


Visual Abstract

Abstract
Primary hyperparathyroidism is a common and potentially debilitating endocrine disorder for which surgery is the only curative treatment. Preoperative imaging is always recommended, even in cases of conventional bilateral neck exploration, with a recognized role for 99mTc-sestamibi scintigraphy in depicting ectopic parathyroid lesions. Scintigraphy can also play a major role in guiding a targeted, minimally invasive parathyroidectomy. However, the ability to recognize multiple-gland disease (MGD) varies greatly depending on the imaging protocol used. Preoperative diagnosis of MGD is important to reduce the risks of conversion to bilateral surgery or failure. In this article we discuss imaging strategies before first surgery as well as in the case of repeat surgery for persistent or recurrent primary hyperparathyroidism. We describe a preferred algorithm and alternative options. Dual-tracer 99mTc-sestamibi/123I subtraction scanning plus neck ultrasound is the preferred first-line option. This approach should improve MGD detection and patient selection for minimally invasive parathyroidectomy. Second-line imaging procedures in case of negative or discordant first-line imaging results are presented. High detection rates can be obtained with 18F-fluorocholine PET/CT or with 4-dimensional CT. The risk of false-positive results should be kept in mind, however. Adding a contrast-enhanced arterial-phase CT acquisition to conventional 18F-fluorocholine PET/CT can be a way to improve accuracy. We also briefly discuss other localization procedures, including 11C-methionine PET/CT, MRI, ultrasound-guided fine-needle aspiration, and selective venous sampling for parathyroid hormone measurement.
Primary hyperparathyroidism (PHPT) is a common endocrine disorder resulting from the autonomous production of parathyroid hormone (PTH) from 1 or more abnormal parathyroid glands (1–4). Its incidence increases with age and is higher in women (2,4). In the United States and Western Europe, fewer than 20% of patients present with renal complications (kidney stones, nephrocalcinosis), skeletal complications (fracture, osteitis fibrosa cystica, bone pain), or symptomatic hypercalcemia; most cases of PHPT are incidentally discovered (2). However, imaging studies in asymptomatic patients may show kidney stones, osteoporosis, or vertebral fractures, and progression occurs in up to 40% of patients during follow-up (3,4). PHPT is characterized by hypercalcemia and elevated or inappropriately normal serum PTH levels. A diagnosis of normocalcemic PHPT can be made only after the elimination of secondary causes of hyperparathyroidism (1–3).
PHPT is caused by a solitary parathyroid adenoma in 80% of cases, whereas multiple-gland disease (MGD), with mostly double adenomas or 4-gland hyperplasia, accounts for 15%–20% of cases and parathyroid cancer accounts for fewer than 1% of cases (2,3). MGD is often sporadic (5) but can also be linked to a hereditary disease. Inherited forms of PHPT include multiple endocrine neoplasia (MEN) syndromes of types MEN1, MEN4, and MEN2A, hyperparathyroidism–jaw tumor syndrome (∼15% risk of parathyroid carcinoma), and familial isolated PHPT (2).
Surgery is the only curative treatment for PHPT. Various medical therapies can increase bone mineral density or reduce serum levels of calcium, but no single drug can do both (2). Parathyroidectomy increases bone mineral density, decreases the risk of fracture, decreases the incidence of nephrolithiasis, and may halt the decline in renal function (1–4,6). Surgery is indicated in any patient younger than 50 years old, any symptomatic patient, and asymptomatic patients with signs of subclinical end-organ involvement—with some variations between guidelines (1,6). Parathyroid imaging studies have no role in establishing the diagnosis of PHPT (1,6); however, imaging is very important for operative planning after the decision to proceed with parathyroidectomy is made (1,6–8).
Here we discuss the aims of preoperative imaging and suggest an imaging algorithm for use before the first surgery as well as in the case of repeat surgery for persistent or recurrent disease.
IMAGING IS RECOMMENDED BEFORE FIRST PARATHYROID SURGERY IRRESPECTIVE OF SURGICAL APPROACH
The surgical approach to PHPT can vary from bilateral cervical exploration to minimally invasive parathyroidectomy (MIP). The choice depends on preoperative localization study findings, family history, the presence or absence of concomitant thyroid disease, and the preference of the surgeon (7). Parathyroid imaging has become a standard preoperative procedure for locating abnormal parathyroid tissue (1,6–8). Sestamibi scintigraphy and neck ultrasound are the most widely used, often so in conjunction, seeking for concordance to increase accuracy (1,6–8). Imaging is not a substitute for surgical expertise, as results can be negative or inaccurate or may locate only part of the hyperfunctioning parathyroid tissue. Parathyroid surgery requires expertise because the patient may harbor MGD (2,3,5); in about 16% of patients, parathyroid lesions can be ectopic (9–11); the hyperfunctioning tissue may involve a supernumerary parathyroid gland (11,12); nodular thyroid disease can make parathyroid surgery more difficult; and parathyroid tumors can be very small—increasingly so because of earlier diagnosis and surgical decisions, with a reported median weight of 0.5 g for adenomas (13). This evolution also leads to greater challenges for imaging techniques.
Although bilateral neck exploration without any preoperative imaging is curative in 92%–95% of patients (14) and minor ectopias can be easily depicted by an experienced surgeon (e.g., prolapsed superior gland in the tracheoesophageal groove or inferior gland in the thyrothymic ligament), some parathyroid glands present major ectopias (e.g., superior glands in a retroesophageal or retropharyngeal position; inferior glands that are undescended, within the carotid sheath, or overmigrated into the mediastinum; or parathyroid glands completely buried in the thyroid parenchyma) (12). The maneuvers to search for an elusive gland (15) may increase the risk of perioperative complications (e.g., transient/permanent hypoparathyroidism, wound infection, postoperative hemorrhage, or recurrent laryngeal nerve injury). Thus, preoperatively identifying an ectopic gland can reduce the extent of dissection in a sizable minority of patients and avoid some surgical failures (e.g., low thoracic parathyroid glands) (9,10,16).
99mTc-sestamibi imaging has a recognized high sensitivity and high positive predictive value (PPV) for ectopic parathyroid lesions (9,10).
ADVANTAGES AND DISADVANTAGES OF TARGETED SURGERY: IMPLICATIONS REGARDING CHOICE OF IMAGING
MIP and bilateral neck exploration are both appropriate surgeries (6,7). A randomized study showed an advantage for unilateral surgery in terms of operative time and incidence of transient hypocalcemia, whereas the rate of failure was not significantly higher (8.5% for unilateral surgery vs. 4.5% for bilateral surgery) (17). A limit to this comparison, however, is that only patients randomized to the unilateral group received a sestamibi scan (17). Bilateral surgery with preoperative imaging is associated with a higher success rate, a shorter operative time, and lower risks of complications than exploratory bilateral surgery (16).
The success of MIP depends on the ability to identify the 15%–20% of patients with MGD. Repeat surgeries are associated with increased costs and morbidity. The use of intraoperative PTH monitoring has been recommended (6). PTH concentrations may, however, decrease (50% decrease 10 min after tumor resection) even though other lesions are still present (18). The mean MGD rates are 19.3% with bilateral exploration but only 5.3% with targeted surgery (P < 0.001) (19). Many studies recently emphasized that the risk of recurrence may be greater than previously believed. Lou et al. reported a recurrence rate of 14.8% over a 10-y follow-up period (20).
Another point to consider is that MIP might require conversion to bilateral surgery in about 20% of cases (21). Conversion is often due to imaging failure (e.g., incorrect localization, missed MGD).
The success of the MIP approach can thus be heavily dependent on the use of a good preoperative imaging strategy. The role of imaging should be even more critical when access to intraoperative PTH is limited. In addition to accuracy, techniques proposed for routine preoperative imaging should be available, affordable, approved, and reimbursed by health insurance and should have low rates of contraindications.
Figure 1 shows the algorithm for preoperative imaging, proposing a first-line approach using neck ultrasound plus 1 radionuclide imaging technique. For radionuclide imaging, we indicate a preferred option and alternative options (Fig. 1), as discussed in the following paragraphs.

Algorithm for imaging investigations in primary hyperparathyroidism. See also Table 1 for suggested activities and acquisition protocol. *Dual-tracer subtraction scan can be positive in patients with previous negative dual-phase imaging results. †Suggestive lesion seen only on nuclear imaging in area not accessible to US should not be considered discordant or inconclusive. ‡Contrast-enhanced arterial-phase CT acquisition can be added (it can improve PPV of PET/CT in difficult cases). §To be considered only in repeat surgery cases with negative first-line and second-line imaging results.
Neck ultrasound is easily available and can be performed by radiologists or trained surgeons and endocrinologists. It is a low-cost, nonirradiating technique that also offers valuable additional information on thyroid morphology. Its effectiveness strongly depends on the operator’s skills. However, neck ultrasound is not accurate enough to be used alone, as it has low sensitivity for ectopic lesions (10) and MGD (22).
WHY IS 99mTc-SESTAMIBI/123I SUBTRACTION IMAGING BETTER OPTION THAN DUAL-PHASE SESTAMIBI SCANNING FOR GUIDING TARGETED SURGERY?
The systematic review by Ruda et al. emphasized the role of 99mTc-sestamibi scintigraphy in PHPT but identified differences in detection sensitivity based on the underlying pathology: sensitivities of 88.44% for solitary adenomas, 44.46% for multigland hyperplasia, and 29.95% for double adenomas (22). As pointed out by Kettle and O’Doherty, however, the systematic review did not separate the different 99mTc-sestamibi protocols (23).
Parathyroid scintigraphy protocols using a single-tracer dual-phase technique and a dual-tracer subtraction technique were previously discussed (23–27). Regarding dual-tracer scintigraphy, 99mTc-sestamibi/123I subtraction imaging is the reference protocol (23,24). With 99mTc-pertechnetate as the thyroid tracer, only successive acquisition is possible, and the subtraction image may be affected by artifacts because of patient motion between the 2 sets of acquisitions (25). Simultaneous acquisition of 99mTc-sestamibi and 123I images reduces acquisition time, allows perfectly coregistered subtraction, and offers excellent sensitivity (16,24,28,29).
Suggested acquisition protocols for 99mTc-sestamibi/123I dual-isotope imaging and for 99mTc-sestamibi dual-phase imaging, with activities used, dosimetry, and camera occupation time, are shown in Table 1. Pinhole acquisition over the thyroid/parathyroid bed area offers enhanced count detection, spatial resolution, and sensitivity (30). SPECT/CT offers anatomic precision (31,32).
Summary of Techniques Used for Parathyroid Scintigraphy and PET/CT
Dual-phase 99mTc-sestamibi scintigraphy based on a comparison of early (∼15 min) and delayed (∼2 h) planar images misses MGD most of the time (33). Among 11 MGD patients, scintigraphy results were negative in 2 and incorrectly suggested a single adenoma in 9 (33). Even when dual-phase scintigraphy is combined with SPECT/CT, its ability to detect MGD remains unsatisfactory. Sandqvist et al. performed 99mTc-sestamibi SPECT/CT at 10 min and 90 min in 160 patients (34). Nine patients had MGD at surgery. Preoperative SPECT/CT had suggested a single adenoma in 8 of them (34). When dual-phase SPECT/CT was combined with 4-dimensional (4D) CT, MGD was predicted in only 3 of 9 patients (34). Therefore, we believe that single-tracer dual-phase scintigraphy cannot reliably guide targeted parathyroid surgery.
Comparative studies have consistently shown that dual-isotope 99mTc-sestamibi/123I subtraction imaging offers higher accuracy than 99mTc-sestamibi dual-phase imaging. Also, all 3 studies that used a pinhole collimator for this comparison obtained similar results (28,29,35). Caveny et al. studied 37 patients (28). 99mTc-sestamibi/123I subtraction imaging showed higher sensitivity than dual-phase imaging (94% vs. 66%; P < 0.01), with fewer false-positive results (0 vs. 2). There was no benefit of adding delayed images to the dual-tracer protocol (28). Krakauer et al. performed a head-to-head comparison in 91 patients (97 parathyroid lesions at surgery) (35). Sensitivities were 93% for 99mTc-sestamibi/123I subtraction imaging and 65% for dual-phase scintigraphy (P < 0.001) (35). 123I is available in Europe on a daily basis and costs approximately U.S. $150 plus delivery for 3 patient doses (35).
Simultaneous 99mTc-sestamibi/123I imaging with pinhole acquisition has a high sensitivity for diagnosing MGD, exceeding 50% in most studies (35–38). MGD is commonly characterized by the presence of glands of unequal size and intensity (36). Therefore, computer subtraction should be performed in gradual steps, with visual monitoring, avoiding oversubtraction. Figure 2 shows the importance of pinhole acquisition for optimal sensitivity, and Figure 3 offers an example of the anatomic information obtained with SPECT/CT. 99mTc-sestamibi and 123I SPECT/CT images can be displayed side-by-side for visual comparison (Fig. 3). Subtraction can also be performed on 3-dimensional data (39,40), but obtaining a well-balanced subtraction is technically more demanding than on planar pinhole images, and the possibility of edge artifacts should be kept in mind.

Simultaneous dual-tracer 99mTc-sestamibi and 123I scan in 39-y-old patient with PHPT. (A) Parallel-hole collimator images with 99Tc-sestamibi, 123I, and subtraction. Parallel-hole subtraction image shows residual focus on right side of neck, barely visible focus on left side (arrow), and no ectopic foci. (B) Pinhole images over thyroid area with 99Tc-sestamibi, 123I, and subtraction. Pinhole subtraction image clearly shows 2 residual foci. Surgery confirmed diagnosis of double adenomas, and calcium level at 6 mo was normal. This example shows better resolution offered by pinhole images and reveals importance of computer subtraction, as visual comparison alone could have missed left-side focus. Computer subtraction should be well balanced, avoiding oversubtraction.

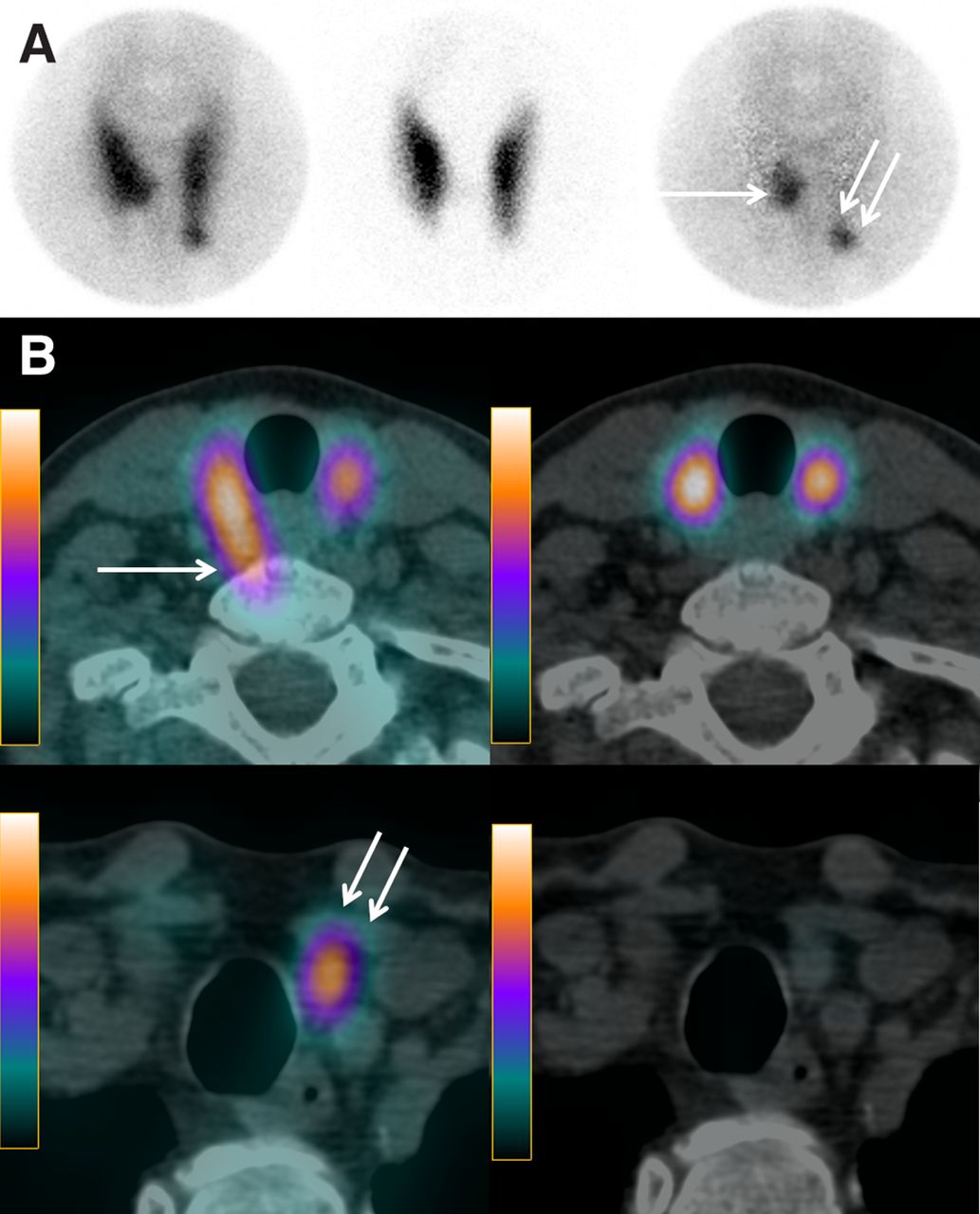
Simultaneous dual-tracer 99mTc-sestamibi and 123I scan in 62-y-old patient with PHPT. (A) Pinhole images of thyroid area with 99mTc-sestamibi, 123I, and subtraction. Pinhole subtraction image clearly identifies 2 residual foci: 1 at inner part of lower third of right thyroid lobe (arrow) and other at lower pole of left thyroid lobe (double arrow). (B) Axial SPECT/CT fusion images with 99mTc-sestamibi (right) and 123I (left), obtained at 2 different levels. On SPECT/CT axial views, right parathyroid lesion is located posteriorly, in paraesophageal position (arrow). This location is typical of prolapsed superior parathyroid gland (minor ectopia). Left inferior parathyroid lesion (double arrow) is located below lower pole of left thyroid lobe. Calcium level 6 mo after resection of 2 adenomas was normal.
99mTc-sestamibi uptake by thyroid nodules complicates the interpretation of all parathyroid scintigraphy protocols. The 123I scan can help by clarifying thyroid morphology and function, recognizing a false-positive result when the thyroid nodule takes up iodine. Sestamibi-avid/iodine-cold thyroid nodules carry a higher risk of malignancy, and fine-needle biopsy can aid in the decision about whether additional thyroid surgery is required.
The 123I scan is necessary even in cases of previous thyroidectomy, as 123I will allow the correct identification of residual thyroid tissue (Fig. 4), which can be mistaken for a parathyroid lesion on neck ultrasound, 99mTc-sestamibi single-tracer scintigraphy, or other imaging modalities. Useless dissection in a neck that has undergone previous surgery can thus be avoided (Fig. 4).

84-y-old patient with PHPT and history of total thyroidectomy. Neck ultrasound results were negative. Simultaneous dual-tracer 99mTc-sestamibi and 123I parathyroid scan was performed after patient was instructed to withhold thyroid hormone therapy for 2 wk. (A) Pinhole images of neck show two 99mTc-sestamibi–avid foci (1 on each side of neck), but 123I scan clearly shows that focus on left side corresponds to thyroid remnant (arrow). (B) 99mTc-sestamibi and 123I SPECT/CT axial views without subtraction reveal posteriorly seated right parathyroid lesion and left thyroid remnant. Targeted surgery could be performed with resection of 600-mg right parathyroid adenoma.
SECOND-LINE IMAGING STRATEGY WHEN SCINTIGRAPHY AND NECK ULTRASOUND RESULTS ARE NEGATIVE, DISCORDANT, OR INCONCLUSIVE
Discordant Imaging: Causes and Consequences
With concordant sestamibi imaging and neck ultrasound, the success rate of MIP is high (6,7). Patients with discordant imaging, in whom only 1 study is positive, or with diverging conclusions as to the site of a lesion(s) constitute a challenging subset of patients (41). These patients usually receive either routine bilateral surgery or MIP under intraoperative PTH monitoring, with a high risk of conversion to bilateral surgery (41).
Causes of discrepancies are multiple. Some limitations are inherent to neck ultrasound (10,22). When neck ultrasound results are negative and 99mTc-sestamibi depicts a well-identified parathyroid lesion in an area less accessible to ultrasound imaging (e.g., retrotracheal, retroesophageal, or upper mediastinal), such a case should not be considered discordant or inconclusive. Some parathyroid lesions may have low 99mTc-sestamibi uptake because of their consistency (e.g., cystic lesions) or low content in oxyphil cells (25). With a dual-phase technique, negativity may also result from rapid tracer washout (25). Factors associated with difficult identification and characterization with either technique can also lead to discrepancies; these include a small parathyroid lesion or the presence of nodular thyroid disease. In MGD, discrepancies are frequent (41) because of limitations of techniques (33) or “satisfaction of search” (42). Finally, the experience of the operator also plays an important role (e.g., parathyroid lesions with atypical ultrasound features) (42).
Discordance can sometimes be resolved by a second neck ultrasound performed by an experienced operator aware of sestamibi findings (42). More generally, the order in which neck ultrasound and sestamibi imaging should be performed has been investigated little. Because of widespread availability, neck ultrasound is often obtained first. In a retrospective analysis of 63 patients, the sensitivity and PPV of neck ultrasound were better when it was performed after 99mTc-sestamibi SPECT/CT (90.9% and 100% vs. 56.6% and 72.2%, respectively; P < 0.05), whereas the performance of 99mTc-sestamibi SPECT/CT was not improved by knowledge of neck ultrasound results (43). Validation of these findings in a prospective setting may have important practical consequences.
Although the risk of MGD is somewhat higher with discordant imaging, most patients (∼70%) have a single adenoma at surgery (41). Therefore, instead of choosing a more extensive surgical exploration, the use of second-line imaging would be desirable (43), as suggested in the algorithm (Fig. 1).
Implications of Negative Parathyroid Scan and Neck Ultrasound Results
Although patients with nonlocalizing imaging results remain surgical candidates (6), an experienced multidisciplinary team should be entrusted with the case. Several studies have indeed reported that patients with negative imaging results may require more extensive exploratory surgery (44) and are exposed to a higher rate of surgical failure (44,45). In a large series from the Mayo Clinic, surgery was curative in 97.5% of patients with localization on the 99mTc-sestamibi/123I scan, compared with 90.4% when the scan results were negative (P < 0.001) (45).
Dual-Tracer Subtraction Imaging in Patients with Negative Dual-Phase Scintigraphy Results
As mentioned in the algorithm (Fig. 1), obtaining positive 99mTc-sestamibi/123I scan results after negative single-tracer imaging results is not rare (e.g., when negative dual-phase imaging results are due to rapid tracer washout) (46).
18F-Fluorocholine (or 11C-Choline) PET/CT
After incidental findings of a parathyroid adenoma during 11C-choline PET imaging for prostate cancer, many teams investigated 18F-fluorocholine (or 11C-choline) PET in PHPT patients with negative/inconclusive 99mTc-sestamibi and neck ultrasound results (47–52). These PET tracers open new avenues for radionuclide imaging of parathyroid glands (27,39,53,54). The best imaging time for 18F-fluorocholine PET is still subject to discussion, but most parathyroid lesions are better defined (better lesion-to-thyroid contrast) at 60 min than at 5 min (55). Some teams image at more than 1 time, whereas most use single-time-point imaging between 30 min (48,51) and 60 min (49) after injection.
Most studies are retrospective, with many patients not being offered surgery, rendering measurements of test performance difficult. Quak et al. prospectively investigated 18F-fluorocholine PET/CT in 25 patients with negative/inconclusive dual-phase 99mTc-sestamibi (including delayed SPECT/CT) and neck ultrasound results (49). Twenty-four patients received surgery. Importantly, surgery was targeted in 18 cases. Analysis per lesion yielded a sensitivity of 18F-fluorocholine of 91.3% and a PPV of 87.5% (49). Only 1 patient had MGD, fewer than expected in this setting (41,44,45), calling into question the sensitivity of 18F-fluorocholine PET/CT for MGD (56). With regard to surgical outcomes, surgical failure occurred in 3 patients (13%) (49). The authors warned about the risk associated with considering equivocal 18F-fluorocholine PET/CT results positive (49).
Parathyroid lesions identified by second-line 18F-fluorocholine PET/CT imaging are often small or deeply seated or have a bony interposition (Fig. 5). Lower resolution and attenuation may contribute to the negativity of sestamibi imaging results. With dual-phase 99mTc-sestamibi imaging, rapid washout can also be a factor.

18F-fluorocholine PET/CT performed 35 min after intravenous injection of 18F-fluorocholine in 71-y-old patient with PHPT. Results of neck ultrasonography and dual-phase 99mTc-sestamibi parathyroid scan performed at another institution before referral were negative. 18F-fluorocholine PET (A) with maximum-intensity-projection and axial view images show 18F-fluorocholine–avid focus corresponding on axial PET/CT fusion and CT images (B) to small tissue lesion behind right sternoclavicular junction (arrows). Parathyroid adenoma (500 mg) was resected.
11C-Methionine PET/CT
Some studies reported good sensitivity when the amino acid tracer 11C-methionine was used for second-line imaging (57), but this tracer is less available than 18F-fluorocholine. The 2 tracers were compared in patients with negative/inconclusive 99mTc-sestamibi SPECT results (58). Surgery was successful in 21 of 26 patients (81%). Per-lesion sensitivity was superior with 18F-fluorocholine versus 11C-methionine (84% vs. 72%; P = 0.001). The PPVs were 93% and 95%, respectively (58).
Parathyroid 4-Dimensional CT
4D CT uses the dynamics of contrast enhancement (noncontrast phase, followed by contrast-enhanced arterial and venous CT phases) to identify abnormal parathyroid glands. A sensitivity of 89% was reported in patients with negative first-line imaging results but with a PPV of 74% (59).
Some limitations of 4D CT need to be recognized. Discordance with intraoperative findings was found in 123 of 411 patients (30%) (60). MGD, lesions of less than or equal to 10 mm, nodular thyroid, and parathyroid lesion in the inferior position were independently associated with discordant 4D CT results.
4D CT is probably not well adapted to routine first-line imaging in PHPT, as it requires substantial expertise, delivers a high radiation dose to the neck and upper thorax, and requires injection of iodinated contrast medium in a population in whom renal impairment is not uncommon.
MRI and PET/MRI
Parathyroid MRI techniques are also evolving. Some teams investigated the use of 18F-fluorocholine PET/MRI (50,61,62), with (61) or without (62) MRI contrast media. More studies are needed to define the role of this technique.
18F-Fluorocholine PET/CT with Contrast Enhancement
Piccardo et al. prospectively investigated the value of fully integrated 18F-fluorocholine PET with 4D CT in 44 PHPT patients with negative/inconclusive first-line imaging results (63). The detection rate with 18F-fluorocholine PET/4D CT (72.7%) was significantly higher (P < 0.05) than with conventional 18F-fluorocholine PET/CT (56.8%) or 4D CT (54.5%) (63). Six lesions missed by 18F-fluorocholine PET but identified by 18F-fluorocholine PET/4D CT were very close to the thyroid. It is worth mentioning that imaging started 10 min after 18F-fluorocholine injection—an approach that might not offer the highest parathyroid-to-thyroid contrast. In a retrospective analysis, Pretet et al. found the sensitivity of 18F-fluorocholine PET/CT superior to that of 4D CT (88% vs. 66%; P = 0.01), with no significant improvement with integrated 18F-fluorocholine PET/4D CT (sensitivity, 92%) (64).
At University Hospitals of Bordeaux, 18F-fluorocholine PET/CT for inconclusive first-line imaging is performed using nonenhanced CT plus a contrast-enhanced arterial-phase CT acquisition, in the absence of contraindications, with the purpose of reducing potential 18F-fluorocholine false-positive results from reactive lymph nodes (Fig. 6). False-positive results with 18F-fluorocholine PET are mostly due to thyroid nodules (47) and reactive lymph nodes (49,55,65). The precontrast CT discriminates parathyroid lesions from the thyroid (higher spontaneous density), whereas the arterial phase best discriminates parathyroid lesions (moderate to high enhancement) from lymph nodes (low enhancement) (Fig. 6). Eliminating the venous phase of conventional 4D CT helps reduce the radiation dose (65).

18F-fluorocholine PET/CT in 74-y-old patient with PHPT. Neck ultrasonography described doubtful left inferior parathyroid lesion, and 99mTc-sestamibi/123I subtraction scintigraphy results were negative. 18F-fluorocholine PET/CT included conventional nonenhanced plus contrast-enhanced arterial-phase CT acquisitions. (A) Maximum-intensity-projection 18F-fluorocholine PET image reveal faint cervical focus (superior arrow) and multiple mediastinal foci (inferior arrow). (B) PET/CT fusion and arterial-phase contrast-enhanced CT (CECT) and PET axial images show choline-avid lesion with high contrast enhancement contiguous to left posterior side of esophagus, suggestive of ectopic parathyroid lesion (arrows). (C) PET/CT fusion and arterial-phase CECT and PET axial images of superior mediastinum show choline-avid lymph node with low contrast enhancement (arrows). At surgery, retroesophageal parathyroid adenoma was resected.
Christakis et al. reported on 12 patients who had persistent/recurrent PHPT and who received surgery on the basis of 18F-fluorocholine–avid lesions (65). Seven patients were cured, whereas 5 (42%) had persistent hypercalcemia. Retrospectively, the arterial-phase enhancements of the associated CT were significantly different between cured patients and not-cured patients (P = 0.007). The authors concluded that grading of the arterial phase of CT can help differentiate between true adenomas and lymph nodes (65).
IS IT TOO EARLY TO PROPOSE 18F-FLUOROCHOLINE PET/CT AS FIRST-LINE IMAGING?
Some teams reported on 18F-fluorocholine (or 11C-choline) as first-line imaging in PHPT (66–70). Four studies had greater than or equal to 50 surgery patients and a prospective design (67,68–70).
Thanseer et al. studied 54 patients (67). The detection rate was higher with 18F-fluorocholine PET/CT (imaging at 15 and 60 min) than with dual-phase 99mTc-sestamibi imaging (100% vs. 76.4%), but with more false-positive results (4 vs. 1) (67). Surgery failed in 2 patients (no lesion found), and no patient had MGD (67).
Beheshti et al. compared 18F-fluorocholine PET/CT (imaging at 60 and 110 min) and dual-phase 99mTc-sestamibi (or 99mTc-tetrofosmin) imaging in 100 patients (68). 99mTc-tetrofosmin is adequate for subtraction but not for dual-phase scanning, as it has a slow washout from the thyroid (25,26). Surgery was performed in 76 patients with intraoperative PTH monitoring. With 18F-fluorocholine, the sensitivity for parathyroid adenomas was 93.7% and the PPV was 90.2%. With 99mTc-sestamibi/99mTc-tetrofosmin, the sensitivity was 60.8% and the PPV was 94.1%. Ten patients had MGD; how many cases were recognized preoperatively was not stated (68).
Cuderman et al. (the latest report from this team) compared 18F-fluorocholine PET/CT (imaging at 5 and 60 min) and a dual-phase 99mTc-sestamibi plus 99mTc-pertechnetate scan in 188 patients (70). Surgery was offered to 103 patients. 18F-fluorocholine had a higher sensitivity (92% vs. 65%), notably in patients with small adenomas or MGD. Surgery failed in 8 patients (70).
In these studies, 18F-fluorocholine imaging had a higher sensitivity than dual-phase 99mTc-sestamibi imaging but a higher rate of false-positive results (67,68,70). Many patients did not receive surgery. Perhaps more importantly, at present there is no evidence that first-line imaging with 18F-fluorocholine PET/CT improves surgical outcomes or, notably, the rate of failed surgery.
No study compared 18F-fluorocholine PET/CT and 99mTc-sestamibi/123I subtraction imaging as first-line imaging. In the only study that compared 11C-choline PET/CT and 99mTc-sestamibi/123I subtraction imaging as first-line imaging, there was no significant difference in sensitivity (69).
The strengths of 18F-fluorocholine PET/CT imaging are shorter imaging time, lower radiation dose (Table 1), and high sensitivity. Sensitivity can be further increased with novel technologies (71), such as digital PET systems (as in Figs. 5 and 6). Potential drawbacks of 18F-fluorocholine PET/CT imaging, on the other hand, are lower availability, much higher cost, currently no listed Food and Drug Administration approval for parathyroid imaging, no thyroid tracer for comparison of risks of false-positive results from thyroid nodules, and uptake by inflammatory lymph nodes.
As stated previously, 99mTc-sestamibi has a high PPV for ectopic parathyroid lesions (9). Surgeons are very confident when embarking on thoracoscopy/thoracotomy based on 99mTc-sestamibi SPECT/CT findings. Experience with 18F-fluorocholine PET/CT imaging is still limited. Uptake of 18F-fluorocholine by inflammatory/granulomatous mediastinal lymph nodes is not rare and might reduce the ability to identify true ectopic parathyroid lesions and label them as such. Contrast-enhanced arterial-phase CT can improve the PPV of 18F-fluorocholine PET/CT (Fig. 6). However, this additional contrast-enhanced CT acquisition has logistical implications, potential side effects, and dose implications, so that it is better reserved for second-line imaging or repeat surgery cases.
LOCALIZATION PROCEDURES BEFORE REPEAT SURGERY FOR PERSISTENT OR RECURRENT HYPERPARATHYROIDISM
Hypercalcemia within 6 mo of surgery defines persistent, as opposed to recurrent, PHPT. Repeat surgery should be decided carefully, as its complication rate is higher than that for a first surgery (6,72). Concordant functional and anatomic imaging studies should be sought (7). Detailed review of surgical reports and previous imaging results is key to successful interpretation.
The algorithm in Figure 1 also applies to repeat surgery.
Sestamibi Imaging and Neck Ultrasound Before Repeat Surgery
In a prospective study, the sensitivity of dual-phase 99mTc-sestamibi SPECT/CT was 19%, whereas the sensitivity of 99mTc-sestamibi/123I scintigraphy (planar only) was 59% (P < 0.01) (73). Sensitivity can be further improved with pinhole imaging (74), and complementary SPECT/CT is necessary given the high prevalence of ectopic glands (27). In MEN1, the possibility of more than 1 site of recurrence should be considered, as with renal hyperparathyroidism (75).
Repeat neck ultrasound should be performed by an experienced operator. Ultrasound-guided fine-needle aspiration for PTH washout can be considered in difficult cases (7,72).
18F-Fluorocholine PET/CT and 4D CT Before Repeat Surgery
In a retrospective analysis of patients with prior neck surgery and negative/inconclusive first-line imaging results (76), the sensitivity of 18F-fluorocholine PET/CT was 96% and the PPV was 77%. With 4D CT, the sensitivity was 75% and the PPV was 80%. The surgical success rate was 73%. Thus, although both techniques have a high sensitivity, the risk of false-positive findings is also high. Combining the 2 studies or adding arterial-phase CT acquisition to conventional 18F-fluorocholine PET/CT to improve the PPV in this challenging population is desirable (65).
11C-Methionine PET/CT Before Repeat Surgery
11C-methionine PET/CT was positive in 6 of 15 patients (40%) with prior negative dual-phase 99mTc-sestamibi imaging results (77).
Selective Venous Sampling for PTH Before Repeat Surgery
Selective venous sampling for PTH before repeat surgery should be considered only when imaging studies are unhelpful (7,72). It is highly reliant on the technique used and the operator’s expertise, with variable results (73,78). The yield when first-line and second-line imaging results, including 18F-fluorocholine PET/CT results, are inconclusive (algorithm in Fig. 1) is currently unknown and deserves investigation before conclusions regarding the role of this invasive technique can be drawn.
CONCLUSION
Preoperative imaging in PHPT can identify ectopic parathyroid glands and is always required. A 99mTc-sestamibi/123I subtraction scanning provides better sensitivity for MGD than a dual-phase 99mTc-sestamibi scan. This approach should be helpful in improving outcomes with targeted parathyroid surgery, reducing the rates of surgical conversions as well as failures. When scintigraphy and neck ultrasound results are negative, 18F-fluorocholine PET/CT or 4D CT still offers high detection rates. The risk of false-positive findings should be kept in mind, however, and strategies to reduce this risk should be encouraged.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: How can radionuclide imaging best guide surgery in patients with PHPT?
PERTINENT FINDINGS: 99mTc-sestamibi/123I subtraction scanning provides better sensitivity than dual-phase 99mTc-sestamibi scanning. When scintigraphy and neck ultrasound are negative/inconclusive, 18F-fluorocholine PET/CT imaging is indicated. Adding a contrast-enhanced arterial CT phase can reduce the risk of false-positive result from reactive lymph nodes.
IMPLICATIONS FOR PATIENT CARE: These optimized radionuclide imaging techniques should be helpful in improving outcomes, allowing precision parathyroid surgery.
ACKNOWLEDGMENT
In accordance with French Jardé Law, the review board of University Hospitals of Bordeaux waives the requirement for informed consent for review articles and retrospective use of anonymized data obtained in the course of routine clinical care.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- Received for publication August 14, 2020.
- Accepted for publication October 21, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Visual Abstract
- Abstract
- IMAGING IS RECOMMENDED BEFORE FIRST PARATHYROID SURGERY IRRESPECTIVE OF SURGICAL APPROACH
- ADVANTAGES AND DISADVANTAGES OF TARGETED SURGERY: IMPLICATIONS REGARDING CHOICE OF IMAGING
- WHY IS 99mTc-SESTAMIBI/123I SUBTRACTION IMAGING BETTER OPTION THAN DUAL-PHASE SESTAMIBI SCANNING FOR GUIDING TARGETED SURGERY?
- SECOND-LINE IMAGING STRATEGY WHEN SCINTIGRAPHY AND NECK ULTRASOUND RESULTS ARE NEGATIVE, DISCORDANT, OR INCONCLUSIVE
- IS IT TOO EARLY TO PROPOSE 18F-FLUOROCHOLINE PET/CT AS FIRST-LINE IMAGING?
- LOCALIZATION PROCEDURES BEFORE REPEAT SURGERY FOR PERSISTENT OR RECURRENT HYPERPARATHYROIDISM
- CONCLUSION
- DISCLOSURE
- ACKNOWLEDGMENT
- REFERENCES
- Figures & Data
- Info & Metrics