


Abstract
2384
Introduction: Newer PET scanners with increased z-axis fields of view and with improved detector technology provide greater sensitivity and thus capture more counts for image generation, potentially allowing for reduced administered activities or reduced image acquisition times. These potentials are particularly relevant to the clinical care of children. Our study aims to quantify the impact of simulated shorter acquisition times (and by analogy lower administered activities) for 18F-FDG PET whole-body PET images obtained in children and young adults with a state-of-the-art digital PET/CT system.
Methods: This retrospective, IRB-approved study included 27 (9 male, 16 female) clinically indicated whole-body FDG PET/CT examinations acquired on a 5-ring 25 cm axial field of view GE Discovery MI Gen 2 PET/CT System (GE Healthcare). Included examinations were selected from clinically performed examinations to be equally distributed by body weight from 0-69.9 kg, with uptake times of 60±10 minutes. Standard-of-care clinical images were acquired at 90 seconds per bed position with 21% overlap. PET examinations were reprocessed based on retrospective trimming of list-mode data to simulate reduced scan acquisition times of 60, 55, 50, 45, 40, and 30 seconds per bed. Images were reconstructed using time-of-flight reconstructions with SharpIR.
A total of 189 image volumes (27 examinations, 7 reconstructions) were generated and independently rated in random order by three board-certified pediatric radiologists with experience in pediatric nuclear medicine. Reviewers were blinded to patient history and simulated activity. Each reconstructed PET volume was scored based on: (1) lesion conspicuity, (2) conspicuity of normal structures, and (3) overall image quality using a 5-rank Likert scale; perceived image noise was also scored using a 4-rank Likert scale. Additionally, for each of the reconstructions, 3-dimensional circular regions-of-interest (ROIs) with a diameter of 3 cm were drawn by a fourth independent observer in (1) a homogeneous area of liver parenchyma, and (2) muscle of the right mid-thigh. The most FDG-avid lesion in the image volume was also contoured. Standardized uptake values (SUV) were recorded for each of the measurements, including SUVmean, SUVmax, and SUVstandard deviation. SUVstandard deviation / SUVmean was calculated as a surrogate of image noise.
Likert scores were converted to numerical values for statistical analysis. Analysis of variance (ANOVA) Friedman's test and Dunn's test were used to compare scores across acquisition times.
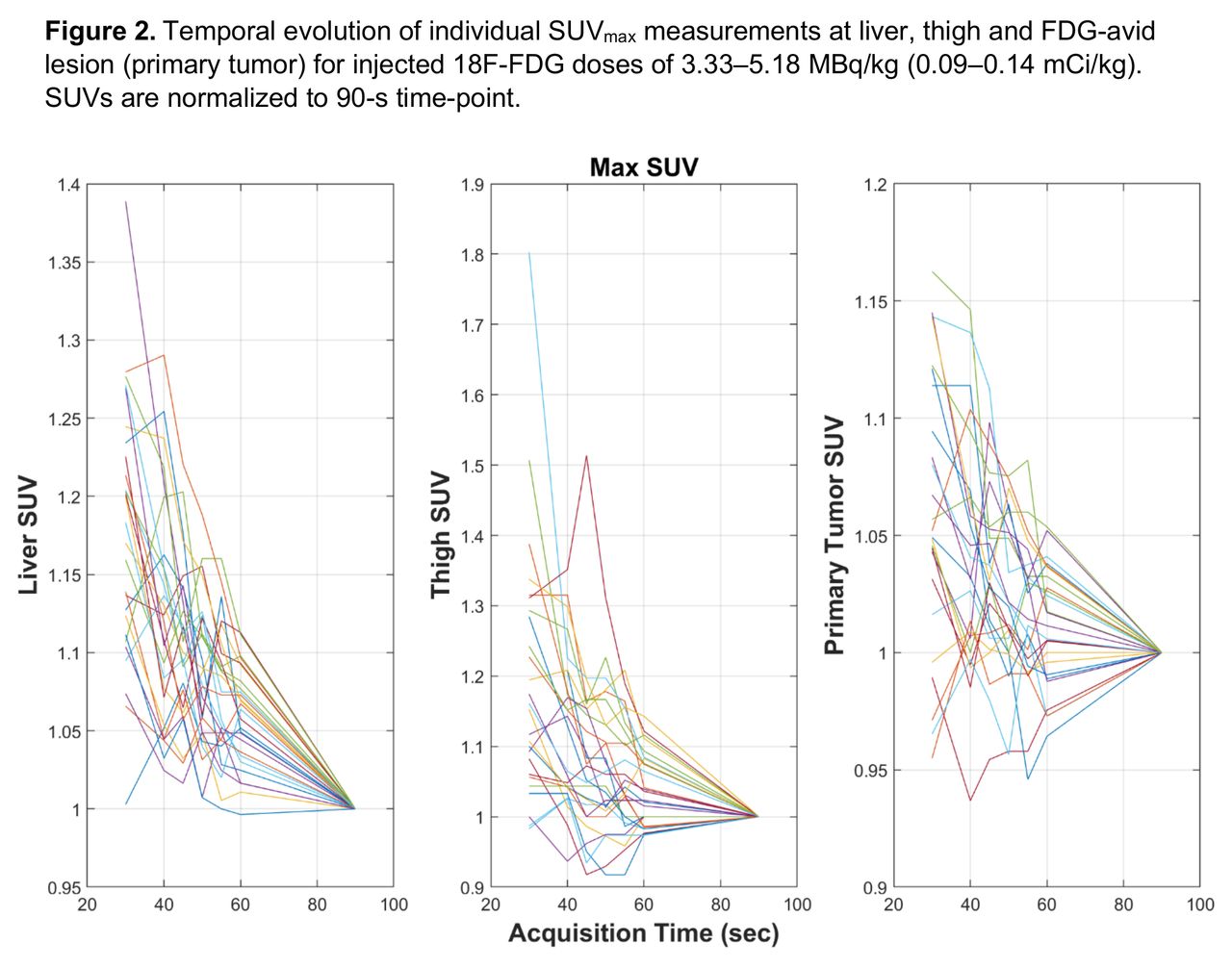
Results: Patients included in this study had a mean age of 10.8 ± 8.3 yr, a weight of 36.3 ± 19.7 kg, and received 0.12 ± 0.01 mCi/kg 18F-FDG. As compared to the 90 sec/bed standard-of-care protocol, a significant difference was observed for lesion conspicuity scores at ≤ 40 sec/bed (p=0.007), for conspicuity of normal structures and overall image quality at ≤ 45 sec/bed (p=0.038 and p=0.006, respectively), and image noise at ≤ 55 sec/bed (p=0.025) (Figure 1). Quantitatively, no statistical difference was observed for SUVmean in liver, thigh, or lesion across all reconstructed acquisition times, although SUVstandard deviation/ SUVmean and SUVmax showed a trend of increase with decreased acquisition times (p<0.0001). Significant differences were present for SUVstandard deviation/SUVmean of liver at ≤ 60 sec/bed (p= 0.044); thigh at ≤ 55 sec/bed (p = 0.018) and lesions at ≤ 50 sec/bed (p = 0.015). Figure 2 demonstrates the decreasing variability in SUVmax with increasing acquisition times.
Conclusions: For children and young adults receiving 0.12 mCi/kg injected activity of 18F-FDG and imaged with a state-of-the-art extended field of view digital PET/CT system, an acquisition time of 60 sec/bed (or 0.8 mCi/kg injected activity imaged at 90 sec/bed) shows no significant impact in image quality or quantitative measures.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.