


Article Figures & Data
Figures
- FIGURE 1.
Algorithm for imaging investigations in primary hyperparathyroidism. See also Table 1 for suggested activities and acquisition protocol. *Dual-tracer subtraction scan can be positive in patients with previous negative dual-phase imaging results. †Suggestive lesion seen only on nuclear imaging in area not accessible to US should not be considered discordant or inconclusive. ‡Contrast-enhanced arterial-phase CT acquisition can be added (it can improve PPV of PET/CT in difficult cases). §To be considered only in repeat surgery cases with negative first-line and second-line imaging results.
- FIGURE 2.
Simultaneous dual-tracer 99mTc-sestamibi and 123I scan in 39-y-old patient with PHPT. (A) Parallel-hole collimator images with 99Tc-sestamibi, 123I, and subtraction. Parallel-hole subtraction image shows residual focus on right side of neck, barely visible focus on left side (arrow), and no ectopic foci. (B) Pinhole images over thyroid area with 99Tc-sestamibi, 123I, and subtraction. Pinhole subtraction image clearly shows 2 residual foci. Surgery confirmed diagnosis of double adenomas, and calcium level at 6 mo was normal. This example shows better resolution offered by pinhole images and reveals importance of computer subtraction, as visual comparison alone could have missed left-side focus. Computer subtraction should be well balanced, avoiding oversubtraction.
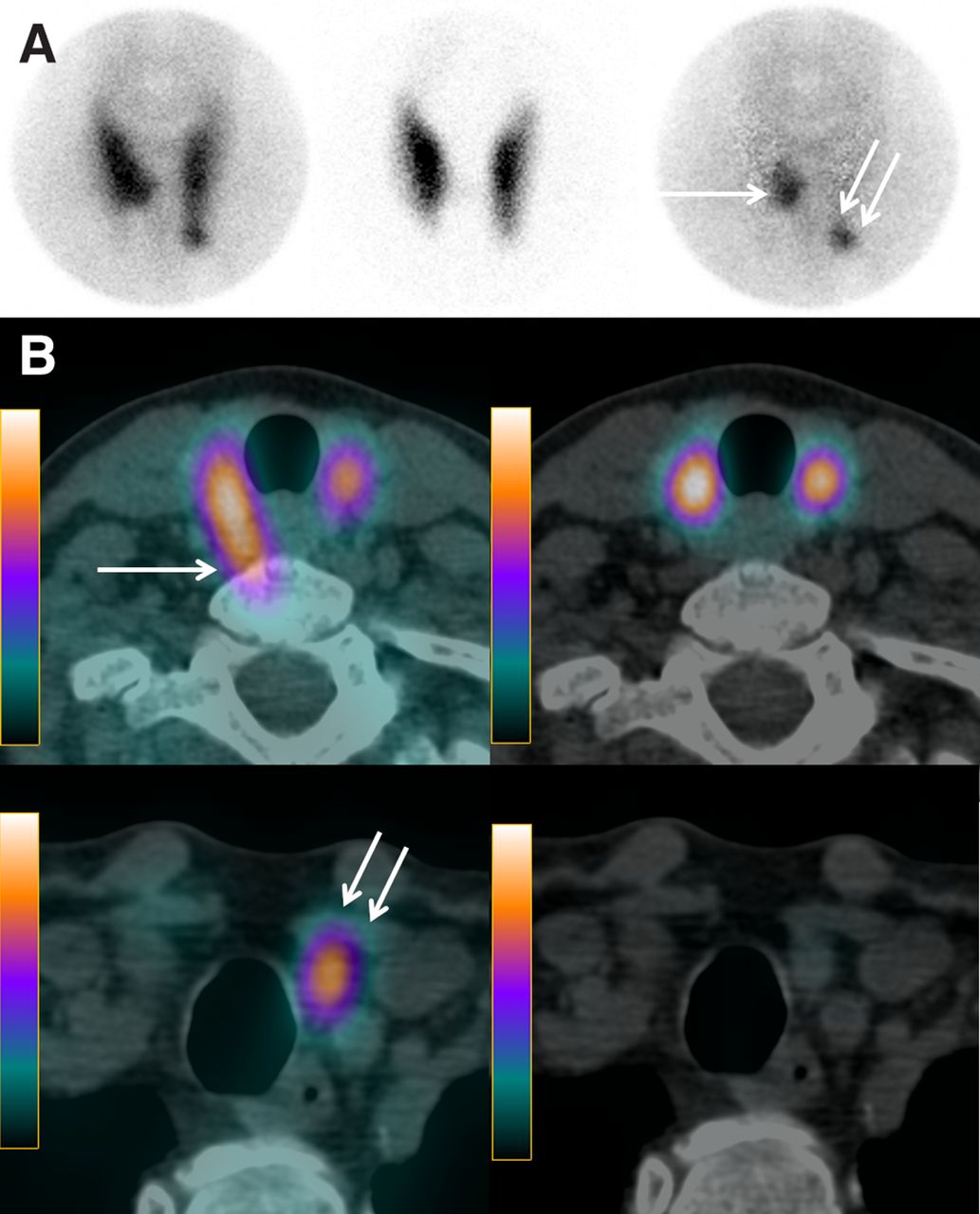
- FIGURE 3.
Simultaneous dual-tracer 99mTc-sestamibi and 123I scan in 62-y-old patient with PHPT. (A) Pinhole images of thyroid area with 99mTc-sestamibi, 123I, and subtraction. Pinhole subtraction image clearly identifies 2 residual foci: 1 at inner part of lower third of right thyroid lobe (arrow) and other at lower pole of left thyroid lobe (double arrow). (B) Axial SPECT/CT fusion images with 99mTc-sestamibi (right) and 123I (left), obtained at 2 different levels. On SPECT/CT axial views, right parathyroid lesion is located posteriorly, in paraesophageal position (arrow). This location is typical of prolapsed superior parathyroid gland (minor ectopia). Left inferior parathyroid lesion (double arrow) is located below lower pole of left thyroid lobe. Calcium level 6 mo after resection of 2 adenomas was normal.
- FIGURE 4.
84-y-old patient with PHPT and history of total thyroidectomy. Neck ultrasound results were negative. Simultaneous dual-tracer 99mTc-sestamibi and 123I parathyroid scan was performed after patient was instructed to withhold thyroid hormone therapy for 2 wk. (A) Pinhole images of neck show two 99mTc-sestamibi–avid foci (1 on each side of neck), but 123I scan clearly shows that focus on left side corresponds to thyroid remnant (arrow). (B) 99mTc-sestamibi and 123I SPECT/CT axial views without subtraction reveal posteriorly seated right parathyroid lesion and left thyroid remnant. Targeted surgery could be performed with resection of 600-mg right parathyroid adenoma.
- FIGURE 5.
18F-fluorocholine PET/CT performed 35 min after intravenous injection of 18F-fluorocholine in 71-y-old patient with PHPT. Results of neck ultrasonography and dual-phase 99mTc-sestamibi parathyroid scan performed at another institution before referral were negative. 18F-fluorocholine PET (A) with maximum-intensity-projection and axial view images show 18F-fluorocholine–avid focus corresponding on axial PET/CT fusion and CT images (B) to small tissue lesion behind right sternoclavicular junction (arrows). Parathyroid adenoma (500 mg) was resected.
- FIGURE 6.
18F-fluorocholine PET/CT in 74-y-old patient with PHPT. Neck ultrasonography described doubtful left inferior parathyroid lesion, and 99mTc-sestamibi/123I subtraction scintigraphy results were negative. 18F-fluorocholine PET/CT included conventional nonenhanced plus contrast-enhanced arterial-phase CT acquisitions. (A) Maximum-intensity-projection 18F-fluorocholine PET image reveal faint cervical focus (superior arrow) and multiple mediastinal foci (inferior arrow). (B) PET/CT fusion and arterial-phase contrast-enhanced CT (CECT) and PET axial images show choline-avid lesion with high contrast enhancement contiguous to left posterior side of esophagus, suggestive of ectopic parathyroid lesion (arrows). (C) PET/CT fusion and arterial-phase CECT and PET axial images of superior mediastinum show choline-avid lymph node with low contrast enhancement (arrows). At surgery, retroesophageal parathyroid adenoma was resected.







Tables
Technique Radiopharmaceutical* Effective dose (mSv)† Protocol of administration Suggested acquisition protocol Total acquisition time 99mTc-sestamibi/123I (subtraction) 123I (∼12 MBq) 1.5 T0: 123I (intravenous or oral) 99mTc and 123I simultaneous dual-isotope acquisition starting 3–5 min after 99mTc-sestamibi injection‡ <1 h 99mTc-sestamibi (∼600 MBq) 5.4 T+2 h: 99mTc-sestamibi (intravenous) Image of thyroid/parathyroid bed with pinhole collimator (15 min) Planar image of neck and mediastinum (5 min)§ Then, dual-isotope SPECT/CT acquisition (∼25 min) 99mTc-sestamibi (dual-phase) 99mTc-sestamibi (740–900 MBq) 6.7–8.1 T0: 99mTc-sestamibi (intravenous) T+15 min (early phase); planar image of neck and mediastinum (5 min)§ ∼90 min in 2 sessions Image of thyroid/parathyroid bed with pinhole collimator (15 min) T+2 h (delayed phase); same protocol as early phase SPECT/CT (∼25 min) at early, delayed, or both phases 18F-fluorocholine PET/CT (± CECT) 18F-fluorocholine (100–200 MBq or 2–3 MBq/kg) 2.0–4.0 T0: 18F-fluorocholine (intravenous) PET acquisition starting ∼45 min (30–60 min) after injection¶ 20–30 min Nonenhanced CT from mandible to carina If arterial-phase CECT is added, then acquisition starts ∼30 s (25–40 s) after beginning of contrast medium injection * Values in parentheses are activities.
↵† Not including CT dose (25). For 123I, we considered thyroid uptake of 20%.
↵‡ Example of nonoverlapping windows (29): for 99mTc, 140 keV ± 7% (130–150 keV); for 123I, 159 keV −4% to +10% (153–175 keV).
↵§ Includes submandibular salivary glands and upper part of myocardium.
↵¶ Early phase (∼ 5 min after injection) is additionally obtained by some authors.
CECT = contrast-enhanced CT; T = time.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Visual Abstract
- Abstract
- IMAGING IS RECOMMENDED BEFORE FIRST PARATHYROID SURGERY IRRESPECTIVE OF SURGICAL APPROACH
- ADVANTAGES AND DISADVANTAGES OF TARGETED SURGERY: IMPLICATIONS REGARDING CHOICE OF IMAGING
- WHY IS 99mTc-SESTAMIBI/123I SUBTRACTION IMAGING BETTER OPTION THAN DUAL-PHASE SESTAMIBI SCANNING FOR GUIDING TARGETED SURGERY?
- SECOND-LINE IMAGING STRATEGY WHEN SCINTIGRAPHY AND NECK ULTRASOUND RESULTS ARE NEGATIVE, DISCORDANT, OR INCONCLUSIVE
- IS IT TOO EARLY TO PROPOSE 18F-FLUOROCHOLINE PET/CT AS FIRST-LINE IMAGING?
- LOCALIZATION PROCEDURES BEFORE REPEAT SURGERY FOR PERSISTENT OR RECURRENT HYPERPARATHYROIDISM
- CONCLUSION
- DISCLOSURE
- ACKNOWLEDGMENT
- REFERENCES
- Figures & Data
- Info & Metrics