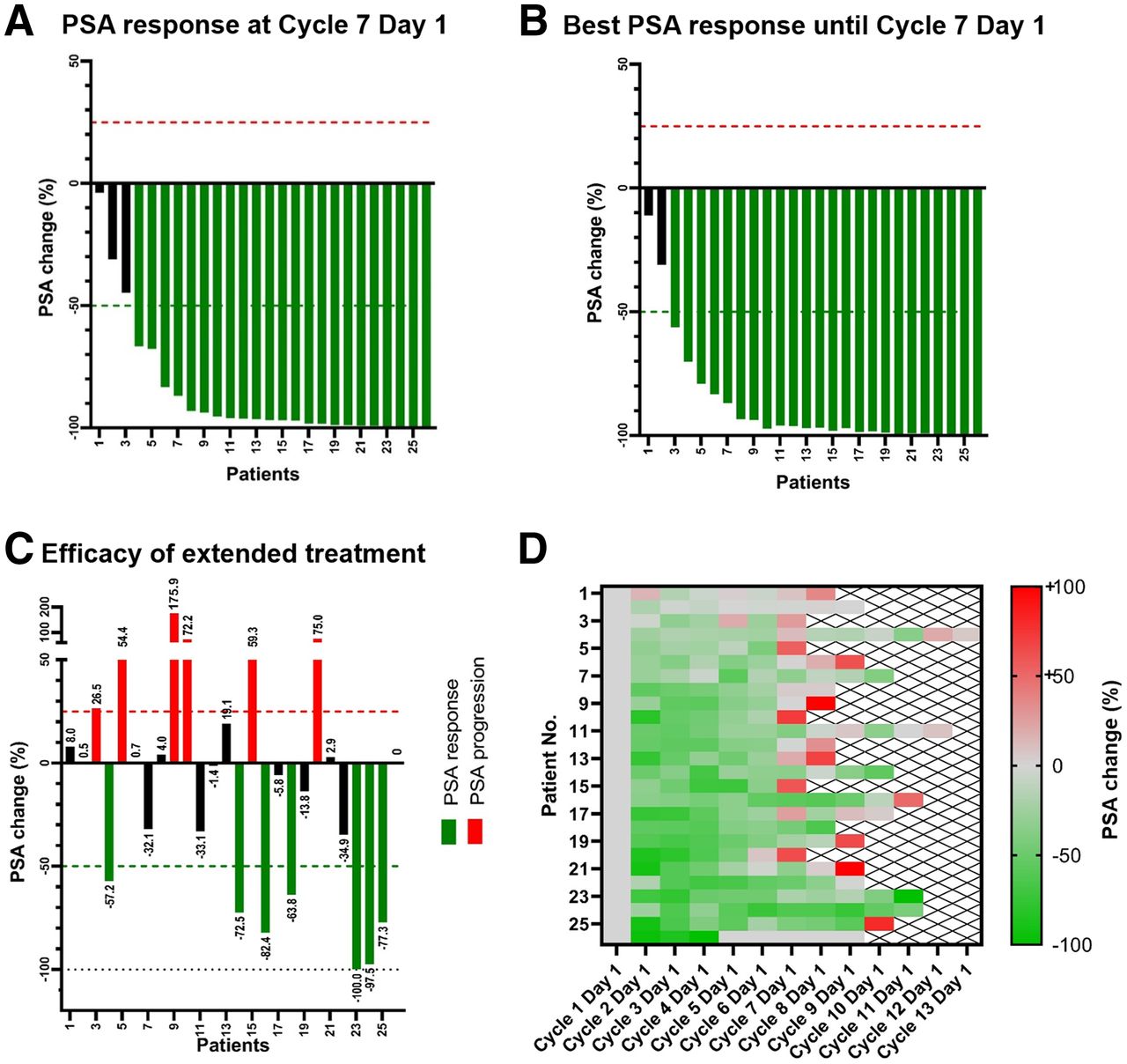
After 6 cycles of 177Lu-PSMA (Fig. 1A), PSA at cycle 7, day 1, had declined in all patients (−86% ± 24%; range, −4% to −100%), and 23 (88%) of 26 patients had demonstrated a PSA response. The best PSA decline until cycle 7, day 1, was −88% ± 22% (range, −11% to −100%), and 24 (92%) of 26 patients demonstrated a PSA response. PSA declined by more than 90% in 19 (73%) patients (Fig. 1B).

Efficacy of PSMA-targeted RLT. (A) After 6 cycles of PSMA-targeted RLT, PSA had declined in all patients (−86% ± 24%; range, −4% to −100%), and 88% of patients had demonstrated PSA response. (B) Best PSA response within first 6 cycles was −88% ± 22% (range, −11% to −100%), and 92% of patients demonstrated PSA response. (C) During treatment extension, 13 patients achieved additional PSA decline compared with nadir, whereas PSA increased in 12 patients. (D) Heat map shows percentage PSA reduction between individual cycles in patients receiving extended treatment. Most patients had progressed at cycle 9, day 1, or discontinued treatment.
Efficacy of Additional Cycles
During treatment extension (Fig. 1C), 50% of patients achieved an additional PSA decline (−52% ± 34%; range, −1% to −100%). Two patients who had already achieved biochemical CR (1 during the first 6 cycles, 1 during treatment extension) but still had PSMA-positive disease also achieved imaging-based CR during treatment extension (Fig. 2). However, the PSA nadir was reached within the first 6 cycles in 11 (42%) of 26 patients.

Efficacy of extended 177Lu-PSMA treatment in 75-y-old man with mCRPC. Postherapeutic scintigraphic images at cycle 1, day 2, showing widespread osseous and lymph node metastases (A, left panel). After 6 cycles, there was PSA response, but PSA was still measurable and residual PSMA-expressing metastases could be noted (A, middle panel, arrow). At cycle 11, day 2, there was both PSA-based and imaging-based complete remission (A, right panel), confirmed by targeted PET (B).
Median progression-free survival was 450 d (range, 276–1,742 d; time from first RLT cycle to progression, Fig. 3). With treatment extension, 42% of patients had stable disease for at least 6 additional months after the end of the standard regimen (in patients with CR [n = 2], 1,126 and 931 d).

Median progression-free survival was 450 d in patients receiving extended treatment.
Extended Treatment Was Generally Well Tolerated
After 6 cycles and during extended treatment, toxicities did not exceed grade 2. Acute toxicity, including myelosuppression, was mild. Chronic kidney disease and xerostomia (Table 2) became more common with repetitive dosing, and became aggravated over time, although these side effects did not exceed grade 2. Dose reductions were made for 2 patients, exclusively because of hematotoxicity. One patient discontinued RLT because of aggravating grade 2 nephrotoxicity.
Toxicity (New Events) After 6 Cycles of 177Lu-PSMA RLT and Additional Events During Extended Treatment
DISCUSSION
Extended PSMA RLT is feasible and may contribute to deeper responses. Both an additional PSA response and a further PSA decline could be induced in patients undergoing extended treatment. Nevertheless, only 12.5% of all patients proceeded to treatment extension, and an even smaller number of all patients will actually benefit from such an approach. For most patients, the standard regimen of 4 + 2 cycles may therefore be the maximum amount of treatment (1,4). In pursuing such a more aggressive treatment regimen, we nevertheless demonstrated that even consistent PSA-based and imaging-based complete remission may be induced in patients having shown a partial response after 6 cycles. In the VISION trial, imaging-based progression-free survival was 8.7 mo (1). Progression-free survival in our extended treatment cohort was 15 mo. Although these cohorts cannot be directly compared, these findings support the potential of maintaining treatment success in selected patients through additional RLT cycles. However, even patients with CR ultimately relapsed, underlining that even the best PSA response may not be durable, although remarkable progression-free survival of up to 1,742 d could be achieved.
Toxicity was generally mild, as reported before for fewer cycles (1–3). However, xerostomia became more frequent as the number of treatment cycles increased. Likewise, kidney function declined, and we had to discontinue RLT in 1 patient with a significant increase in creatinine levels. Nevertheless, we did not observe grade 3 or 4 toxicities. However, as some sequelae of high organ doses may develop with temporal delay, one cannot rule out that there are late toxicities of which we did not became aware during follow-up if patients continued care elsewhere. In addition, many patients prone to development of relevant toxicity likely already discontinued treatment before a decision for extended treatment was made (1). Renal and salivary gland toxicity may become particularly relevant if patients receive PSMA-targeted RLT earlier after diagnosis, such as at the first biochemical recurrence.
Limitations of this study include its retrospective, single-center nature and limited patient number. Patients received 2 different compounds, that is, 177Lu-PSMA-617 and 177Lu-PSMA I&T. However, a recent study showed that both radiopharmaceuticals are similarly effective in patients with mCRPC, with very low rates of clinically relevant toxicities (12). The study concept comes along with an inherent selection bias toward patients with an exceptional PSA response and mild toxicity. The selection bias, along with the limited patient number, prevented a reasonable analysis of predictors for actual benefit of extended treatment. Future work should therefore put effort into identifying those patients who will have deeper responses through extended treatment.
CONCLUSION
We demonstrated that extension of 177Lu-PSMA treatment is feasible and effective in selected patients with mCRPC. However, only a small fraction of all treated patients may proceed to and benefit from extended treatment.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is extended treatment with PSMA-targeted RLT feasible and active in patients with mCRPC?
PERTINENT FINDINGS: In a retrospective study on patients receiving up to 13 177Lu-PSMA cycles every 6–8 wk until disease progression, complete remission, or removal from treatment because of toxicity, death, or patient preference, 50% of patients achieved an additional PSA decline or CR, but xerostomia and chronic kidney disease became more common with repetitive dosing.
IMPLICATIONS FOR PATIENT CARE: Extended treatment to deepen responses is feasible and active.
Footnotes
Published online Jul. 19, 2022.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 14, 2022.
- Revision received July 12, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.