


Abstract
2955
Introduction: There are approximately 12,000 new cases of Spinal Cord Injury (SCI) every year in the United States. Though primary injury causes immediate structural damage, a series of secondary injuries such as hemorrhage, inflammation and neuronal loss leads to functional deficits after SCI. Inflammation plays a significant role in both neurotrauma and neurodegeneration. We previously demonstrated that intranasal insulin treatment reduces inflammation and increases viability of cells within the CNS following traumatic brain injury in a preclinical model. Here we investigate the benefit of intranasal insulin in a model for moderate SCI by using FDG-PET uptake and behavioral assessments.
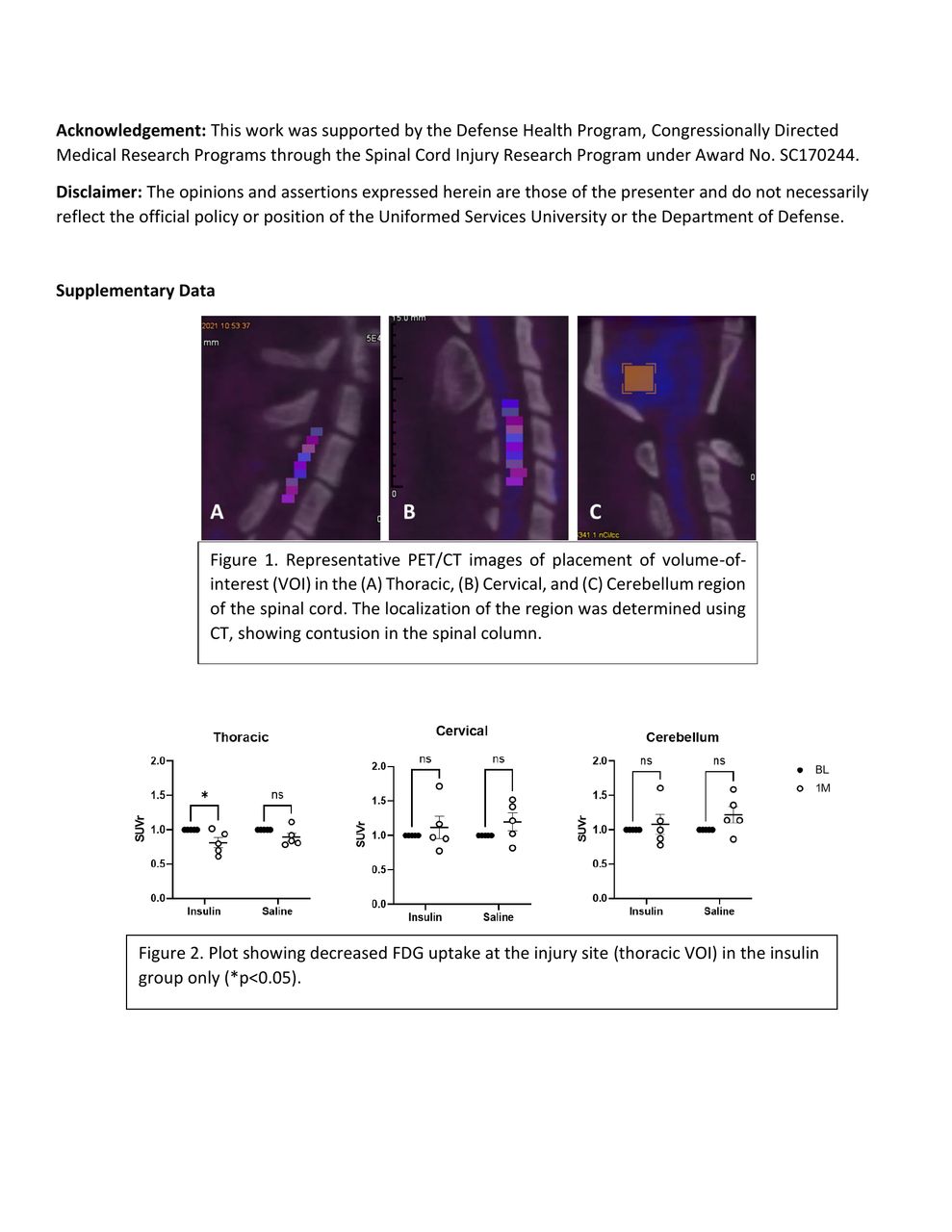
Methods: Adult male Sprague Dawley rats were randomly divided into 2 groups – Insulin Treatment Group (n=5) and Saline Control Group (n=5). The PET/CT images were acquired (Siemens Inveon preclinical scanner, Erlangen, Germany) for two time points – Baseline (prior to injury) and 1 month post injury. For injury, the animals received a laminectomy around vertebral level T9, and moderate contusion SCI (150 kdyne force) was induced with the Infinite Horizon Impactor (Precision Systems Incorporated, Natick, Maat). Intranasal insulin (6IU) or saline was administered daily for from 4 hours post-injury to 7 days. FDG uptake was assessed by drawing volume of interest (VOI’s) in the thoracic (injured) spinal cord, cervical (uninjured) (C2-C5) spinal cord, and cerebellum (brain), using Siemens Inveon Workplace software (V4.2) [Figure 1]. Standardized Uptake Value normalized to Baseline (SUVr) was plotted to compare the changes over time in the two groups. The Basso-Beattie-Bresnahan (BBB) scale was used to assess neurological function in both the Control and Treatment group weekly starting at 1-day post-injury. The statistical analysis was done using GraphPad Prism (v9.0.2), two-way repeated measures (RM) of analysis of variance (ANOVA) and Sidak’s multiple comparisons tests.
Results: The Insulin Treated group showed a significant decrease in the FDG uptake at the injury site (thoracic) at one month post injury compared to its baseline. There were no changes in FDG uptake at the sites away from injury (cervical or the cerebellum VOI). The control group showed no significant changes in any of the VOIs at one month post injury compared to its baseline [Figure 2]. BBB scores showed no significant difference between groups at any time point.
Conclusions: One month post SCI, FDG PET scans show reduced FDG uptake in lesion site which is greater, and statistically significant in the insulin treated group. This reduction in FDG uptake in the intranasal insulin treated group appears to reflect reduced inflammation at the injury site. The behavioral analysis indicates that this reduction in glucose uptake does not translate to any change in gross motor function. We will also discuss histological assessment of inflammation, neuronal survival, and glial cell activation at the injury site.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.