


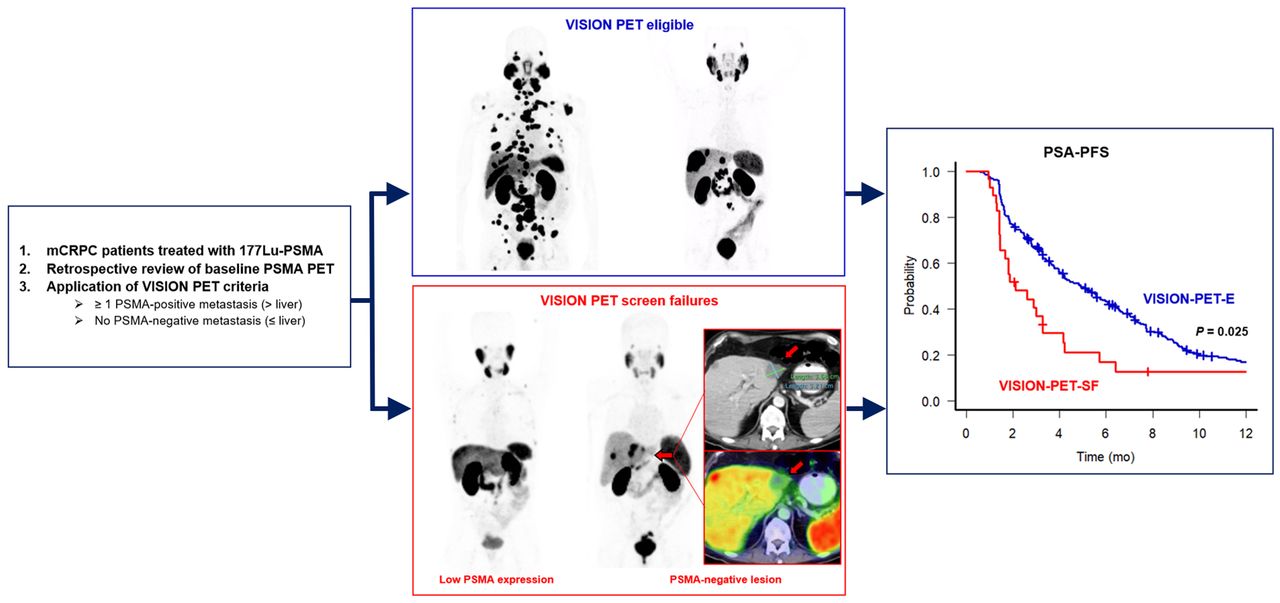
Visual Abstract

Abstract
The aim of the study was to assess the outcome of patients with metastatic castration-resistant prostate cancer treated with 177Lu-prostate-specific membrane antigen (PSMA) who would have been a screen failure (SF) in the VISION trial based on PSMA PET/CT criteria. Methods: We conducted a retrospective multicenter cohort study on 301 patients with metastatic castration-resistant prostate cancer treated with 177Lu-PSMA. The patients were classified into eligible (VISION-PET-E) and SF (VISION-PET-SF) groups on the basis of the baseline PSMA PET/CT results. Prostate-specific antigen (PSA) response rates, PSA progression-free survival, and overall survival were compared. Results: Of 301 patients, 272 (90.4%) and 29 (9.6%) were VISION-PET-E and VISION-PET-SF, respectively. The VISION-PET-SF patients had a worse rate of ≥50% PSA decline (21% vs. 50%, P = 0.005) and PSA progression-free survival (2.1 vs. 4.1 mo, P = 0.023) and tended to have a shorter overall survival (9.6 vs. 14.2 mo. P = 0.16) than the VISION-PET-E patients. Conclusion: The VISION-PET-SF patients had worse outcomes than the VISION-PET-E patients. Our cohort did not include preexcluded patients (10%–15%) by local site assessments. Thus, 20%–25% of the patients may be SFs in unselected populations. Refinements in patient selection for 177Lu-PSMA are needed to optimize outcomes.
Men with metastatic castration-resistant prostate cancer have few alternative therapeutic options when the disease progresses after androgen-deprivation therapy, androgen receptor signaling inhibitors, and chemotherapy. Recently, the VISION trial, an international open-label, randomized phase 3 trial showed that prostate-specific membrane antigen (PSMA)–targeted molecular radionuclide therapy (MRT) with 177Lu-PSMA can improve the outcome of patients with advanced metastatic castration-resistant prostate cancer. In this trial, 831 patients with metastatic castration-resistant prostate cancer previously treated with androgen receptor signaling inhibitor and taxane regimens were randomized in a 2:1 ratio to 177Lu-PSMA (7.4 GBq every 6 wk × 6 cycles) plus the best standard of care (n = 551) or the standard of care alone (n = 280). The trial met both primary endpoints of overall survival (OS) and radiographic progression-free survival (PFS). The median OS was 15.3 mo in the 177Lu-PSMA arm versus 11.3 mo in the standard-of-care–alone arm, resulting in a 38% reduction in the risk of death. The radiographic PFS was 8.7 versus 3.4 mo, respectively (1).
The VISION trial used PSMA PET/CT to select patients for inclusion. The screen failure (SF) rate was “only” 12.6% (126/1,003) (1), and some have argued that the trial could have been positive even in an unselected population (2). Eligibility by PSMA PET/CT results was determined by the sponsor’s central readers (criteria initially not disclosed). The VISION PET selection criteria were released publicly at the American Society of Clinical Oncology 2021 meeting (3). It remains unknown whether the VISION PET criteria were appropriate to screen for and identify patients who will not benefit from 177Lu-PSMA. Here, we exploited a database established retrospectively from multiple institutions to evaluate the outcome of patients treated with 177Lu-PSMA who would have been a SF by VISION PET criteria.
MATERIALS AND METHODS
We conducted a retrospective cohort study in our institutional database of patients treated with at least 1 cycle of 177Lu-PSMA between November 2017 and July 2021 (n = 74) and a multicenter dataset published previously (n = 230) (4). Patients were treated under compassionate use, an expanded access program, or clinical trials (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). All patients underwent a baseline 68Ga-PSMA-11 PET/CT scan before receiving 177Lu-PSMA therapy. The eligibility criteria and institutional treatment protocols are described in Supplemental Tables 1 and 2. The presence of PSMA-positive disease by PET was not consistently predefined and was determined by the local clinical investigators at each institution.
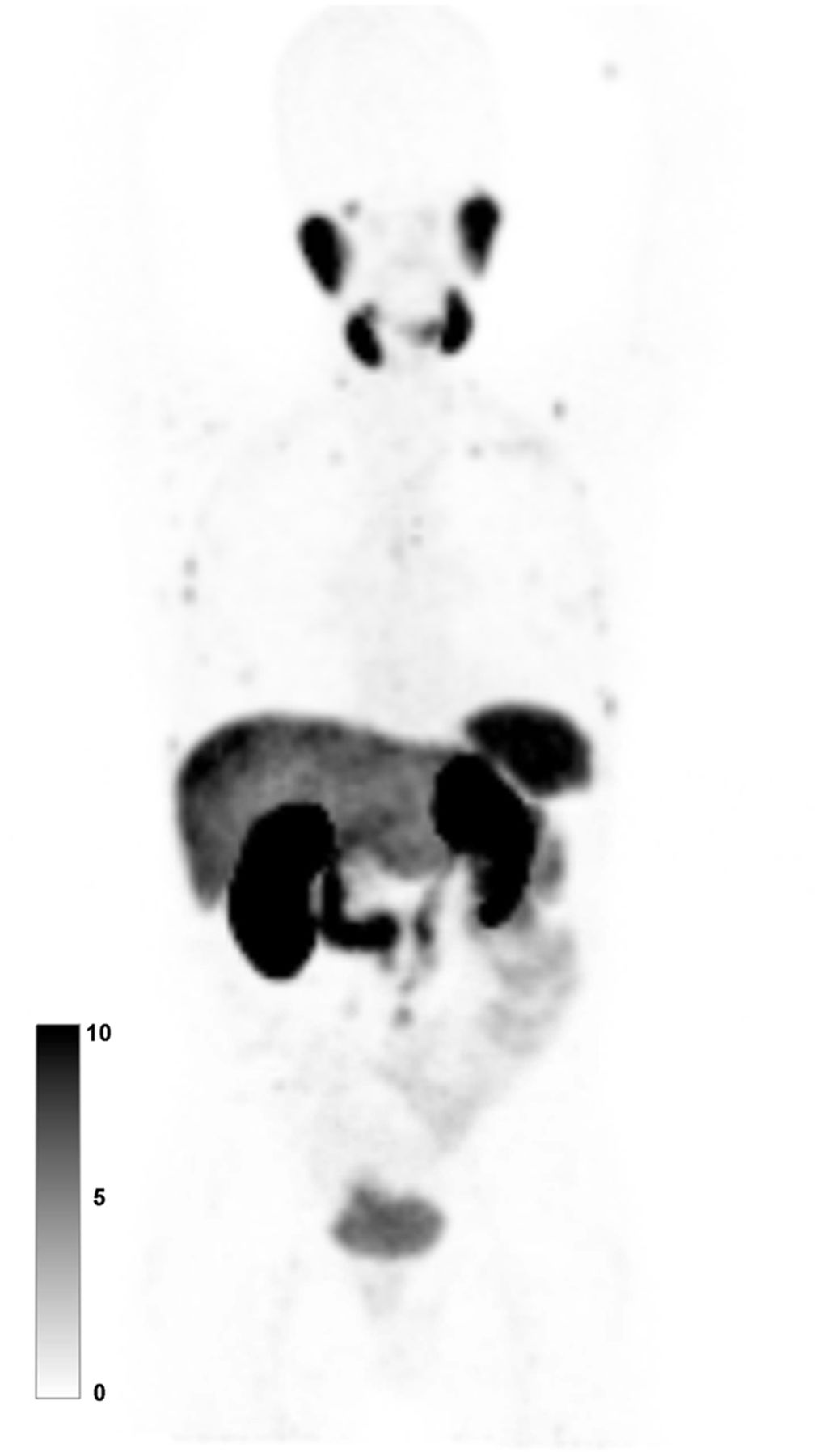
One reader dually board-certified in radiology and nuclear medicine, and masked to the patient outcomes, reviewed the baseline PSMA PET/CT scan of each patient to apply the VISION PET criteria and determine eligible (VISION-PET-E) versus SF (VISION-PET-SF) patients. Patients were classified as VISION-PET-E if they had at least 1 PSMA-positive and no PSMA-negative metastatic lesions. The presence of PSMA-positive lesions was defined as PSMA uptake greater than uptake by liver parenchyma (3). The patients were classified as VISION-PET-SF if the baseline scan showed either of the following: absence of a metastatic lesion with uptake greater than in the liver background (i.e., low PSMA expression) or the presence of at least 1 metastatic lesion measurable by CT (≥1 cm for bone lesions with a soft-tissue component [M1b] or solid/visceral organ lesions [M1c], ≥2.5 cm for lymph node lesions [N1-M1a]) with uptake less than or equal to that in the liver background (i.e., PSMA-negative lesions) (1). Typical PSMA PET/CT images of low PSMA expression and PSMA-negative lesions are shown in Figures 1 and 2, respectively.
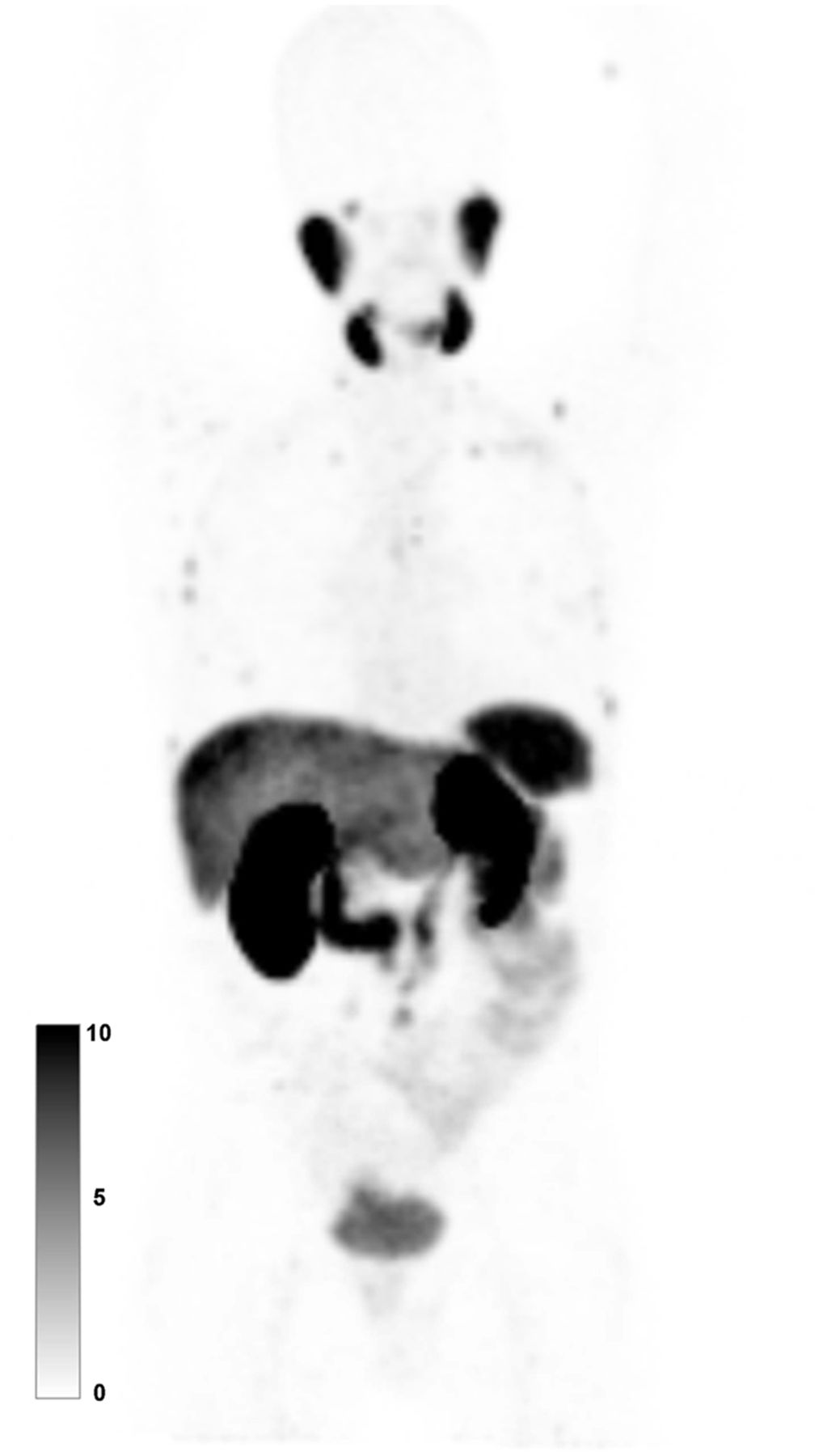
Baseline PSMA PET maximum-intensity projection of patient with metastatic castration-resistant prostate cancer categorized as VISION-PET-SF because of low PSMA expression (i.e., no PSMA-positive [>liver] metastatic lesion). SUVmax of liver and highest-uptake lesion were 9.6 and 6.4, respectively.

Baseline PSMA PET maximum-intensity projection (A), CT image (B), and PSMA PET/CT image (C) of patient with metastatic castration-resistant prostate cancer categorized as VISION-PET-SF because of PSMA-negative lesion (i.e., PSMA-negative metastatic lesion: liver metastasis ≥ 1.0 cm, uptake ≤ liver). One liver metastasis (arrow) showed lower uptake (SUVmax, 4.1) than liver parenchyma (SUVmax, 6.3).
Outcome measures included prostate-specific antigen (PSA) response rates (≥50% PSA decline or any decline), PSA PFS, and OS. Kaplan–Meier curves with log-rank testing and Cox regression analysis were used to compare survival outcomes. The Fisher exact test and logistic regression analysis were used for categoric variable comparisons. The UCLA institutional review board waived written informed consent requirements because of the retrospective design of the analysis (waivers 19-000896 and 21-001565).
RESULTS
Overall, 3 of 304 (1.0%) men were lost to follow-up (n = 2) or had missing DICOM CT images (n = 1) and were excluded. Among 301 men, 272 (90.4%) and 29 (9.6%) were classified as VISION-PET-E and VISION-PET-SF, respectively. Cohort characteristics are provided in Table 1. The VISION-PET-SF patients had more visceral metastasis than VISION-PET-E patients (58.6% vs. 25.4%, P < 0.001). The median number of cycles was lower for VISION-PET-SF patients than for VISION-PET-E patients (2 cycles [interquartile range, 2–3] vs. 3 [interquartile range, 2–4], P = 0.010).
Patient Characteristics
In the VISION-PET-SF group, 8 (2.7%) and 21 (7.0%) of 301 men were deemed to have low–PSMA-expressing or PSMA-negative lesions, respectively (summary images of these 29 patients are provided in Supplemental Figs. 1–29). The PSMA-negative lesions were in lymph nodes (n = 7), bone (n = 1), and visceral organs (liver, n = 4; lung, n = 5; pleura, n = 2; brain, n = 1; and muscle, n = 1).
Our cohort of VISION-PET-E patients was fairly comparable to the cohort included in the VISION trial (analysis set used for imaging-based PFS, Supplemental Table 3) (1). However, the treatment history differed. All VISION patients had been treated with a regimen of androgen receptor signaling inhibitor and taxane. In contrast, 94.5% and 80.1% of the current cohort underwent androgen receptor signaling inhibitor therapy and chemotherapy before MRT, respectively. Nevertheless, the PSA response and OS were comparable between the 2 cohorts (≥50% PSA decline, 50.3% vs. 46.0%; any PSA decline, 71.3% vs. 71.5%; OS, 14.2 mo vs. 14.6 mo).
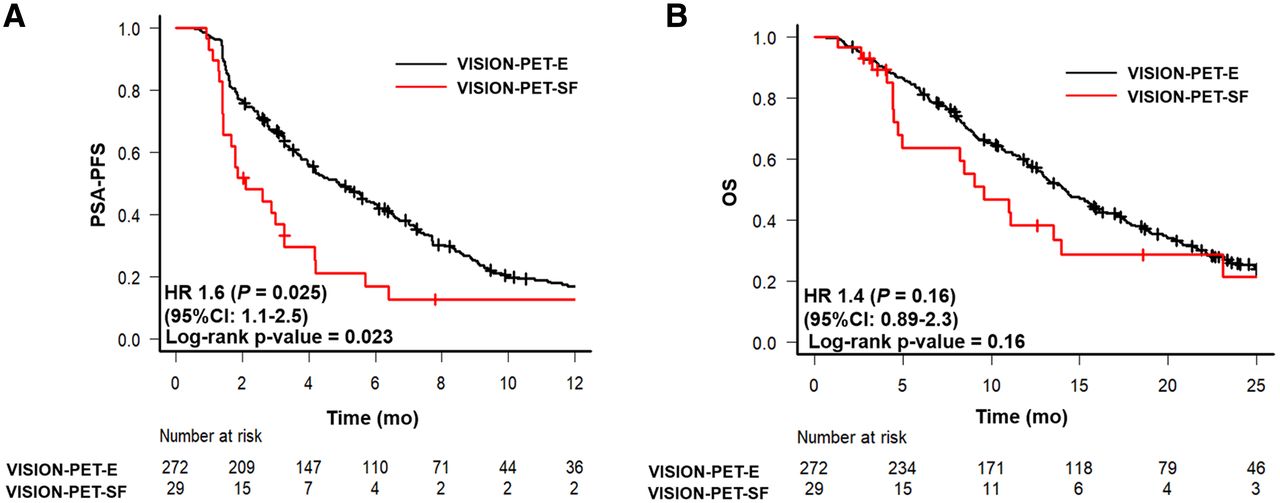
The median follow-up time was 22.5 mo (interquartile range, 12.5–29.2 mo; range, 2.1–62.3 mo). The outcomes of the VISION-PET-E and VISION-PET-SF patients are shown in Table 2. The VISION-PET-SF patients had a significantly worse rate of ≥50% PSA decline, any PSA decline, and median PSA PFS than the VISION-PET-E patients. Although not statistically significant, median OS was 4.6 mo shorter in the VISION-PET-SF patients (Fig. 3).
Outcomes of VISION-PET-E and VISION-PET-SF Patients
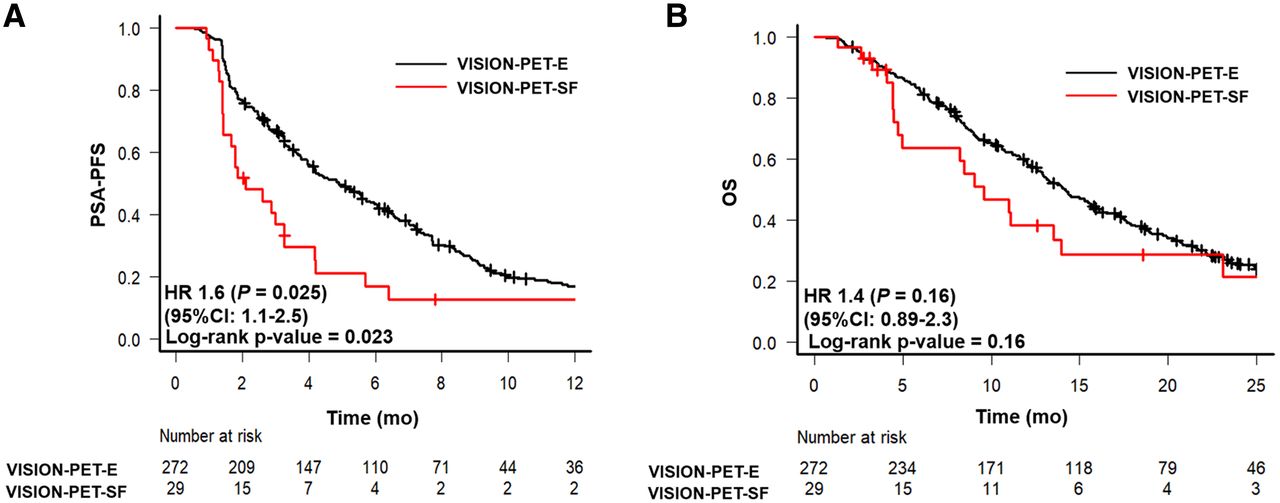
Kaplan–Meier curves of PSA PFS (A) and OS (B) comparing VISION-PET-E and VISION-PET-SF patients. HR = hazard ratio.
In the VISION-PET-SF patients, the patients with PSMA-negative lesions (n = 21) had a shorter OS than those with low PSMA expression (n = 8) (Supplemental Table 4). However, there was no statistical difference in ≥50% PSA decline, any PSA decline, and median PSA PFS between the patients with PSMA-negative lesions and those with low PSMA expression (Fig. 4).

Kaplan–Meier curves of PSA PFS (A) and OS (B) comparing patients with low PSMA expression and PSMA-negative lesion. HR = hazard ratio.
DISCUSSION
The VISION trial used PSMA PET as a biomarker to select patients for 177Lu-PSMA therapy. The VISION-PET-SF rate was “only” 12.6% (126/1,003) (1). Therefore, some have argued that the trial could have been positive even in an unselected population (2).
Here, we report that the VISION-PET-SF patients had worse outcomes than the VISION-PET-E patients in response to 177Lu-PSMA therapy. We retrospectively identified a VISION-PET-SF rate of 9.6% in a cohort of 301 patients who were nevertheless deemed VISION-PET-E and treated with PSMA MRT on the basis of local assessments. Eligibility for treatment was determined by the local clinical investigators at each institution. The VISION PET criteria were released in June 2021 and were not available at the time of initial treatment. There are 2 main explanations for why patients with SF criteria by VISION PET criteria were still treated with 177Lu-PSMA. First, VISION-PET-SF patients with PSMA-negative lesions also had PSMA-positive lesions. The local investigators may have considered that these PSMA-positive lesions were sufficiently suggestive of a treatment response. Second, in VISION-PET-SF patients with low PSMA expression, the local investigators may have considered the PSMA expression PET signal uptake as not sufficiently low to exclude patients from treatment, as there was no consistently predefined threshold to characterize PSMA positivity.
Our cohort did not include patients who were excluded upfront from PSMA MRT by the local clinical investigators. The local SF rate was estimated at around 10%–15% by contributing sites. Thus, SF numbers in our cohort are underestimated and can range from 20% to 25% in unselected populations. Including these patients in the analysis would further enhance the observed outcome differences.
Absent or low target expression limits the response to PSMA-targeted therapies (5,6). However, the key driving parameter of patient outcome seems to be the presence of PSMA-negative lesions that respond poorly to PSMA-targeted MRT and drive the prognostic of the patient (7,8). These lesions can be better identified with 18F-FDG PET than with conventional imaging, as illustrated by the higher PSA response rates and PSA PFS observed in the Australian trials that used 18F-FDG PET in addition to PSMA PET for patient selection (9).
Our results highlight the importance of using baseline PSMA PET/CT to identify patients unlikely to respond to PSMA-targeted therapies and stratify them toward other treatment options. However, the best management of patient with PSMA-negative lesions or with low–PSMA-expressing disease is unknown. Combination with stereotactic body radiation therapy to the largest or most glycolytic (i.e., aggressive) or non–PSMA-expressing lesions together with PSMA-targeted MRT may be one effective synergistic therapeutic approach. Use of this approach alternatively or in combination with other non–PSMA-targeted systemic therapies may be required.
Refinements in patient selection for PSMA MRT are needed to optimize patient outcomes. More comprehensive phenotyping via PET imaging may provide the road map to such refinements. Not characterizing target expression before PSMA-targeted treatment appears now nonethical, as a predictive whole-body imaging biomarker for response to PSMA-targeted therapies is available.
CONCLUSION
Patients with low or no PSMA-expressing lesions as assessed by PSMA PET/CT have a poor response profile to 177Lu-PSMA therapy. Refinements in patient selection for 177Lu-PSMA are needed to optimize patient outcomes.
DISCLOSURE
Jeremie Calais reports prior consulting activities outside the submitted work for Advanced Accelerator Applications, Blue Earth Diagnostics, Curium Pharma, GE Healthcare, Janssen, IBA RadioPharma, POINT Biopharma, Progenics, Radiomedix, and Telix Pharmaceuticals. Johannes Czernin is a founder and holds equity in Sofie Biosciences and Trethera Therapeutics. Intellectual property is class 99–patented by the University of California and licensed to Sofie Biosciences and Trethera Therapeutics. Johannes Czernin was a consultant for Endocyte Inc. (VISION trial steering committee), Actinium Pharmaceuticals, and Point Biopharma outside the submitted work. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the outcome of patients who would have been VISION-PET-SF and who were still treated with 177Lu-PSMA therapy?
PERTINENT FINDINGS: The patients who were VISION-PET-SF showed worse outcomes after 177Lu-PSMA therapy than those who were VISION-PET-E.
IMPLICATIONS FOR PATIENT CARE: Pretherapy PSMA PET/CT is a biomarker of target expression that helps to predict patient response to 177Lu-PSMA therapy. Refinements in patient selection for 177Lu-PSMA are needed to optimize patient outcomes.
ACKNOWLEDGMENTS
(We acknowledge the following individuals for their assistance with the creation of the multicenter study dataset, none of whom were compensated for their contributions and all of whom agreed to have us include their names here: Matthias Eiber (Technical University Munich), Michael Hofman (Peter MacCallum Cancer Center Melbourne), Ken Herrmann and Wolfgang Fendler (University Hospital Essen), Clemens Kratochwil and Uwe Haberkorn (University Hospital Heidelberg), and Ebrahim Delpassand (Excel Diagnostic Center Houston).
Footnotes
Guest editor: Todd Peterson, Vanderbilt University.
Published online Mar. 10, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 28, 2021.
- Accepted for publication February 22, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 99mTc-MIP-1404 SPECT/CT Companion Diagnostic for 177Lu-PSMA Therapy in Metastatic Castration-Resistant Prostate Cancer
- The Role of PSMA PET Parameters as Biomarkers for Response to PSMA-Targeted Radiopharmaceutical Therapy
- Challenges with 177Lu-PSMA-617 Radiopharmaceutical Therapy in Clinical Practice
- Clinical Management of Advanced Prostate Cancer: Where Does Radiopharmaceutical Therapy Fit in the Treatment Algorithm?
- SNMMI Consensus Statement on Patient Selection and Appropriate Use of 177Lu-PSMA-617 Radionuclide Therapy
- SNMMI Consensus Statement on Patient Selection and Appropriate Use of 177Lu-PSMA-617 Radionuclide Therapy
- Is 18F-FDG PET Needed to Assess 177Lu-PSMA Therapy Eligibility? A VISION-like, Single-Center Analysis
- 177Lu-PSMA-I&T for Treatment of Metastatic Castration-Resistant Prostate Cancer: Prognostic Value of Scintigraphic and Clinical Biomarkers
- Clinical Trials of Prostate-Specific Membrane Antigen Radiopharmaceutical Therapy
- Reply: What Does an Imaging "Selection" Claim Actually Mean?