


Abstract
2634
Introduction: The distinction between viable and non-viable myocardium in patients with LV dysfunction is a clinically important issue among possible candidates for myocardial revascularization. Several non-invasive techniques are used to detect and assess ischemia and myocardial viability. These techniques include echocardiography, dobutamine stress echocardiography, cardiac magnetic resonance imaging (MRI) and SPECT and PET cardiac imaging. In this systematic review We aim to : 1) Review the current literature on the accuracy of these methods. 2) Summarize their advantages and disadvantages 3) Provide representative images of various testing modalities 4) Evaluate future directions for use of Novel PET tracers and AI Algorithms.
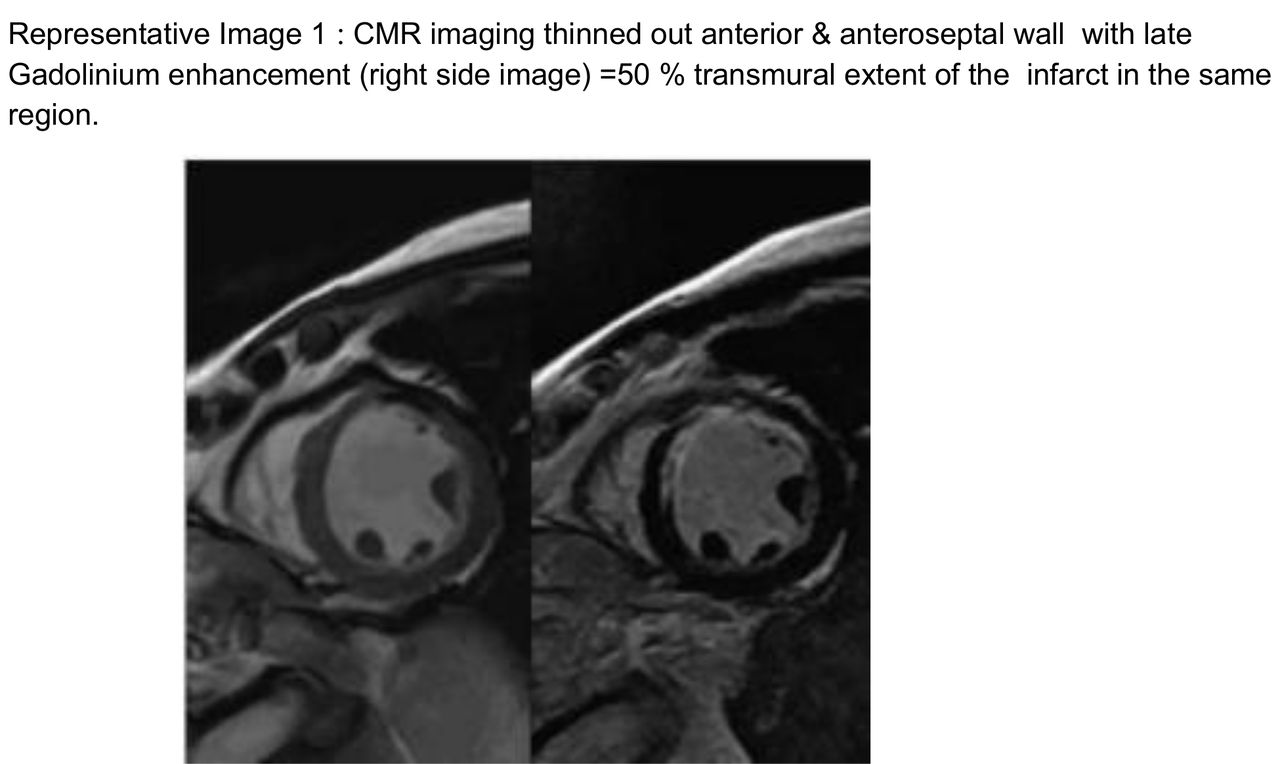
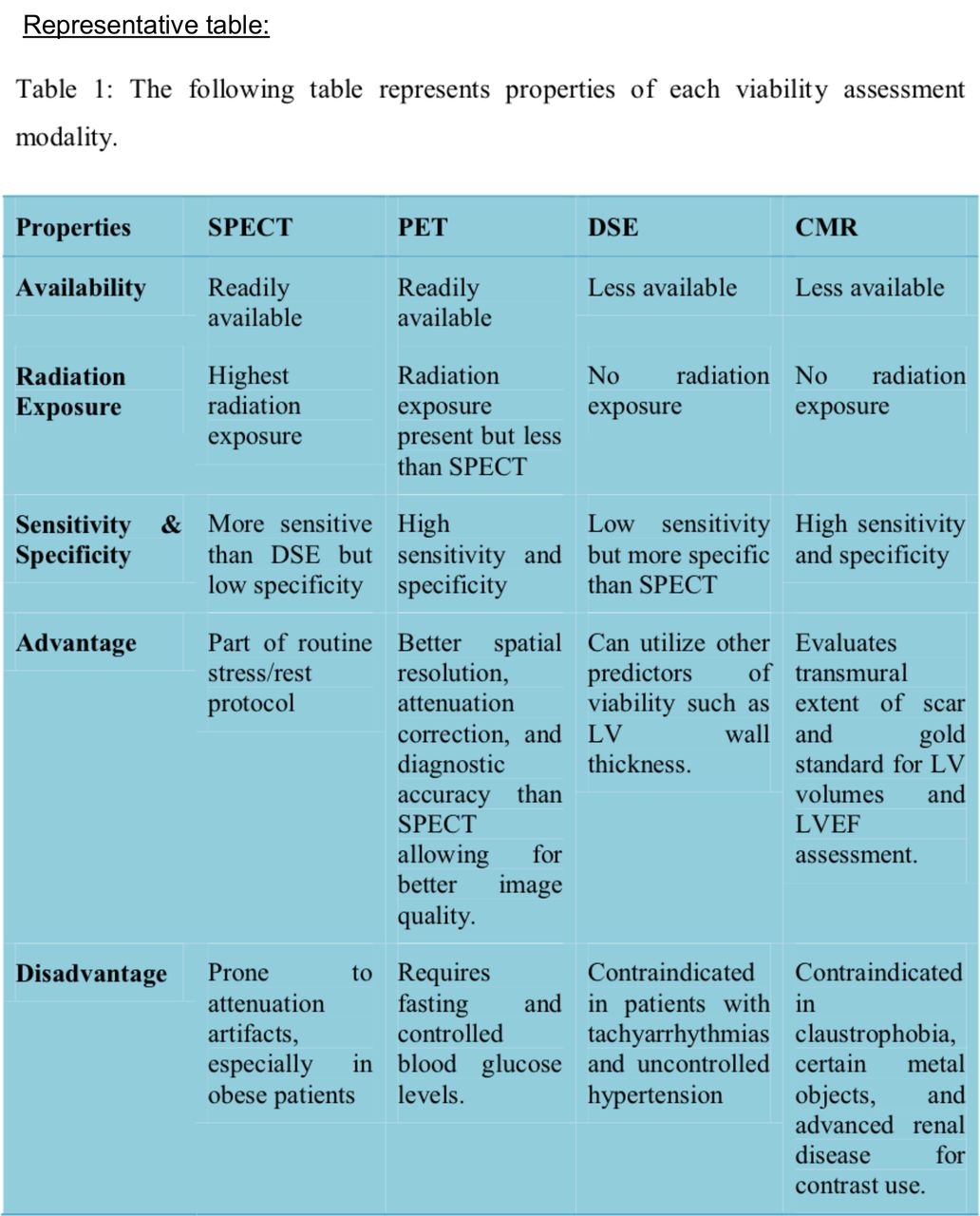
Methods: During LV dysfunction due to ischaemia, three possible effects can be seen on the myocardium: non-viable myocardium, stunned myocardium and hibernating myocardium. We describe the pathophysiology of irreversible and reversible ischemic damage. Recent echocardiographic modalities like myocardial wall deformation indices including tissue Doppler imaging (TDI), strain rate imaging (SRI) and dobutamine stress echocardiography (DSE) were evaluated. DSE relies on echocardiographic assessment of myocardial thickening and endocardial excursion during administration of dobutamine. The four type of responses noted are discussed along with it. Cardiovascular magnetic resonance (CMR) is used along with gadolinium-chelated contrast studies to provide information on global left ventricular function and regional wall motion. The transmural extent of scarring is inversely correlated with functional recovery of the dysfunctional myocardium post revascularization, whereas an absence of late gadolinium enhancement in a hypokinetic myocardium has been shown to be associated with functional recovery. Nuclear Imaging tests - SPECT and PET myocardial viability studies are the most frequently performed non-invasive techniques. Various radioactive tracers used and their mechanism of localization are discussed with a brief discussion on Novel PET/CT tracers and their indications.Various modalities and their advantages and disadvantages are analyzed and tabulated, along with representative images for each of them.
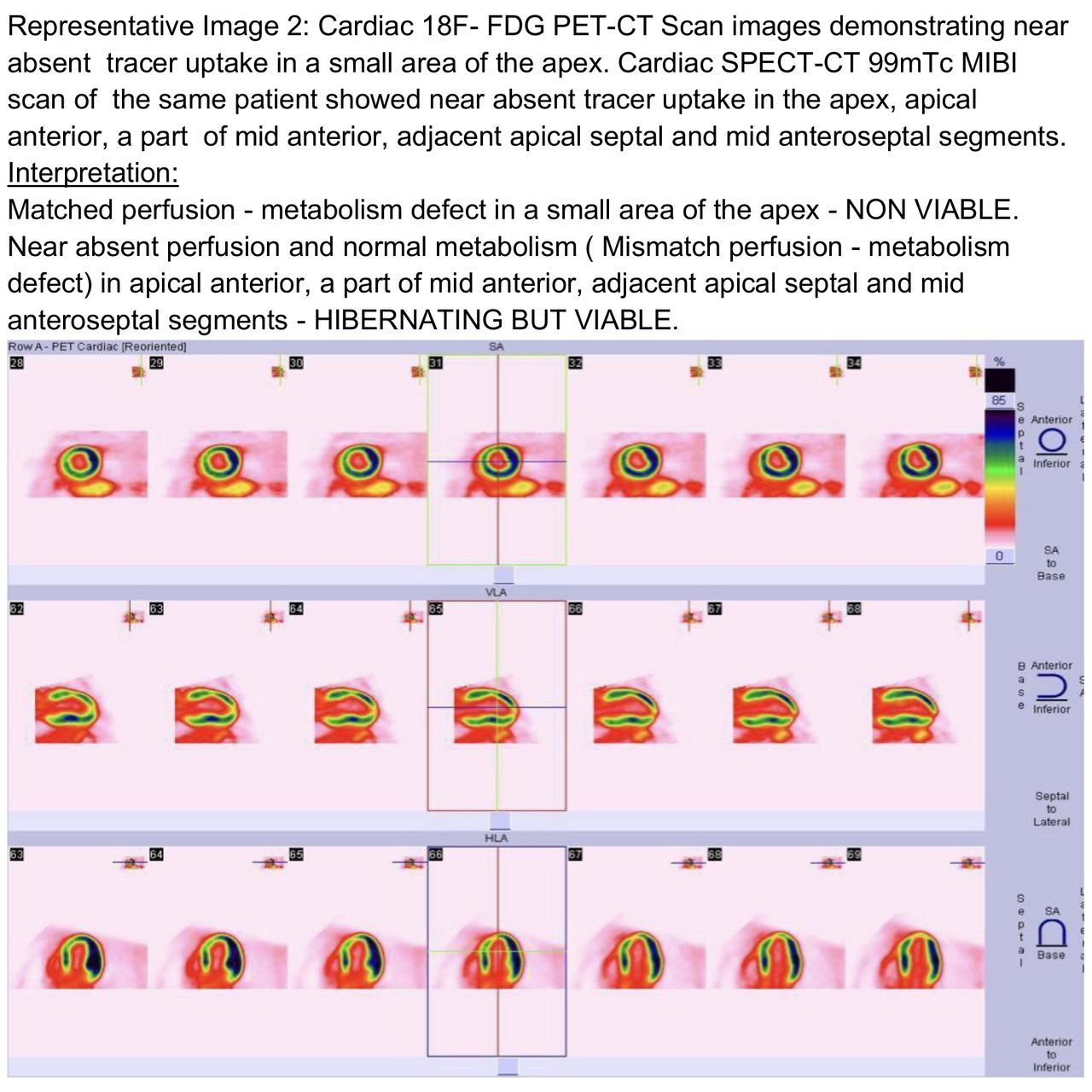
Results: It was observed in various studies that viability testing can have a lower specificity. A number of studies have explored the low specificity and NPV and have questioned the role of viability testing as to having any benefit in predicting outcomes post revascularization. Some studies observed that the presence of viable myocardium by 18F- FDG PET/CT scan was not related to long-term survival in patients with ischemic cardiomyopathy. After reviewing several studies and recent data available we concluded that PET/CT has the highest sensitivity for the prediction of regional ventricular function post revascularization, making it the technique of choice as per our study. However, we found that there is only limited understanding of the extent and severity of mismatched perfusion and metabolism that are required to predict degrees of improvement in LV function. Therefore defining and quantifying the myocardial viability defects seen on 18F-FDG PET/CT is very much required in the present scenario.
Conclusions: It is imperative that the nuclear medicine physicians are well versed with the diagnostic utility of these tests. 18F- FDG PET/CT imaging is concluded to be the best means for defining viability and has proven useful in predicting regional and global recovery of LV function following revascularization. With the information presented, the physicians will be able to optimize the use of these non-invasive modalities for optimal selection of patients who would actually benefit from revascularization procedures.



In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.