


Abstract
3231
Introduction: Nuclear imaging of renal cortex lesions in kidneys is important in the evaluation of pyelonephritis and renal scarring post-infection in pediatrics. Minimizing radiation dose in pediatric patients, whose cancer risk per unit administered activity is thought to be much higher than for adults due to higher tissue sensitivity and longer potential lifespan, is of vital interest. Balancing image quality and the potential long-term effects of radiation can pose a challenge. 99mTc-labeled dimercaptosuccinic acid (DMSA) renal imaging at Boston Children’s Hospital (BCH), is commonly performed without an accompanying CT for attenuation map estimation to reduce radiation dose. In lieu of CT-based attenuation estimation, attenuation maps are typically approximated using manual segmentation of the body outline of emission slices with uniform attenuation within. This work proposes an alternative method that estimates the attenuation maps directly from DMSA scatter window data using deep learning (DL). Our objective is to show that with careful tuning and optimization, generating a personalized attenuation map from the scatter data only for DMSA SPECT renal imaging is plausible and can be accomplished highly accurately.
Methods: DMSA SPECT projections for photopeak (130-150 keV) and scatter (110-130 keV) windows were produced via SIMIND Monte Carlo simulation of 58 pediatric XCAT torso phantoms with activity distributions modeled from pediatric DMSA patients acquired at BCH. Simulations were based on a Siemens SPECT/CT with ultra-high resolution parallel-hole collimators (256x256x256, pixel size=0.23976cm) and linear attenuation factors from tables of tissue values. Reconstructions were performed using in-house OSEM software configured to match patient acquisitions, including individual orbits of the dual-camera heads of the SPECT system. Scatter window reconstructions without attenuation correction and ground truth attenuation maps were then used as training data for an artificial neural network.
Attenuation map prediction was performed by training a Generative Adversarial Network (GAN). GANs pose two opposing CNN-based models, a Generator, and a Discriminator in an adversarial arrangement to train the Generator to produce the desired synthetic images. This project used a standard Discriminator and a Generator that was a modified to contain additional layers, residual connections, customized objective functions, and a one-cycle learning rate scheduler. The discriminator used a gradient penalty objective for training and the Generator used a multi-object loss function consisting of a multi-scale structural similarity metric combined with an L2 norm. Training used single slices from 8 distinct noise realizations per patient simulation split into 5-folds, for 600 epochs, and a maximum learning rate of 1e-3 for the 1-cycle learning rate scheduler.
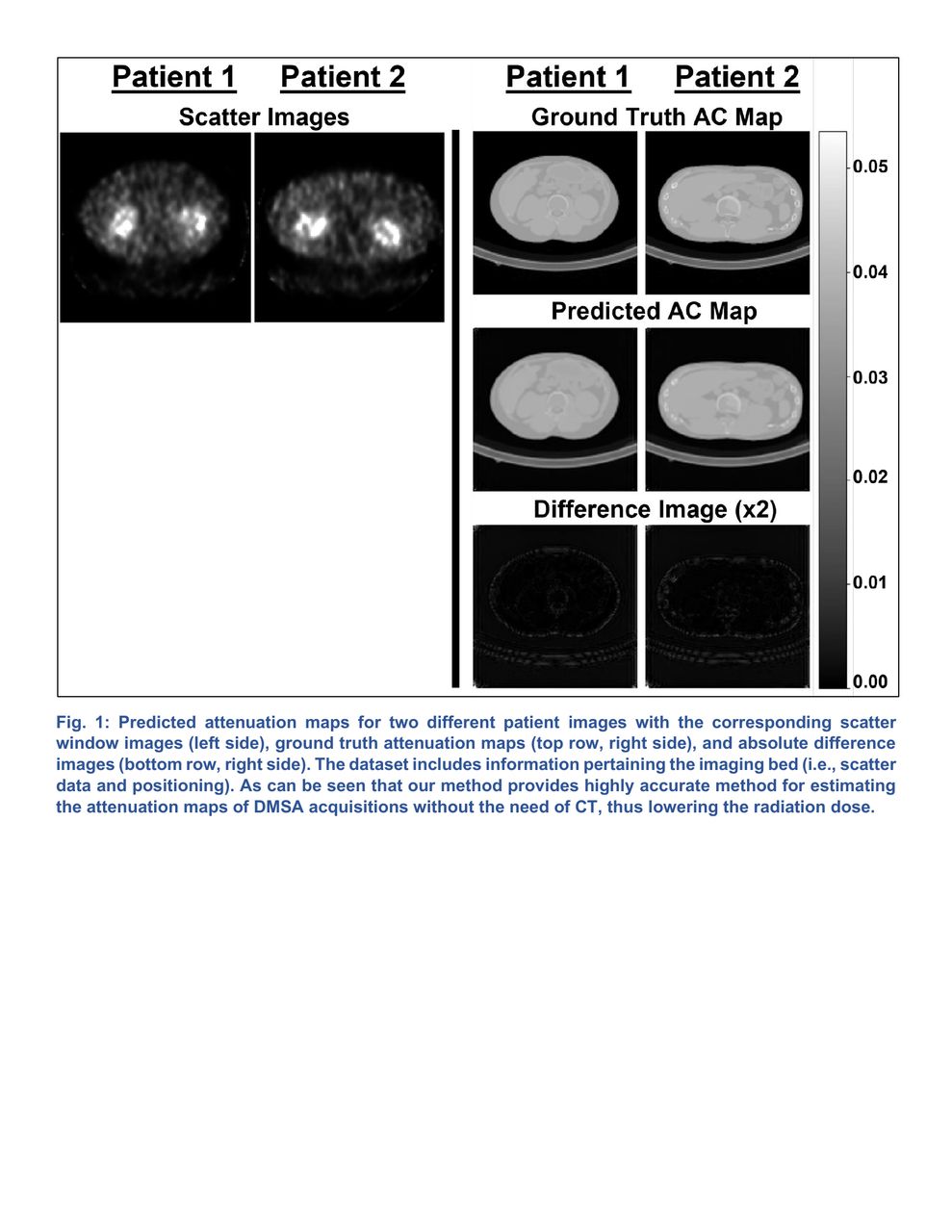
Results: The proposed method produces attenuation maps that are relatively close to the ground truth. Fig 1 shows scatter reconstructions (top row, left) and a comparison of the predicted linear attenuation map (middle row, right) to that of the ground truth (top row, right) with corresponding absolute difference images scaled by 2 for ease of visualization (bottom row, right). The imaging bed of the BCH SPECT/CT added to the XCAT attenuation prior to simulation is also part of the predicted attenuation map and not added as a post-process. We calculated a Mean Absolute Error of 0.0013 (± 0.00018) and an average Peak Signal to Noise Ratio of 12.9 across the validation sets. In the future we plan to address the residual ringing on the edges as well as incorporating the patient’s arms when in the down position within the field-of-view of the system into our dataset.
Conclusions: Generating an accurate attenuation map from the scatter window data alone without the use of any other information is not only feasible but highly accurate including the location and attenuation of the imaging bed.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.