


Visual Abstract
Abstract
Our objective was to evaluate the impact of 18F-FDG PET CT on the management of urachal adenocarcinoma (UrC-ADC). Methods: A retrospective analysis of patients with UrC-ADC from 2001 to 2019 at Memorial Sloan Kettering was performed. Mayo stage before 18F-FDG PET/CT, rate of detection of the primary malignancy and metastases on 18F-FDG PET/CT, Mayo stage after 18F-FDG PET/CT, and change in patient management were determined. Results: Of 21 patients with UrC-ADC before 18F-FDG PET/CT, Mayo staging was I/II in 8, III in 3, and IV in 10. 18F-FDG PET/CT detected previously unidentified metastases in 8 (38%) of 21 patients, resulting in upstaging of disease in 3 (14%) patients and a change in treatment in 4 (19%) patients. Conclusion: 18F-FDG PET/CT has clinical utility in patients with UrC-ADC by identifying metastatic disease not appreciated on anatomic imaging, leading to changes in staging and patient management.
Urachal adenocarcinoma (UrC-ADC) is an aggressive nonurothelial tumor of the urachus, a remnant of the embryologic structure connecting the allantois and fetal bladder (1–4). Metastatic disease exists on presentation in 20%–50% of UrC-ADC patients (5–7). The stage of UrC-ADC is the most important prognostic factor, with 5-y survival rates of 63%, 55%, 19%, and 8% for stages I, II, III, and IV, respectively (2,6). Accurate and effective staging is therefore critical in assessing UrC-ADC and guiding treatment (3,5,8,9).
Although 18F-FDG PET/CT has demonstrated value in many malignancies (10–12), UrC-ADC is often mucinous in histology (1–4), and mucinous malignancies may demonstrate low or absent 18F-FDG uptake (13). Thus, 18F-FDG PET/CT may not be sensitive for UrC-ADC. Data for 18F-FDG PET/CT in UrC-ADC are limited to brief reports and pictorial essays (14–17). The objective of this study was to determine whether 18F-FDG PET/CT impacts systemic staging of UrC-ADC and its clinical management.
MATERIALS AND METHODS
Study Design
This Health Insurance Portability and Accountability Act–compliant, retrospective, single-institution study was performed under Institutional Review Board approval, with the requirement to obtain informed consent being waived by the board. Our hospital information system was screened for patients with pathologically proven cases of UrC-ADC diagnosed between January 2001 and January 2019 who underwent imaging with contrast-enhanced CT or MRI and 18F-FDG PET/CT within 6 wk of each other before systemic or radiation therapy. Patients with the following characteristics were excluded: incomplete clinical or histopathologic records, prior malignancy, nonadenocarcinoma histology of UrC, no 18F-FDG PET/CT imaging, no conventional CT or MRI within 6 wk before the 18F-FDG PET/CT, or administration of chemotherapy or radiation therapy before 18F-FDG PET/CT. For patients included in our analysis, medical records were reviewed to determine age, sex, and pathologic subtype (mucinous or nonmucinous) of the tumor.
Determination of Stage Before 18F-FDG PET/CT
The Mayo staging system for UrC (Table 1) was used to classify the urachal tumors (5). Contrast-enhanced CT (or MRI for 1 patient) was used to determine an imaging stage before 18F-FDG PET/CT.
Mayo Classification Staging System for Urachal Cancer
18F-FDG PET/CT Imaging and Interpretation
18F-FDG PET/CT and contrast-enhanced cross-sectional imaging studies were evaluated by a nuclear radiologist who was dually board-certified in nuclear medicine and diagnostic radiology, had 15 y of PET/CT experience, and was masked to the pre-PET/CT stage. A nuclear medicine fellow assisted. SUVs, normalized to body weight, were determined on the GE Healthcare AW suite. According to standard 18F-FDG PET/CT reporting, uptake was considered abnormal when it was focal, was not physiologic or inflammatory, and had an intensity greater than the local background.
Determination of Stage After 18F-FDG PET/CT and Rate of Upstaging
Metastases identified by 18F-FDG PET/CT that had not been detected in prior conventional cross-sectional imaging studies were recorded. 18F-FDG PET/CT results were used to determine disease stage after 18F-FDG PET/CT. The initial clinical stage was compared with the clinical stage after 18F-FDG PET/CT to determine the rate of upstaging. Changes in patient management based on 18F-FDG PET/CT were recorded as determined from medical records. The 18F-FDG PET/CT scan results were confirmed with the histologic data when available. When the histology was not available, imaging follow-up was used.
Characterization of Primary Malignancies
CT or MR images were reviewed to classify the primary UrC-ADC as well defined or ill defined, solid or cystic, enhancing or nonenhancing, and with or without calcifications. On 18F-FDG PET/CT, the primary UrC-ADC was classified as 18F-FDG–avid (above the local background), and if avid, the SUVmax was recorded.
RESULTS
Patient Demographics
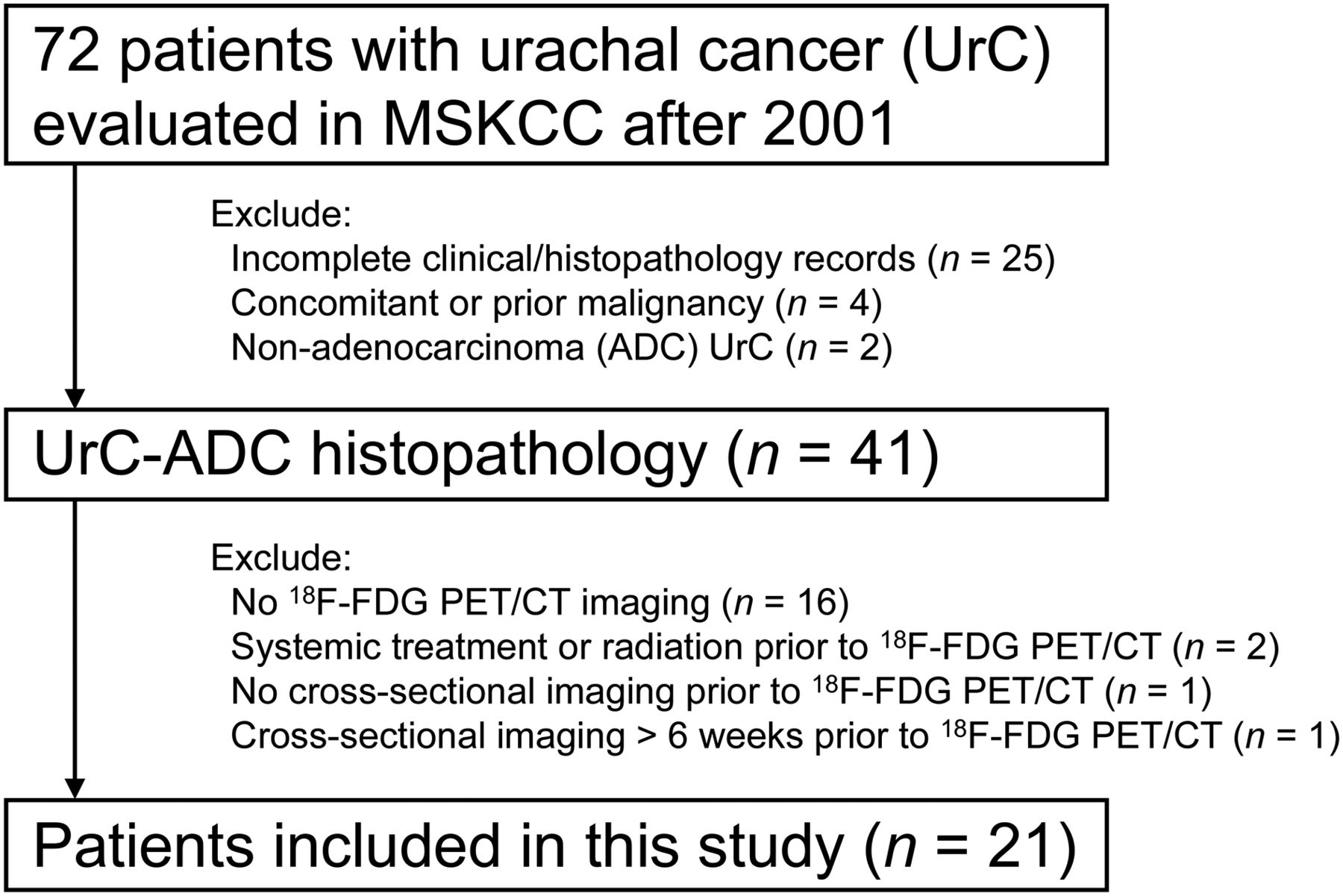
A Standards for Reporting of Diagnostic Accuracy Studies (STARD) diagram of patients screened and included in our analysis is presented in Figure 1. The demographics of the 21 patients included in the cohort are outlined in Table 2.

STARD diagram for patients screened and included in our analysis.
Demographics for Our Cohort of 21 Patients with UrC-ADC
Mayo Stage Before 18F-FDG PET/CT
Before 18F-FDG PET/CT, Mayo staging was I/II in 8 (38%), III in 3 (14%), and IV in 10 (48%) patients. All metastatic disease detected on conventional cross-sectional imaging was histopathologically proven from at least 1 site. The most common sites of distant metastases were the peritoneum (n = 6), lung (n = 4), distant nodes (n = 2), liver (n = 2), pancreas (n = 1), and soft tissue (n = 1). Five patients had more than 1 site of metastatic disease.
Additional Metastases Detected by 18F-FDG PET/CT
Twenty-one patients underwent 18F-FDG PET/CT within 6 wk of conventional imaging (Table 3) and before systemic or radiation therapy. In 11 patients, 18F-FDG PET/CT was performed before resection of the primary malignancy, whereas in 10 patients, it was performed afterward. The median number of days from prior cross-sectional imaging to 18F-FDG PET/CT was 17.3 (range, 0–42).
Results for 21 Patients with UrC-ADC Undergoing 18F-FDG PET/CT After Conventional CT or MR
Previously undetected metastases were identified on 18F-FDG PET/CT in 8 of 21 patients (38%). These included osseous metastases in 4 patients, nodal metastases in 3 patients (pelvic, n = 2; thoracic, n = 1), pancreatic metastases in 2 patients, and hepatic metastases in 1 patient. Two patients had more than 1 site of newly detected metastatic disease: osseous and nodal in one, and osseous and pancreatic in the other. The SUVmax of 18F-FDG–avid metastases ranged from 3.0 to 14.5. Histopathologic confirmation was obtained in 3 patients (pelvic nodal and pancreatic in 1 patient, liver in 1 patient, and pancreatic in 1 patient), whereas in 5 patients newly detected metastases demonstrated an increase in size or 18F-FDG avidity on subsequent imaging studies. Three patients (14%) were upstaged by 18F-FDG PET/CT: two from Mayo stage II to IV and the third from Mayo stage III to IV.
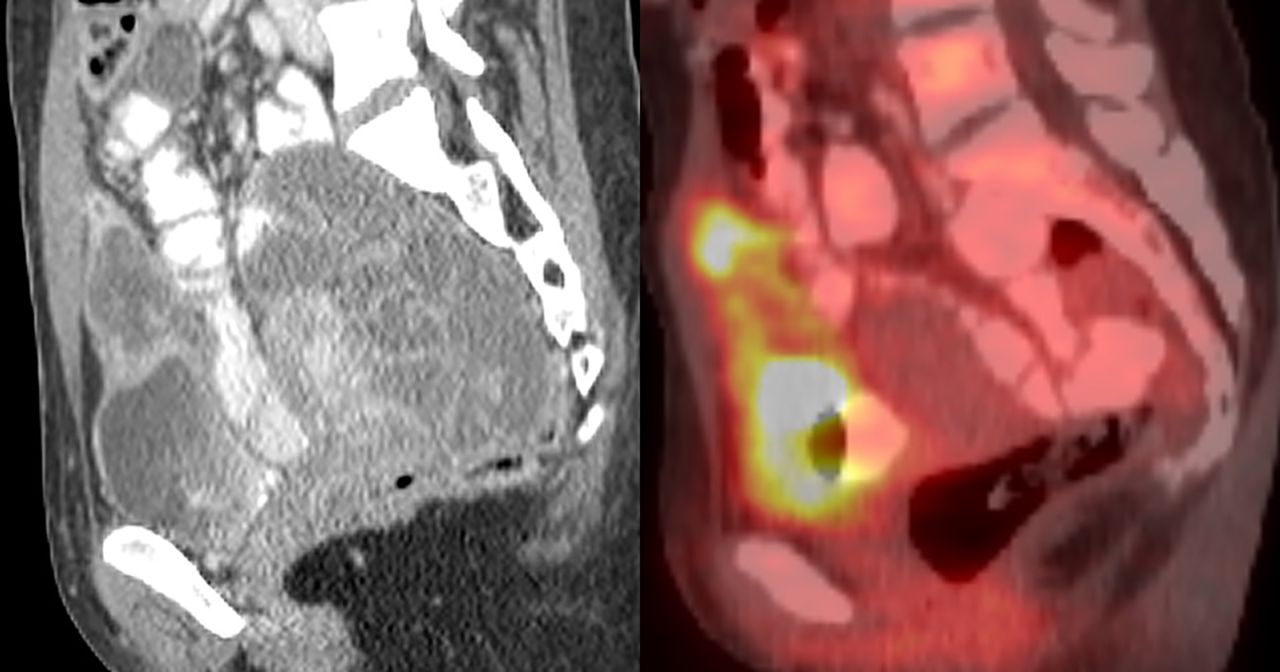
On the basis of the 18F-FDG PET/CT findings, treatment was changed or escalated in 4 of 21 patients (19%). An 18F-FDG–avid pancreatic metastasis that was detected in 1 patient (previously considered a candidate for potentially curative surgical resection of the primary UrC-ADC) resulted in systemic treatment with chemotherapy instead of surgery. An 18F-FDG–avid liver metastasis was detected in 1 patient (Fig. 2), resulting in initiation of systemic chemotherapy. In a third patient, 18F-FDG–avid pancreatic and osseous metastases led to treatment escalation with chemotherapy and radiation to osseous metastases (Fig. 3). A fourth patient (considered Mayo stage IV by CT and thus not upstaged by 18F-FDG PET/CT) being treated with chemotherapy alone was subsequently treated with radiation after detection of additional osseous metastases on 18F-FDG PET/CT.

A 50-y-old man with UrC-ADC. Axial 18F-FDG PET/CT (A) demonstrates hepatic lesion (arrow) with SUVmax of 9.0, which was occult on prior contrast-enhanced CT (B). Lesion was subsequently biopsied under ultrasound guidance and proven to be metastasis.

A 47-y-old man with UrC-ADC. Axial PET/CT (A) demonstrates 18F-FDG–avid pancreatic lesion (arrow) with SUVmax of 14.2, as well as additional osseous metastasis lesion (arrowhead) not detected on prior contrast-enhanced CT of abdomen and pelvis (B). Pancreatic lesion was subsequently sampled by endoscopic ultrasound using fine-needle aspiration and proven to be metastasis.
Characteristics of Primary Urc-ADC Tumors on Contrast-Enhanced CT and 18F-FDG PET/CT
The primary UrC-ADC tumor was imaged with contrast-enhanced CT in 17 patients at the time of their initial clinical presentation. The mean size of the primary tumor in the longest-axis dimension was 4.8 cm (range, 2.2–13.7 cm). Most tumors had well-defined margins (82%), were predominantly cystic or mixed solid–cystic (76%), and demonstrated enhancement (88%). Thirteen (76%) of the primary UrC-ADC tumors contained calcifications.
Six patients had their primary tumor resected before undergoing the contrast-enhanced cross-sectional CT or MRI study that was performed within 6 wk before the 18F-FDG PET/CT imaging study. That left 11 primary urachal tumors imaged on PET/CT. Seven of the 11 (63.6%) primary UrC-ADCs evaluable on PET/CT were 18F-FDG–avid, with a mean SUVmax of 13.8 (range, 4.0–27.5), and 4 of the 11 (46%) demonstrated background 18F-FDG uptake. Additional imaging features of primary UrC-ADC on contrast-enhanced CT and 18F-FDG PET/CT are summarized in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org).
Mucinous Tumors Versus Nonmucinous Tumors and 18F-FDG Avidity
Fourteen UrC-ADCs were mucinous on histopathology. Of these, 10 (71%) had metastatic disease. Seven of the 10 (70%) with metastatic disease demonstrated 18F-FDG–avid metastases. Of the 7 with 18F-FDG–avid metastases, 4 had an evaluable primary tumor, and 3 of the 4 primary tumors were 18F-FDG–avid (SUVmax, 4, 1.7, and 24.6).
Seven UrC-ADCs were nonmucinous tumors. Of these, 5 (71%) had metastatic disease. All 5 with metastatic disease (100%) demonstrated 18F-FDG–avid metastases. Of the 5 with 18F-FDG–avid metastases, 3 had an evaluable primary tumor, and all 3 of the primary tumors were 18F-FDG–avid (SUVmax, 9, 19.5, and 27).
DISCUSSION
We evaluated the clinical utility of 18F-FDG PET/CT in staging of UrC-ADC. 18F-FDG PET/CT detected additional metastases in nearly 40% of patients and upstaged disease by radiographic criteria in almost 15%, compared with cross-sectional imaging performed within 6 wk beforehand. In addition, 18F-FDG PET/CT resulted in a change in management or treatment plan in almost 20% of patients.
Because of the rarity of this tumor, the literature pertaining to 18F-FDG PET/CT evaluation of urachal pathology consists primarily of case reports and smaller case series. The positive predictive value of imaging to detect malignancy preoperatively is low when dealing with a urachal mass (18), as both benign and malignant urachal pathology can appear similar on contrast-enhanced CT and 18F-FDG PET/CT (19,20). Variable 18F-FDG avidity of UrC-ADC has been described in the literature (21,22). Guimarães et al. described a primary UrC-ADC demonstrating increased 18F-FDG uptake (without distant metastases), for which 18F-FDG PET/CT provided valuable information for diagnosis and initial staging (22). Zeman et al. described a false-negative 18F-FDG PET/CT finding in a mucinous UrC-ADC showing background 18F-FDG uptake without evidence of metastatic disease (23). Interestingly, Li et al. described 18F-FDG PET/CT findings in a patient with a primary mucinous UrC-ADC showing low-level 18F-FDG avidity (SUV, 2.4), with 18F-FDG–avid nodal and osseous metastases (SUV, 6.9) (21). We noted a similar finding in our series of patients. Of the 4 patients with 18F-FDG–avid metastases and an evaluable mucinous primary UrC-ADC, the primary tumor was nonavid in 1 case.
Mucinous tumors have been shown to demonstrate low or background 18F-FDG uptake due to hypocellularity, potentially limiting the sensitivity of 18F-FDG PET/CT (13,24). The mucinous tumor subtype comprised the majority (67%) of our patients with UrC-ADC. Half of these patients (7/14) developed 18F-FDG–avid metastatic disease.
We are limited by both the small sample size and the retrospective nature of the study. In addition, the absence of data or guidelines for the use of 18F-FDG PET/CT in UrC-ADC may have introduced selection bias in our single-center analysis. However, because of the rarity of UrC-ADC, high-powered prospective studies would be difficult to undertake.
CONCLUSION
Our data suggest that 18F-FDG PET/CT has clinical utility in patients with UrC-ADC by identifying metastatic disease not appreciated on anatomic imaging, leading to changes in staging and patient management.
DISCLOSURE
Funding was received from an NIH/NCI Cancer Center support grant (P30 CA008748). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Does 18F-FDG PET/CT impact the staging and management of UrC-ADC?
PERTINENT FINDINGS: This retrospective analysis of 21 patients with UrC-ADC before chemotherapy or radiation therapy demonstrated that 18F-FDG PET/CT within 6 wk of conventional CT or MRI detected previously unidentified metastases in 8 (38%) patients, resulted in upstaging of disease in 3 (14%) patients and a change in treatment management in 4 (19%) patients.
IMPLICATIONS FOR PATIENT CARE: 18F-FDG PET/CT has clinical utility in patients with UrC-ADC by identifying metastatic disease not appreciated on anatomic imaging, leading to changes in staging and patient management.
Footnotes
Published online Sep. 18, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 15, 2020.
- Accepted for publication August 11, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.