


Abstract
2800
Introduction: The surgical success of parathyroid surgery for primary (PHP) or secondary (SHP) hyperparathyroidism may be limited by the location of the glands or their difficult access, mainly in previously operated necks. The introduction of new molecular imaging techniques with the incorporation of fluorescent tracers such as indocyanine green (ICG) and near-infrared (NIR) imaging has proven useful in detecting the parathyroid glands (1,2). The aim of this study is to describe our experience with ICG in the intraoperative location of the parathyroid glands.
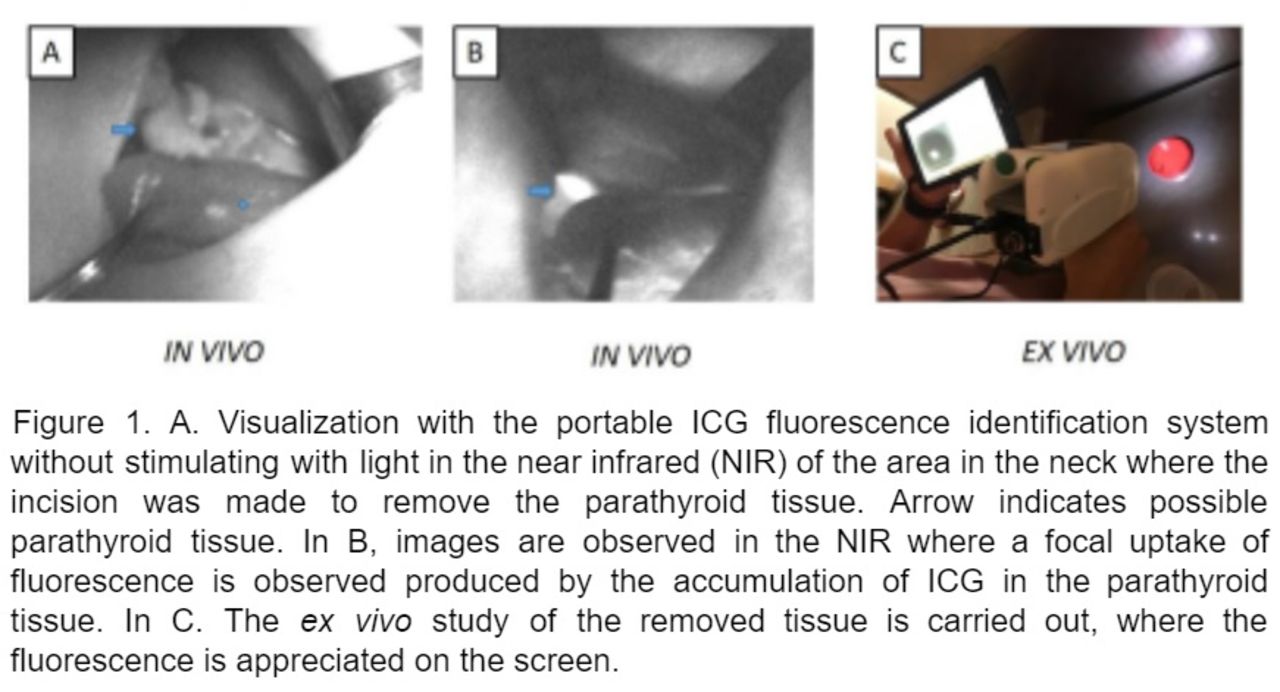
Methods: The intraoperative identification of parathyroid tissue using ICG is based on the intravenous administration of 7.5mg (3ml) as a bolus at the moment of wanting to visualize the glands. ICG is distributed systemically and by mechanisms not yet understood it accumulates at the parathyroid and thyroid tissue level, not in muscle, fat or lymph nodes. The arrival time is 20-30 seconds and later the accumulation of ICG by these tissues can be identified. A system capable of detecting ICG fluorescence is needed, for which we developed a portable system. When the accumulation of ICG is observed, the fluorescent structures are identified in-vivo, and when they are removed (ex-vivo). Subsequently, the piece is sent to pathological anatomy for confirmation, as well as taking intraoperative PTH before and after removal of the parathyroid tissue. We describe the aforementioned procedure in 1 patient with PHP and 5 patients with SHP.
Results: 86% of the patients were female. The age range was between 20 and 55 years (average 33). Of the 6 patients, 5 had a diagnosis of SHP and 1 of PHP The mean preoperative PTH was 850pg/mL in the HPTP and 1730 pg/mL in the HPTS. As a noteworthy history, two of the patients with SHP had been operated on for the same condition. Nuclear medicine studies demonstrated the presence of parathyroid hyperplasia in at least two glands for HPTS and an ectopic (mediastinal) adenoma for PHP. During the intraoperative period, the parathyroid tissue was identified both in-vivo and ex-vivo using our fluorescence detection equipment (Figure 1). In the case of PHP, the adenoma was excised. In the cases of SHP, the glands were removed and a remnant was left. In the intraoperative period, a total of 13 glands were removed using the fluorescent guide and confirmed with pathological anatomy. The decrease in postoperative PTH values was reported (PHP at 150pg / mL and SHP at 1177pg / mL on average). No complications were recorded.
Conclusions: Our experience confirms the value of ICG and our portable fluorescence detection system in the identification of parathyroid tissue, being able to be used safely and effectively for intraoperative localization of the parathyroid glands in both PHP and SHP. We have been able to provide the surgeon with a tool to identify these glands and thus achieve surgical success.
References:
1. De Long JC, Ward EP, Lwin TM, Brumund KT, Kelly KJ, Horgan S, Bouvet M. Indocyanine green fluorescence-guided parathyroidectomy for primary hyperparathyroidism. Surgery 2018 Feb;163(2):388-392. doi: 10.1016/j.surg.2017.08.018.
2. Cui, L., Gao, Y., Yu, H., Li, M., Wang, B., Zhou, T., & Hu, Q. (2017). Intraoperative Parathyroid Localization with Near-Infrared Fluorescence Imaging Using Indocyanine Green during Total Parathyroidectomy for Secondary Hyperparathyroidism. Scientific Reports, 7(1), 1–10. https://doi.org/10.1038/s41598-017-08347-6

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.