


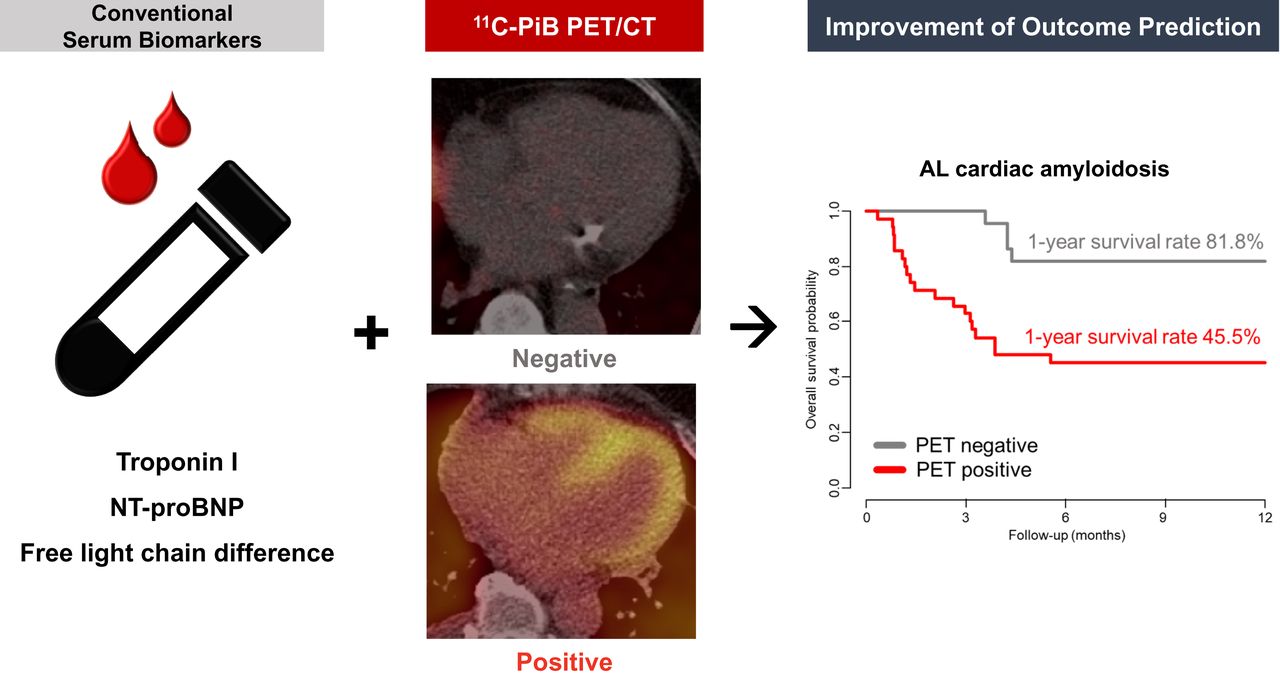
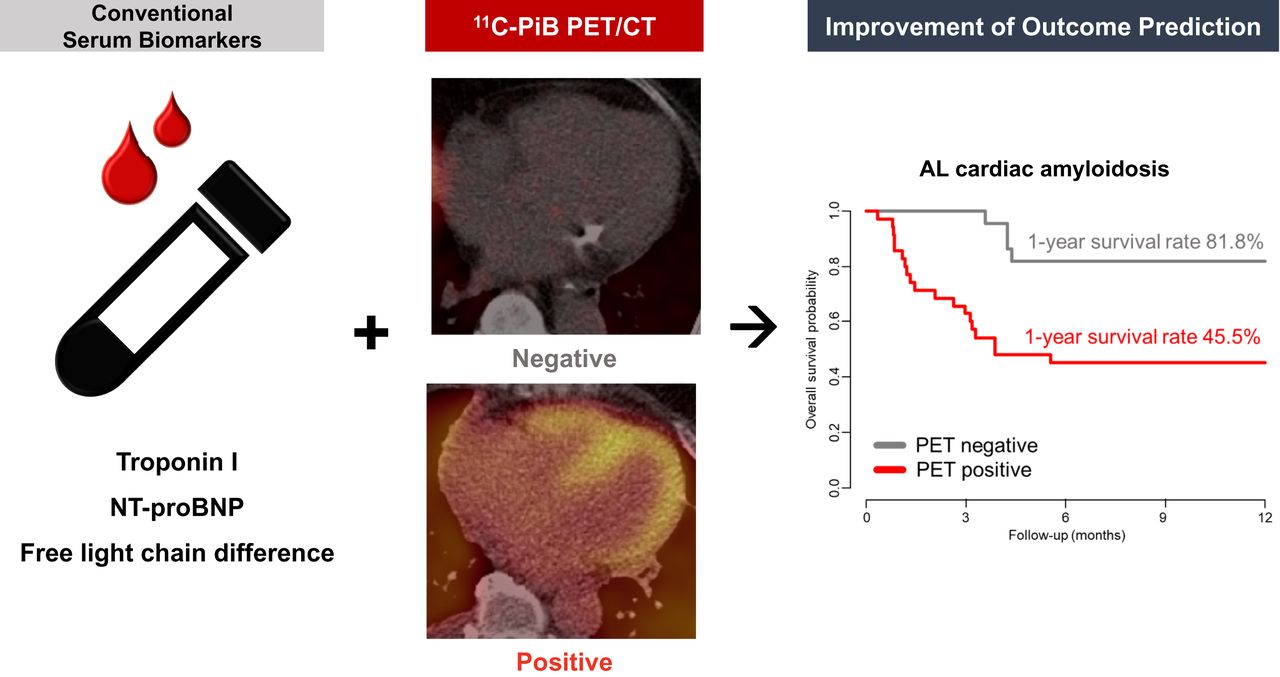
Visual Abstract
Abstract
11C-Pittsburgh compound B (PiB) PET/CT visualizes the amount of myocardial amyloid deposit and can be used to prognosticate patients with amyloid light-chain (AL) cardiac amyloidosis (CA). However, whether 11C-PiB PET/CT has any independent additional prognostic value beyond the commonly used biomarkers remains unknown. Methods: This prospective study was on a cohort of 58 consecutive patients with AL CA who underwent 11C-PiB PET/CT. The patients were stratified into 2 groups on the basis of a visual assessment of whether there was myocardial 11C-PiB uptake on PET/CT. The primary endpoint was 1-y overall mortality. The independent prognostic utility of 11C-PiB PET/CT was analyzed using net reclassification improvement and integrated discrimination improvement. Results: Among the 58 patients enrolled, 35 were positive for myocardial 11C-PiB uptake on PET/CT. Patients with myocardial 11C-PiB PET uptake had a worse 1-y overall survival rate than those without (81.8% vs. 45.5%, P = 0.003 by log-rank test). In the multivariate analysis, positivity for myocardial 11C-PiB uptake on PET/CT was an independent predictor of 1-y mortality (adjusted hazard ratio, 3.382; 95% CI, 1.011–11.316; P = 0.048). In analysis of 3 subgroups of patients—those with a troponin I level of at least 0.1 ng/mL, those with an N-terminal pro-B-type natriuretic peptide (NT-proBNP) level of at least 1,800 pg/mL, and those with a difference of at least 180 mg/L between free light chains (the 3 commonly used biomarkers and their thresholds for staging in AL amyloidosis)—Kaplan–Meier curves showed for all 3 subgroups that patients positive for myocardial 11C-PiB uptake on PET/CT had a worse prognosis than those who were negative. Additionally, when the results of 11C-PiB PET/CT were added to these 3 biomarkers, the performance of 1-y mortality prediction significantly improved by net reclassification improvement (troponin I, 0.861; NT-proBNP, 0.914; difference between free light chains, 0.987) and by integrated discrimination improvement (0.200, 0.156, and 0.108, respectively). Conclusion: 11C-PiB PET/CT is a strong independent predictor of 1-y overall mortality and provides incremental prognostic benefits beyond the 3 commonly used biomarkers of AL amyloidosis staging. Considering the recent development of numerous amyloid-targeting molecular imaging agents, further investigations are warranted on whether PET/CT should be included in risk stratification for patients with AL CA.
Amyloidosis is a rare group of disorders caused by the accumulation of proteinaceous fibrils in certain organs that compromises their structure and function (1). Cardiac amyloidosis (CA) refers to the myocardial deposition of amyloid fibrils, of which the immunoglobulin amyloid light chain (AL) and transthyretin are the most common types (2). Cardiac involvement is the major determinant of prognosis in AL amyloidosis patients; therefore, accurate evaluation of the degree of involvement is crucial for prognostication (3).
Endomyocardial biopsy is commonly used for the evaluation of CA, for which the presence of AL proteins can be evaluated, together with its degree of deposition (4). However, endomyocardial biopsy involves invasive removal of the myocardial tissue and does not provide information on disease activity or the hemodynamic consequences. In contrast, biomarkers such as serum cardiac troponins and N-terminal pro-B-type natriuretic peptide (NT-proBNP)/BNP, which are associated with the hemodynamic burden to the heart, are used for cardiac staging, albeit not specific for CA (5–7). The absolute difference between the involved and uninvolved free light chains (dFLC), as a parameter for hematologic disease burden, is also incorporated into the staging system and improves the risk stratification of AL amyloidosis patients (8). Additionally, imaging markers such as left ventricular strain on speckle-tracking echocardiography and the gadolinium enhancement pattern on cardiovascular MRI are helpful for the prognostication of AL amyloidosis patients (9–14).
To date, advances in nuclear imaging have allowed a more specific, noninvasive approach to the diagnosis and prognostication of CA (15). We and others have shown that 11C-Pittsburgh compound B (PiB) PET/CT may be used for diagnosis of AL CA by reflecting the amount of myocardial amyloid deposited and that this amount is associated with patient prognosis (16–18). However, for a new imaging test to be clinically useful, verification is needed of whether it has any independent additional prognostic value beyond the commonly used conventional prognosticators. In this study, we aimed to determine whether 11C-PiB PET/CT could provide independent incremental prognostic value over serum biomarkers in patients with AL CA.
MATERIALS AND METHODS
Study Population
This prospective study was on a cohort of patients with AL CA diagnosed at Seoul National University Hospital between 2012 and 2019. Cardiac involvement of AL amyloidosis was diagnosed with confirmation by monoclonal gammopathy in the peripheral blood and lineage-restricted expansion of plasma cells in the bone marrow, together with either a positive endomyocardial biopsy result or a cardiac imaging–based diagnosis with histologic confirmation of amyloid infiltration by noncardiac biopsies (average left ventricular wall thickness ≥ 12 mm on echocardiography with no identifiable cause; unexplained low voltage QRS amplitude < 0.5 mV in the limb leads of the 12-lead electrocardiogram; typical features of CA on cardiovascular MRI, including diffuse late gadolinium enhancement and myocardial extracellular volume expansion) (19–21).
The endomyocardial biopsy was performed in a standard manner (22). Deposition of amyloid in the myocardium was confirmed by positive amyloid P staining by immunohistochemistry and by apple-green birefringence by Congo-red staining (23).
The study complied with the declaration of Helsinki and was approved by the Institutional Review Boards. All subjects signed an informed-consent form.
11C-PiB PET/CT Protocol and Image Interpretation
11C-PiB PET/CT was performed using a dedicated PET/CT machine (Biograph 40; Siemens Medical Solutions). After low-dose CT scanning, 11C-PiB (555 MBq) was injected intravenously. Thirty minutes later, a 3-dimensional PET/CT scan was obtained at 3 min per bed position, with a spatial resolution of 4.2 mm. The detailed 11C-PiB PET/CT protocol has been published elsewhere (16). Images were displayed in transaxial, coronal, and sagittal planes 5 mm thick. Because the purpose of this study was not to analyze the diagnostic accuracy of 11C-PiB PET/CT for AL CA but to demonstrate the clinical utility of 11C-PiB PET/CT in AL CA—and taking into consideration our previous finding that static 11C-PiB PET/CT reflects the myocardial amyloid load (17)—we used visual estimation of the static PET/CT images to divide the study population into groups either positive or negative for myocardial 11C-PiB uptake (Fig. 1) instead of using the quantified best cutoff SUV as in our previous study (16,17). The 11C-PiB PET/CT findings were considered positive when the myocardial 11C-PiB uptake was visually discernible from the blood pool (i.e., left ventricular cavity) (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). The individual images and interpretations of 11C-PiB PET/CT for all participants are listed in Supplemental Figure 2. All images were interpreted by a single expert masked to all other findings; in ambiguous cases, another independent observer participated in the visual analysis.

Representative positive vs. negative 11C-PiB PET/CT images. 11C-PiB PET/CT findings were classified into either negative (top panels) or positive (bottom panels) based on visually estimated retention of 11C-PiB in myocardium.
Echocardiography and Biomarker Measurement
Two-dimensional echocardiography was performed within 2 wk of PET/CT according to current guidelines (24). We measured early diastolic transmitral inflow velocity (E velocity) and early diastolic mitral annular velocity (e’ velocity) at the septal annulus by Doppler echocardiography to calculate the E/e’ ratio.
We collected data on the serum biomarkers retrospectively, based on the electronic medical records. A serum free-light-chain assay was performed at the initial diagnosis of amyloidosis, and dFLC was calculated from these results. Serum NT-proBNP and troponin I were measured within 1 mo from 11C-PiB PET/CT. Subgroups were analyzed in patients with serum biomarker values higher than the thresholds for each biomarker used in the revised Mayo staging system (troponin I ≥ 0.1 ng/mL, NT-proBNP ≥ 1,800 pg/mL, and dFLC ≥ 180 mg/L) (8).
Outcome Ascertainment
The outcome of the study was all-cause death, confirmed either by medical records or by reviewing the official nationwide data on death certification provided by the National Statistical Office of Korea. Patients were censored when they underwent heart transplantation. Each patient was followed from the date of the 11C-PiB PET/CT scan to either the date of death or up to 1 y.
Statistical Analysis
Continuous variables are described as mean ± SD or as median and interquartile range (IQR), and categoric variables are described as frequencies and percentages. We compared continuous variables using the Student t test or the Mann–Whitney U test after testing for normality with the Shapiro–Wilk test. We compared categoric variables between the 2 groups using either the χ2 test or the Fisher exact test.
We used the Kaplan–Meier estimate to describe and compare the survival curves between groups with the log-rank test. The proportional hazards assumption was checked using a statistical test based on the Schoenfeld residuals and their plots. Hazard ratios (HRs) with a 95% CI were determined using the Cox proportional hazards regression. Covariates with a P value of less than 0.05 on univariate Cox analysis were included in the multivariable model. Time zero was defined as the time of the 11C-PiB PET/CT scan. To determine the incremental predictive value of 11C-PiB PET/CT in addition to the 3 conventional serum biomarkers (troponin I, NT-proBNP, and dFLC), the net reclassification improvement and the integrated discrimination improvement were computed in regard to 1-y overall mortality (25).
All analyses used a 2-sided P value, and a P value of less than 0.05 was considered statistically significant. Statistical analyses were performed with SPSS statistics, version 25.0 (IBM Corp.), or R programming, version 4.0.5 (http://www.R-project.org).
RESULTS
Patient Characteristics
Among the 62 patients diagnosed with CA who underwent 11C-PiB PET/CT, 58 were included in the final analysis, excluding those with non-AL CA (n = 4). Among the 58 patients, 53 were histologically diagnosed with CA by endomyocardial biopsy, and the diagnosis in the remaining 5 was based on findings strongly suggestive of CA on at least 2 noninvasive modalities, such as echocardiography, cardiovascular MRI, or electrocardiography. The average age was 64.0 ± 9.1 y, and 43% were male. There were 35 patients with a positive 11C-PiB PET/CT result. The baseline demographic and clinical data are compared according to myocardial 11C-PiB PET uptake in Table 1.
Baseline Characteristics of Study Participants
The average age was higher in patients with a positive 11C-PiB PET/CT result than in those with a negative result (65.5 ± 9.8 y vs. 61.7 ± 7.6 y, P = 0.121). The systolic blood pressure was lower in patients with a positive 11C-PiB PET/CT result (median, 104.0 mm Hg [IQR, 92.5–114.0 mm Hg] vs. 111.0 mm Hg [IQR, 104.5–122.5 mm Hg]; P = 0.034). During the 1-y follow-up, more patients with a negative 11C-PiB PET/CT result received autologous peripheral blood stem cell transplantation (30.4% vs. 8.6%, P = 0.040). As for the echocardiography data, there was no significant difference between the 2 groups, except for E velocity (P = 0.021), e’ velocity (P = 0.043), and E/e’ ratio (P = 0.004).
Outcome Comparison According to the 11C-PiB PET/CT Results
During the 1-y follow-up, 23 patients died. Among 35 patients with a positive 11C-PiB PET/CT result, 16 (54.3%) died, whereas 4 (17.4%) of those with a negative result died. In the entire cohort, the 1-y overall survival rate was 59.3%; the survival rates at 3 mo and 6 mo were 77.2% and 59.3%, respectively (Fig. 2A). Kaplan–Meier survival curves showed that the 1-y overall survival rate was significantly worse in patients with a positive 11C-PiB PET/CT result (81.8% vs. 45.5%; P = 0.003 by log-rank test; Fig. 2B). In the multivariate analysis, positivity for myocardial 11C-PiB PET uptake was an independent predictor of 1-y overall survival (adjusted HR, 3.382; 95% CI, 1.011–11.316; P = 0.048) (Supplemental Table 1).
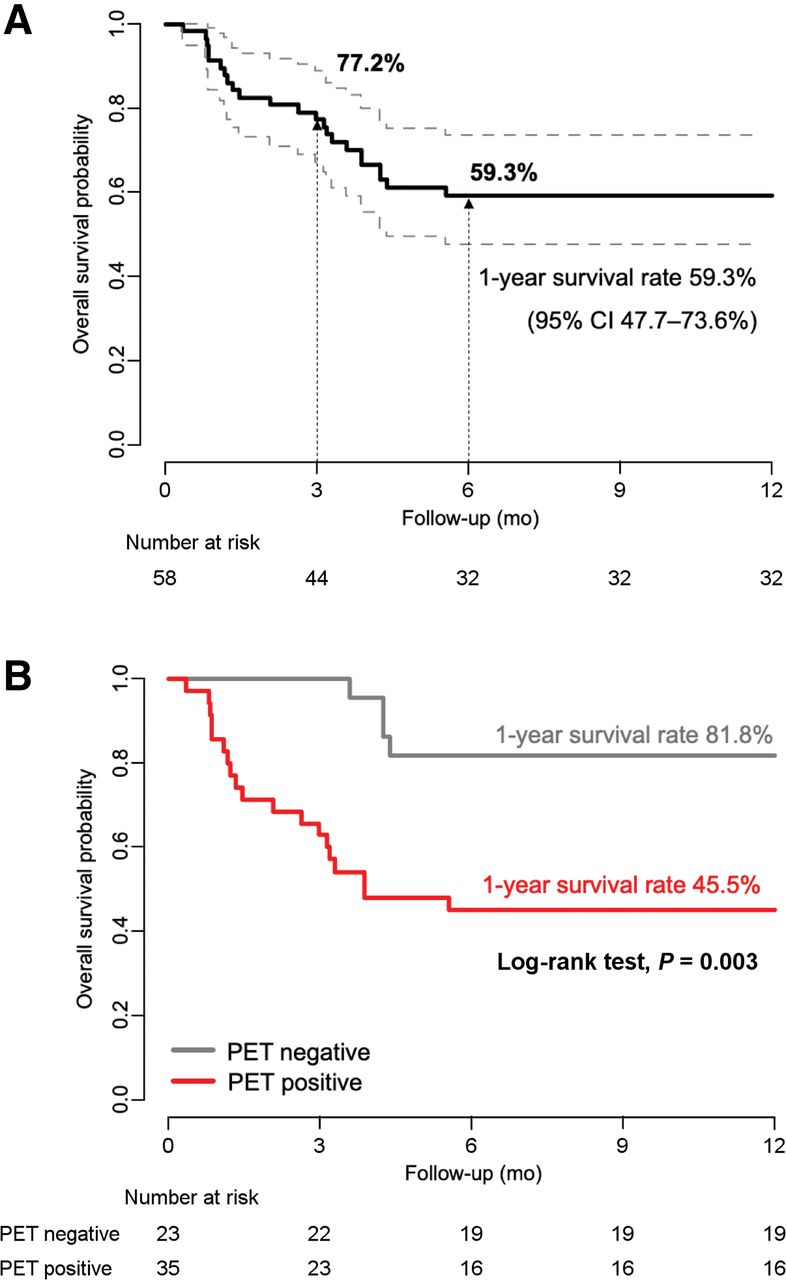
Kaplan–Meier survival curves for 1-y overall survival in entire AL CA population in current cohort (A) and according to myocardial 11C-PiB PET uptake as in Figure 1 (B).
Incremental Value of 11C-PiB PET/CT in Addition to Serum Biomarkers for AL CA Prognostication
Among the 58 AL CA patients, 34, 39, and 47 had values available for troponin I (median, 0.14 ng/mL; IQR, 0.07–0.39 ng/mL), NT-proBNP (median, 3,733 pg/mL; IQR, 1,117–7,232 pg/mL), and dFLC (median, 291.7 mg/L; IQR, 155.2–744.8 mg/L). There were no statistically significant differences in the 3 serum biomarkers between patients positive and patients negative for myocardial 11C-PiB PET uptake (Fig. 3).

Circulating biomarkers in patients with AL CA stratified by myocardial 11C-PiB PET uptake. Dot plot of each cardiac biomarker is according to myocardial 11C-PiB PET uptake: troponin I (A), NT-proBNP (B), and dFLC (C).
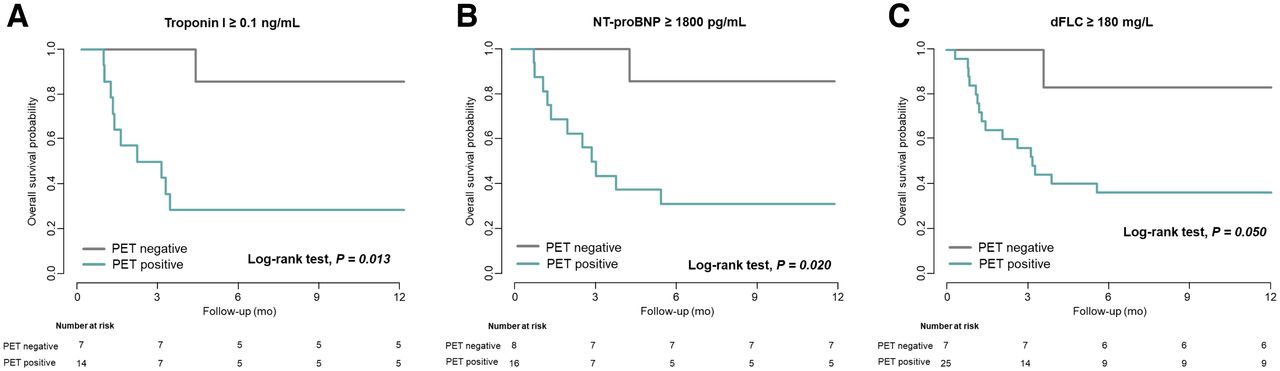
We performed a subgroup analysis on the subset of patients with levels of troponin I, NT-proBNP, and dFLC higher than the thresholds of the revised Mayo staging system (troponin I ≥ 0.1 ng/mL, NT-proBNP ≥ 1,800 pg/mL, and dFLC ≥ 180 mg/L) (8)—the subset of patients considered high-risk. Among the patients with a higher level of troponin I, positivity for myocardial 11C-PiB PET uptake was associated with worse overall survival during the 1-y follow-up (P = 0.013 by log-rank test, Fig. 4A [unadjusted HR, 8.884; 95% CI, 1.121–70.410; P = 0.039]). This pattern was similar in the patients with a higher level of NT-proBNP (P = 0.020 by log-rank test, Fig. 4B [unadjusted HR, 7.892; 95% CI, 1.011–61.610; P = 0.049]) and in the patients with a higher level of dFLC (P = 0.050 by log-rank test, Fig. 4C [unadjusted HR. 5.923; 95% CI, 0.783–44.82; P = 0.085). Additionally, the cardiac staging system incorporating 11C-PiB PET/CT in combination with the 2004 Mayo classification system (26) also significantly predicted 1-y overall survival (Supplemental Fig. 3).
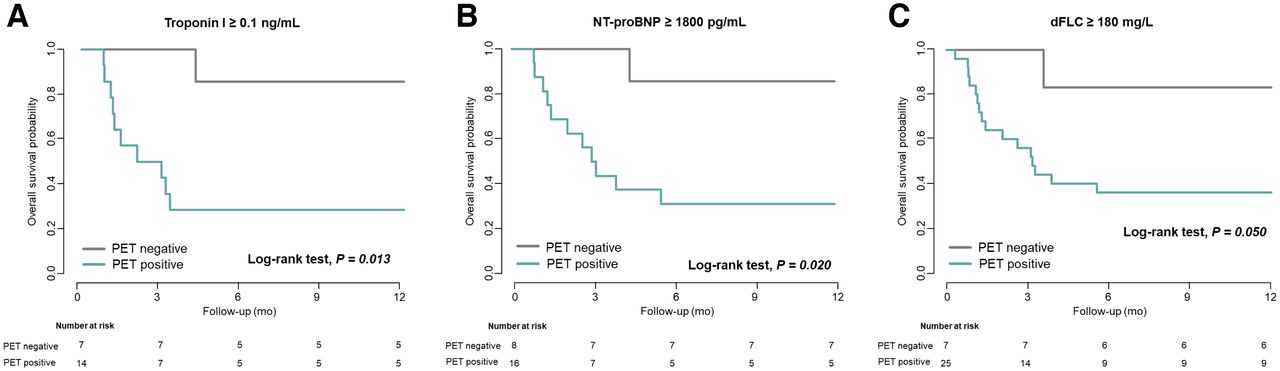
Kaplan–Meier survival curves for 1-y overall survival in patients with AL CA according to myocardial 11C-PiB PET uptake in patients with troponin I ≥ 0.1 ng/mL (A), NT-proBNP ≥ 1,800 pg/mL (B), and dFLC ≥ 180 mg/L (C).
To determine the incremental predictive value of 11C-PiB PET/CT in regard to outcome, the net reclassification improvement and integrated discrimination improvement were measured when the results of 11C-PiB PET/CT were added to the 3 conventional biomarkers (troponin I, NT-proBNP, and dFLC). Both the net reclassification and the integrated discrimination for prediction of 1-y overall survival showed a consistent significant improvement when the results of 11C-PiB PET/CT were added (net reclassification improvements of 0.861, 0.914, and 0.987, respectively [all P < 0.01]; integrated discrimination improvements of 0.200, 0.156, and 0.108, respectively [all P < 0.05]) (Supplemental Table 2).
DISCUSSION
To our knowledge, this was the first study to prove that in patients with AL CA, 11C-PiB PET/CT adds incremental prognostic power to conventional serum biomarkers, including troponin I, NT-proBNP, and dFLC. The main findings of the study were that 11C-PiB PET/CT predicts 1-y overall survival in patients with AL CA; that positivity for 11C-PiB PET uptake in the myocardium is a robust prognosticator capable of reclassifying subjects stratified as high-risk on the basis of the conventional biomarkers; and that compared with conventional biomarkers, 11C-PiB PET/CT provides additional independent prognostic information for predicting 1-y survival.
11C-PiB, the prototype PET amyloid tracer, is one of the most studied and widely used amyloid β peptide imaging agents. 11C-PiB PET was first used to image and quantify amyloid deposits in Alzheimer dementia (27,28) and is effective in diagnosing CA and predicting its prognosis as in our previous studies (16–18). However, the lack of evidence for an independent predictive power apart from the previously well-validated biomarkers for cardiac staging, such as troponin I, NT-pro BNP, and dFLC (8), limits the clinical application of 11C-PiB PET/CT in these patients. The current study expanded on our previous research and demonstrated the clinical implications of 11C-PiB PET/CT as a risk predictor for AL CA patients, independent of the commonly used biomarkers. Notably, we demonstrated that positivity for 11C-PiB PET uptake in the myocardium remains one of the strongest independent predictors of 1-y overall survival.
Patients with AL CA have a dismal prognosis, with nearly half dying within 1 y of the diagnosis as in the current study. Therefore, previous cardiac staging systems have recommended using cardiac biomarkers such as troponin I and NT-proBNP for risk stratification of AL amyloidosis (7,8). However, circulating cardiac biomarkers are not generally specific to AL CA and are also elevated in heart failure of other etiologies (29). Given the strong association between myocardial 11C-PiB PET uptake and worse clinical outcome in AL CA patients, we propose that for more accurate cardiac staging, 11C-PiB PET/CT be considered. The prognostic power of 11C-PiB PET/CT was maintained even in patients with higher levels of dFLC. Therefore, it is expected that 11C-PiB PET/CT could play a greater role in risk prediction of AL CA patients who are likely to be falsely considered high-risk, possibly because of nonspecific elevations of the serum biomarkers.
Among the biopsy-confirmed AL CA patients, there was a certain proportion with very low myocardial uptake of 11C-PiB when using SUVs as a measure of tracer uptake (16). In the current study, visual assessment of the 11C-PiB PET/CT images demonstrated that a significant number of patients who may be quantified as positive may actually have a negligible amount of myocardial 11C-PiB PET uptake that could be considered negative in the visual assessment, as is also supported by our previous work (17). These patients with low or visually negative myocardial 11C-PiB PET uptake had a significantly better prognosis than those with strong uptake, suggesting that uptake reflects the amount of amyloid deposited in the myocardium and can be used to determine the prognosis of patients with AL CA (17). Similarly, a small pilot study of 9 patients diagnosed with CA found that cardiac function and symptoms remained stable if there was no myocardial 11C-PiB PET uptake but that the prognosis was poor if there was uptake (30). Taking these findings together, it is expected that myocardial 11C-PiB PET uptake is strongly related to an advanced stage of disease. Further studies may be needed on standardized protocols using quantitative or semiquantitative methods to define the cutoffs that could be used to identify high-risk groups.
To date, no imaging tool has been included in the cardiac staging of patients with AL amyloidosis. However, staging is essential for prognostication, such as the identification of high-risk populations (31,32), and for optimal management. Given the need for improved cardiac staging systems in AL amyloidosis, we provide evidence for using 11C-PiB PET/CT to discriminate high-risk patients. Furthermore, our findings warrant further investigation, possibly by multicenter studies, into whether an additive imaging study is needed to accurately predict the prognosis of AL CA patients.
Our study was not without limitations. First, although the study was prospective, the sample size was small, and there is therefore a possibility of overfitting in the multivariate analysis. Second, because troponin I, NT-proBNP, and dFLC levels were not measured for all patients, a selection bias may exist. Third, not all patients with AL CA defined by clinically acceptable imaging-based criteria underwent an endomyocardial biopsy. However, all patients underwent noncardiac biopsies for histologic confirmation of systemic amyloidosis, and the diagnosis of AL CA followed the universally accepted diagnostic criteria. Finally, in contrast to most studies, which have used dynamic 11C-PiB PET for early detection of CA, we used static 11C-PiB PET/CT images because these have been shown to be a good alternative (33). Additionally, the static scan has the advantages of patient convenience, practicability for routine clinical use, and the potential to evaluate the whole body for amyloid deposits.
CONCLUSION
11C-PiB PET/CT is a strong, independent predictor of 1-y overall survival in patients with AL CA and is additive to well-validated serum biomarkers such as troponin I, NT-proBNP, and dFLC. Therefore, 11C-PiB PET/CT may be useful as a novel imaging marker for cardiac staging beyond established predictors in AL CA. Considering the recent development of numerous amyloid-targeting molecular imaging agents, future prospective studies are warranted on whether PET/CT should be included in risk stratification for AL CA patients.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Does 11C-PiB PET/CT provide independent incremental prognostic value over conventional serum biomarkers in patients with AL CA?
PERTINENT FINDINGS: 11C-PiB PET/CT was a strong independent predictor of 1-y overall survival in patients with AL CA and provided incremental prognostic benefits that were additive to well-established serum biomarkers such as troponin I, NT-proBNP, and dFLC.
IMPLICATIONS FOR PATIENT CARE: 11C-PiB PET/CT may be useful as a novel imaging marker for cardiac staging beyond established predictors in AL CA patients.
ACKNOWLEDGMENT
We thank the Medical Research Collaborating Center of Seoul National University Hospital for statistical review and consultation.
Footnotes
Published online Dec. 16, 2021.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication August 11, 2021.
- Revision received December 9, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Head-to-head comparison of [18F]florbetapir and [18F]FDG PET for the early detection of amyloidosis in systemic amyloidosis and plasma cell dyscrasias
- Molecular Imaging of Systemic and Cardiac Amyloidosis: Recent Advances and Focus on the Future
- Prognostic Value of Left Ventricular 18F-Florbetapir Uptake in Systemic Light-Chain Amyloidosis