


Visual Abstract

Abstract
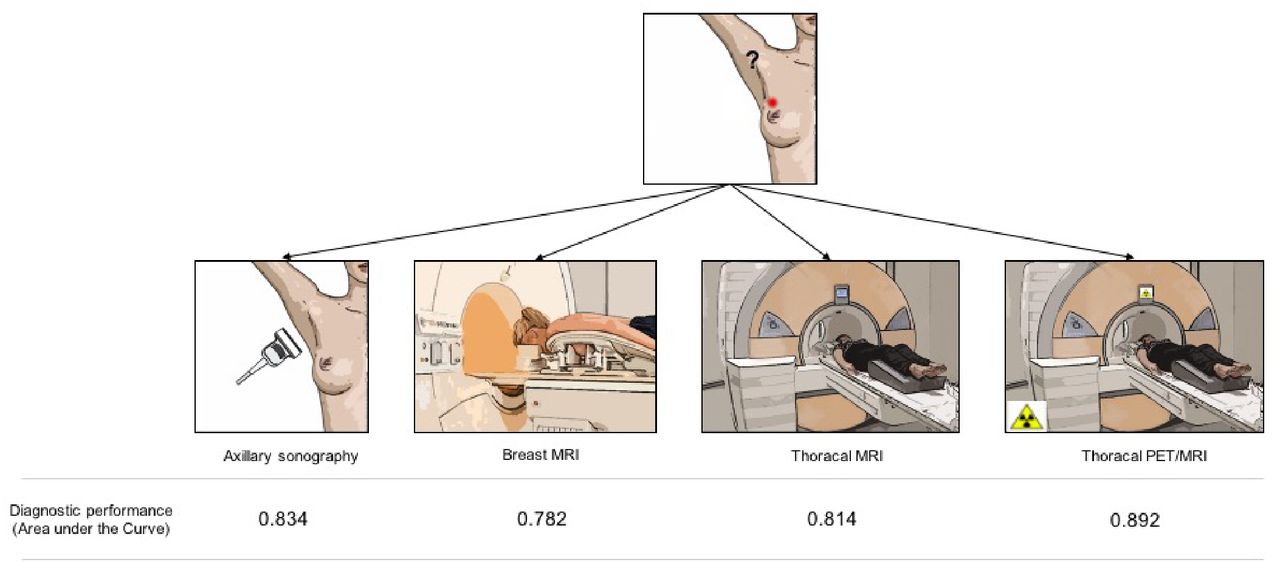
The purpose of this study was to compare breast MRI, thoracic MRI, thoracic 18F-FDG PET/MRI, and axillary sonography for the detection of axillary lymph node metastases in women with newly diagnosed breast cancer. Methods: This prospective double-center study included patients with newly diagnosed breast cancer between March 2018 and December 2019. Patients underwent thoracic (18F-FDG PET/)MRI, axillary sonography, and dedicated prone breast MRI. Datasets were evaluated separately regarding nodal status (nodal-positive vs. nodal-negative). Histopathology served as the reference standard in all patients. The diagnostic performance of breast MRI, thoracic MRI, thoracic PET/MRI, and axillary sonography in detecting nodal-positive patients was tested by creating receiver-operating-characteristic curves (ROC) with a calculated area under the curve (AUC). Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were calculated for all 4 modalities. A McNemar test was used to assess differences. Results: In total, 112 female patients (mean age, 53.04 ± 12.6 y) were evaluated. Thoracic PET/MRI showed the highest AUC, with a value of 0.892. The AUCs for breast MRI, thoracic MRI, and sonography were 0.782, 0.814, and 0.834, respectively. Differences between thoracic PET/MRI and axillary sonography, thoracic MRI, and breast MRI were statistically significant (PET/MRI vs. axillary sonography, P = 0.01; PET/MRI vs. thoracic MRI, P = 0.02; PET/MRI vs. breast MRI, P = 0.03). PET/MRI showed the highest sensitivity (81.8% [36/44]; 95% CI, 67.29%–91.81%), whereas axillary sonography had the highest specificity (98.5% [65/66]; 95% CI, 91.84%–99.96%). Conclusion: 18F-FDG PET/MRI outperforms axillary sonography, breast MRI, and thoracic MRI in determining the axillary lymph node status. In a clinical setting, the combination of 18F-FDG PET/MRI and axillary sonography might be considered to provide even greater accuracy in diagnosis.
Breast cancer is the most common cancer in women worldwide, representing about 25% of all cancers in women (1). Initial treatment strategies and patients’ prognosis are fundamentally based on tumor biology and tumor stage. Typically, the axillary lymph nodes are the first site of nodal metastatic disease in invasive breast cancer (2). The ability to distinguish between nodal-positive and nodal-negative status in both pre- and posttherapeutic situations is crucial to provide an appropriate and individualized therapeutic concept for the axilla and to determine prognosis (3). So far, sentinel lymph node biopsy or sentinel lymph node excision has been regarded as the gold standard for axillary staging in early breast cancer (4), but different surgical axillary procedures such as targeted lymph node excision or targeted axillary dissection have been proposed as favorable alternatives to deescalate invasive procedures such as axillary dissection (5). However, these invasive procedures can cause morbidity such as infection or hematoma, as well as causing patient discomfort. At the time of initial diagnosis, about 25%–40% of early breast cancer stages show axillary nodal metastatic disease (6,7), which means that for about 60%–75% of the patients with early-stage breast cancer any kind of axillary intervention represents overtreatment. Therefore, a noninvasive imaging method for discriminating between nodal-positive and nodal-negative axillary status is desirable to avoid unnecessary biopsies before therapy and to facilitate therapy planning.
Different imaging modalities are available for the initial staging of breast cancer patients. Over the last few years, breast MRI, axillary sonography, and CT have become well established in this regard (8,9). However, no imaging modality has yet proven accurate enough to replace invasive procedures for determining the correct nodal status (10,11). While 18F-FDG PET imaging can reliably display increased glycolytic activity in metastatic tissue, MRI offers images with high anatomic resolution and high soft-tissue contrast. Hence, hybrid 18F-FDG PET/MRI might serve as an excellent combined imaging modality for locoregional staging compared with conventional imaging such as ultrasound, breast MRI, or CT (12).
The aim of our study was to compare thoracic 18F-FDG PET/MRI, breast MRI, thoracic MRI, and axillary sonography with regard to their ability to determine the correct axillary nodal status in patients with primary breast cancer, using histopathology as the reference standard.
MATERIALS AND METHODS
Patients
The local ethics committees approved this prospective, double-center study (studies 17-7396-BO and 6040R). All patients gave written informed consent before enrolment. Patients who had newly diagnosed, therapy-naive breast cancer with an elevated risk for distant metastases between March 2018 and December 2019 were included in this study if they fulfilled the following criteria: a newly diagnosed, treatment-naïve T2 or higher tumor; a newly diagnosed, treatment-naïve triple-negative tumor of any size; or a newly diagnosed, treatment-naïve tumor with molecular high risk (Ki-67 > 14% or G3 or her2 overexpression). Breast feeding, pregnancy, malignancies in the last 5 y, or contraindications to MRI or MRI contrast agents were exclusion criteria. Of the 112 patients, 45 had been reported previously (13). In contrast to the prior publication, we investigated further imaging modalities such as breast MRI and sonography for axillary nodal staging instead of the comparison of MRI, PET/MRI, and bone scintigraphy for N and M staging.
PET/MRI and Breast MRI
All 18F-FDG PET/MRI examinations were performed from head to mid thigh on an integrated 3.0-T PET/MRI scanner (Biograph mMR; Siemens Healthcare GmbH) with the patient supine, about 60 min after intravenous injection of a body weight–adapted dose of 18F-FDG (4 MBq/kg of body weight). Patients fasted for 6 h before the examination, and blood glucose levels were ensured to be below 150 mg/dL before 18F-FDG was injected.
Just before the whole-body imaging was performed, each patient underwent dedicated breast MRI in the head-first prone position on the same integrated 3.0-T PET/MRI scanner. The imaging protocol has been detailed by Kirchner et al. (14). Thoracic whole-body PET/MRI and MRI sections were evaluated for axillary nodal status and are referred to here as 18F-FDG thoracic PET/MRI and thoracic MRI.
PET/MR and MR Image Analysis
Images were analyzed independently and in random order by 2 experienced radiologists with extensive experience in hybrid imaging, as well as by a nuclear medicine specialist, using an OsiriX Workstation (Pixmeo SARL) with a reading intermission of 4 wk to avoid recognition bias. Discordant readings were resolved in a collective consensus reading. For every patient and modality, the axillary lymph node status was rated as either nodal-positive or nodal-negative. Morphologic features for the diagnosis of lymph node metastases on MRI were short-axis diameter greater than 10 mm, irregular margin, inhomogeneous cortex, perifocal edema, absence of fatty hilum, asymmetry in comparison to the contralateral site, contrast medium enhancement, and blurred nodal border (15). In PET/MRI, tracer uptake above the level of the direct background and the surrounding lymph nodes was considered a sign of malignancy. To measure SUVmax and SUVmean, a manually drawn region of interest was placed around the respective lymph node. Readers were masked to patient identity, history, and the results of local and distant metastasis but aware of the diagnosis of breast cancer.
Axillary Sonography
Axillary sonography was performed at each center by a gynecologist with multiple years of experience in breast and axillary ultrasound. No regular second assessment was done by a second reader. An Acuson S2000 system (Siemens Healthcare GmbH), a SuperSonic Imagine Aixplorer (Toshiba Medical Systems GmbH), and an Aplio MX SSA-780A system (Toshiba Medical Systems GmbH), each with a linear array transducer of 5–12 MHz, were used. Lymph nodes were regarded as suggestive, mostly with an indication for biopsy, when the cortical thickness was greater than 3 mm, the cortex was lobulated, or the hilum was decreased or absent (16,17).
Reference Standard
Histopathology served as the reference standard in every patient and was used to evaluate the nodal status (nodal-positive vs. nodal-negative). If available, tissue samples from axillary dissection or sentinel lymph node biopsy before systemic therapy were used as the reference standard. If no sufficient pretherapeutic sampling was available, sentinel lymph node excision or axillary dissection after neoadjuvant systemic therapy was used as a surrogate reference standard. In the case of insufficient pretherapeutic sampling, additional histologic preparations were evaluated, using focal fibrosis or focal necrosis as an indirect indication for previously vital lymph node metastases (18,19).
Statistics
Statistical analysis was performed using SPSS Statistics, version 26 (IBM Corp.). A P value of less than 0.05 was considered statistically significant. Data are presented as mean ± SD. The diagnostic performance of breast MRI, thoracic MRI, thoracic PET/MRI, and axillary sonography in detecting nodal-positive patients was tested by creating receiver operating-characteristic (ROC) curves with a calculated area under the curve (AUC). A McNemar test was used to assess AUC differences between thoracic PET/MRI and axillary sonography, thoracic MRI, and breast MRI and between axillary sonography and thoracic MRI, respectively. In addition, sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were calculated for breast MRI, thoracic MRI, thoracic PET/MRI, and axillary sonography. Sensitivity was defined as true-positive/(true-positive + false-negative). Specificity was defined as true-negative/(true-negative + false-positive). Positive predictive value was defined as true-positive/(true-positive + false-positive). Negative predictive value was defined as true-negative/(true-negative + false-negative). Accuracy was defined as (true-negative + true-positive)/(true-negative + true-positive + false-negative + false-positive) (20). To compare SUVmax between false-positive and correctly positive lymph nodes on thoracic PET/MRI, a Student t test was used.
RESULTS
Patient Population and Reference Standard
In total, 112 women (mean age, 53.04 ± 12.6 y) were prospectively included in this study (Fig. 1). Patient demographics and primary tumor characteristics are presented in Table 1. In every patient, breast MRI, thoracic MRI, and PET/MRI were available. Axillary sonography was available in 108 patients. In all patients, 18F-FDG was used as the tracer (mean activity, 247.7 ± 53.52 MBq).
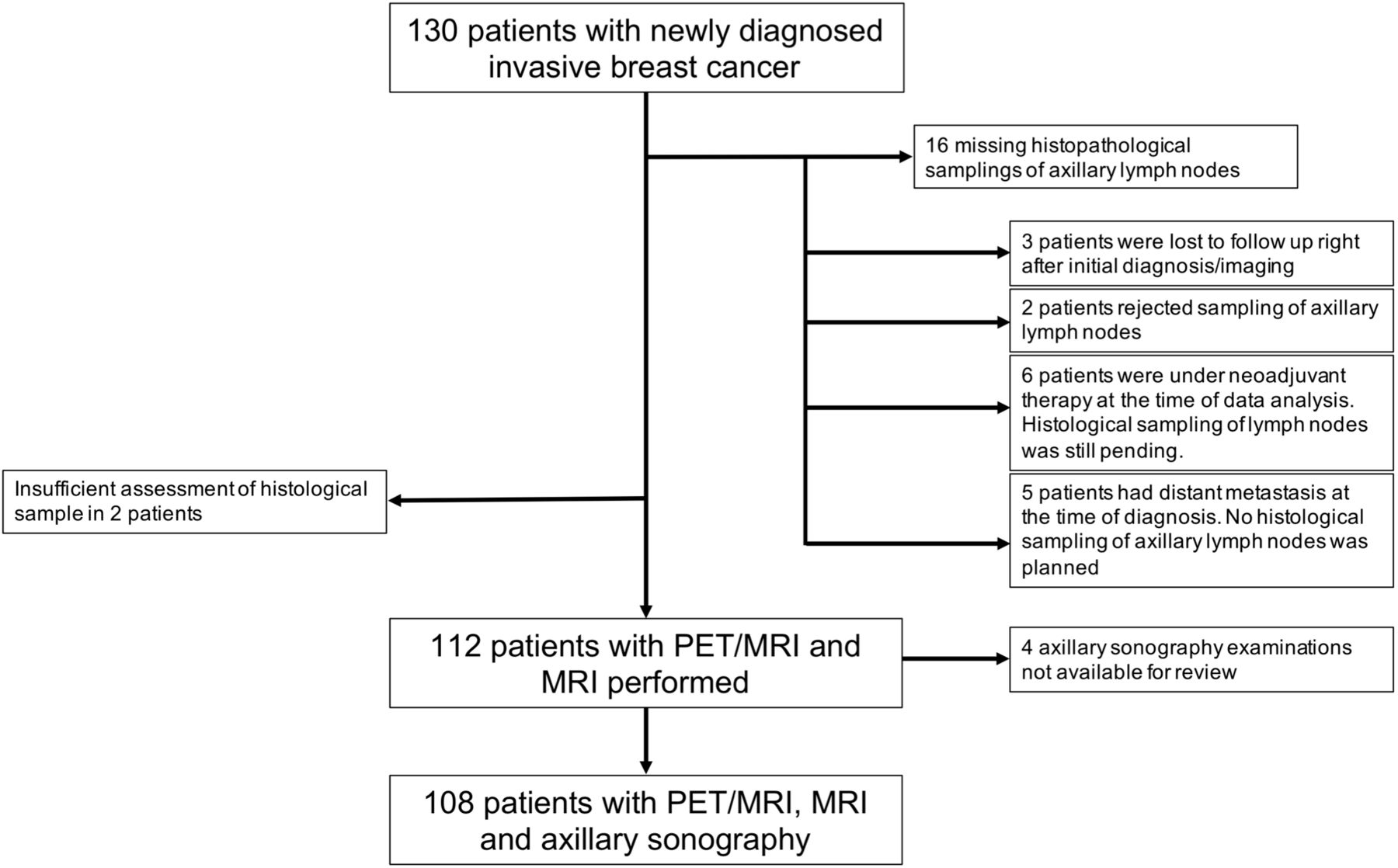
STARD diagram showing initial number of patients and reasons for exclusion.
Patient Demographics and Primary Tumor Characteristics
On the basis of the reference standard, 44 patients (39%) were nodal-positive, whereas 68 (61%) patients were nodal-negative. In 57 of 112 patients, histologic samples were taken before systemic therapy (31 axillary core-needle biopsies, 20 sentinel lymph node excisions, and 6 axillary dissections), whereas 55 samples were taken right after neoadjuvant systemic therapy (50 sentinel lymph node excisions and 5 axillary dissections).
Diagnostic Performance
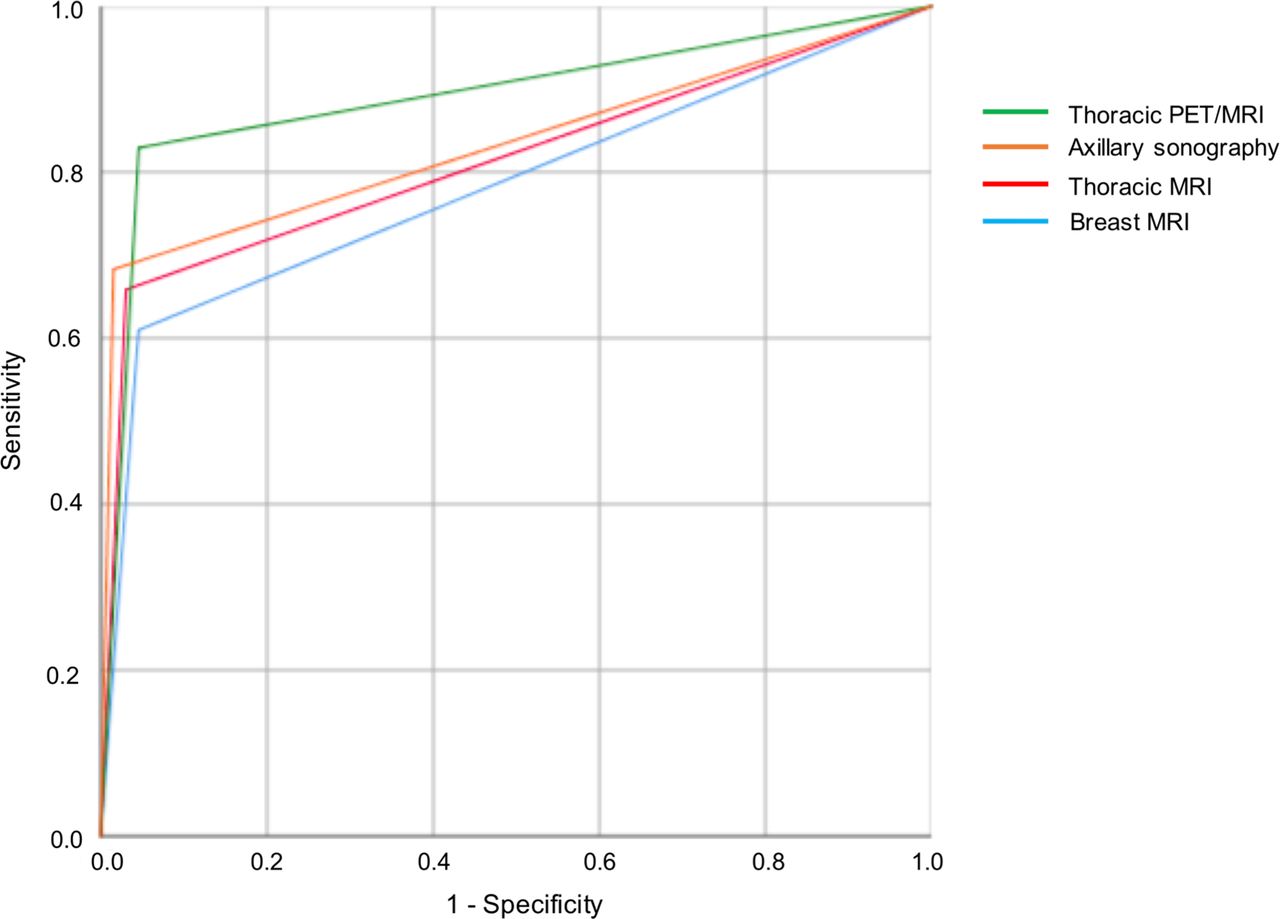
Of the imaging modalities tested, thoracic PET/MRI showed the highest AUC, with a value of 0.892 (95% CI, 0.801–0.953) (Fig. 2; Table 2). The AUCs for breast MRI, thoracic MRI, and axillary sonography were 0.782 (95% CI, 0.674–0.871), 0.814 (95% CI, 0.718–0.904), and 0.834 (95% CI, 0.740–0.920), respectively.
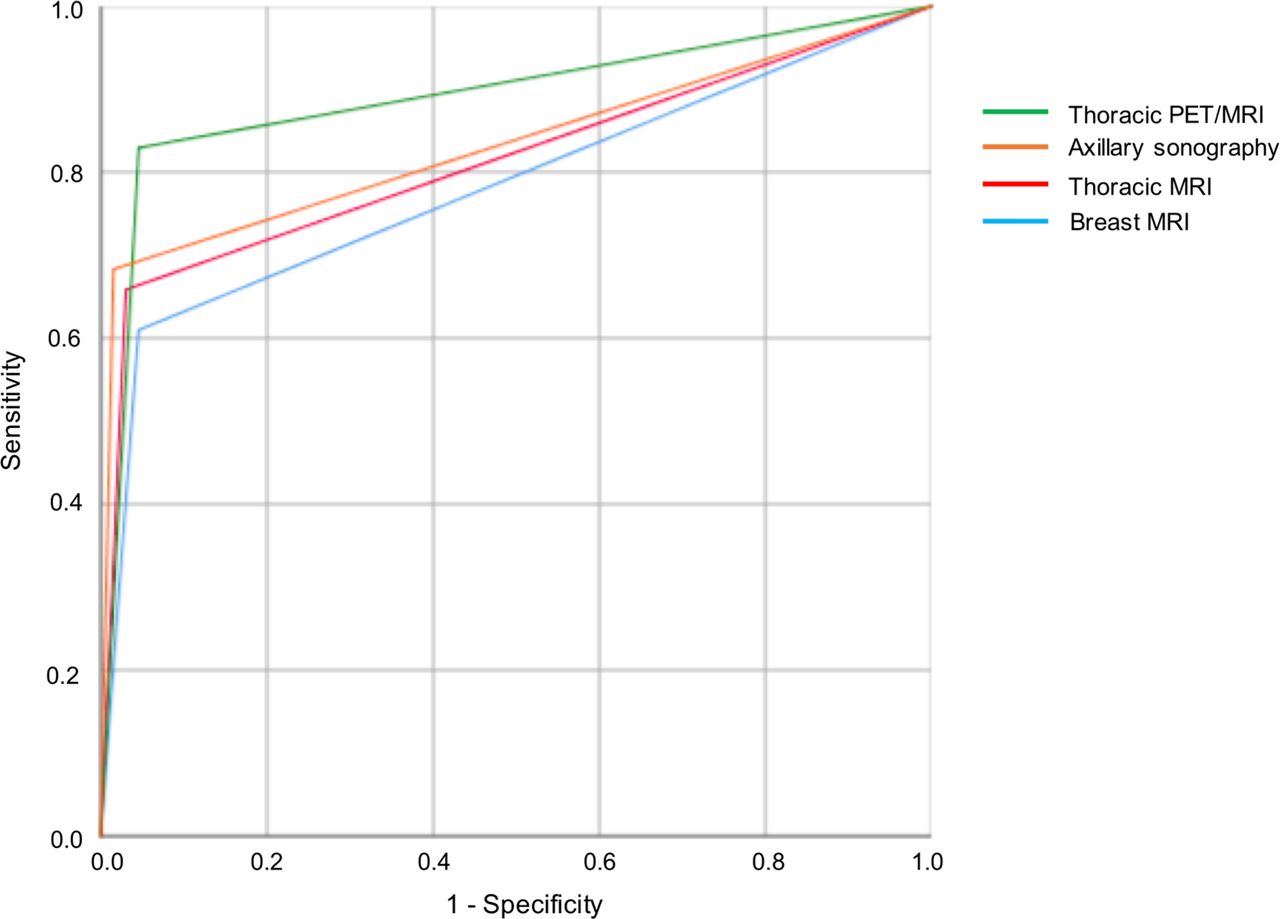
Receiver-operating-characteristic curves for diagnostic performance, comparing axillary lymph node positivity among thoracic PET/MRI, axillary sonography, thoracic MRI, and breast MRI.
AUC for the 4 Modalities
We found that PET/MRI had the highest sensitivity of the 4 imaging modalities (81.8% [36/44]; 95% CI, 67.29%–91.81%), whereas breast MRI had the lowest sensitivity (61.4% [27/44]; 95% CI, 45.50%–75.64%). On the other hand, axillary sonography had the highest specificity (98.5% [65/66]; 95% CI, 91.84%–99.96%), whereas breast MRI and thoracic PET/MRI had the lowest specificity (each 95.6% [65/68]; 95% CI, 87.64%–99.08%). At 96.7% (29/30; 95% CI, 80.39%–99.51%), axillary sonography had the best positive predictive value, whereas breast MRI showed the weakest positive predictive value (90.0% [27/30]; 95% CI, 74.37%–96.54%). Thoracic PET/MRI offered the best negative predictive value, at 89.0% (65/73; 95% CI, 81.25%– 93.84%). In contrast, breast MRI offered the weakest negative predictive value (79.3% [65/82]; 95% CI, 72.42%– 84.77%). Overall, thoracic PET/MRI showed the best diagnostic accuracy (90.18% [101/112]; 95% CI, 83.11%– 94.99%) (Tables 3 and 4; Figs. 3 and 4). Differences between PET/MRI and axillary sonography (P = 0.01), thoracic MRI (P = 0.02), and breast MRI (P = 0.03) were statistically significant, whereas differences between axillary sonography and thoracic MRI were not (P = 0.68).
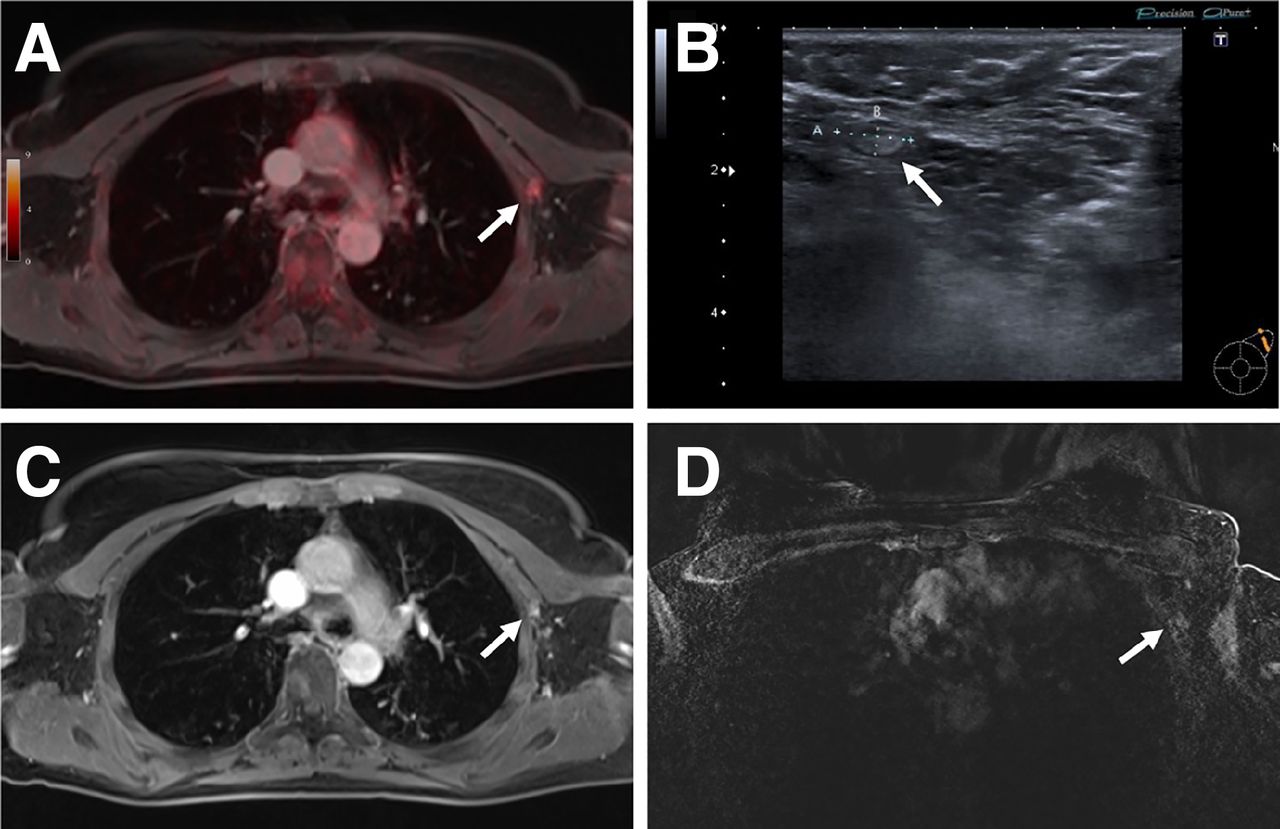
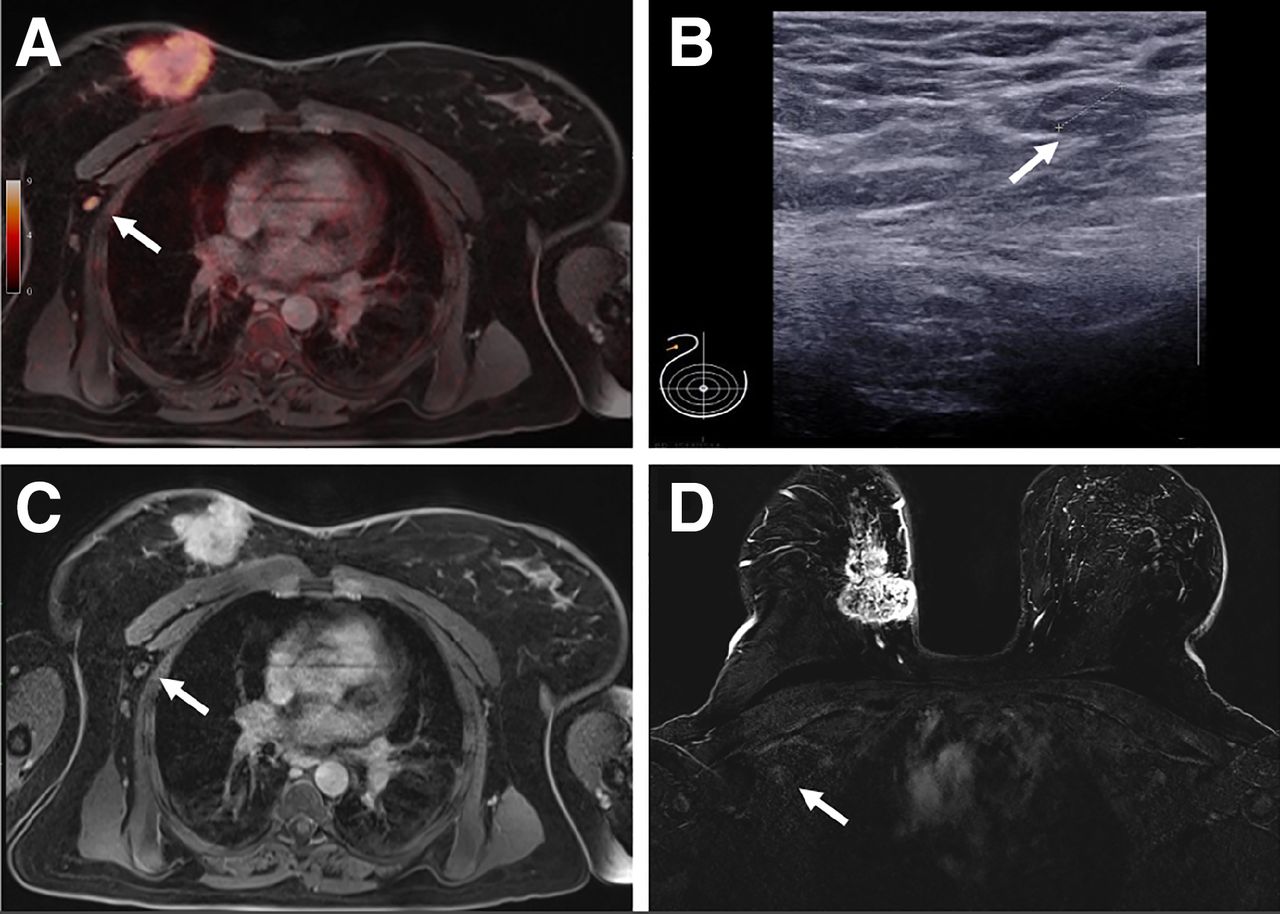
Pathologically confirmed axillary lymph node metastasis (arrows) that was correctly identified on 18F-FDG PET/MRI (A) because its tracer uptake was above background level (SUVmax, 4.7). This lymph node was rated false-negative on axillary sonography (B), thoracic MRI (C), and breast MRI (D).
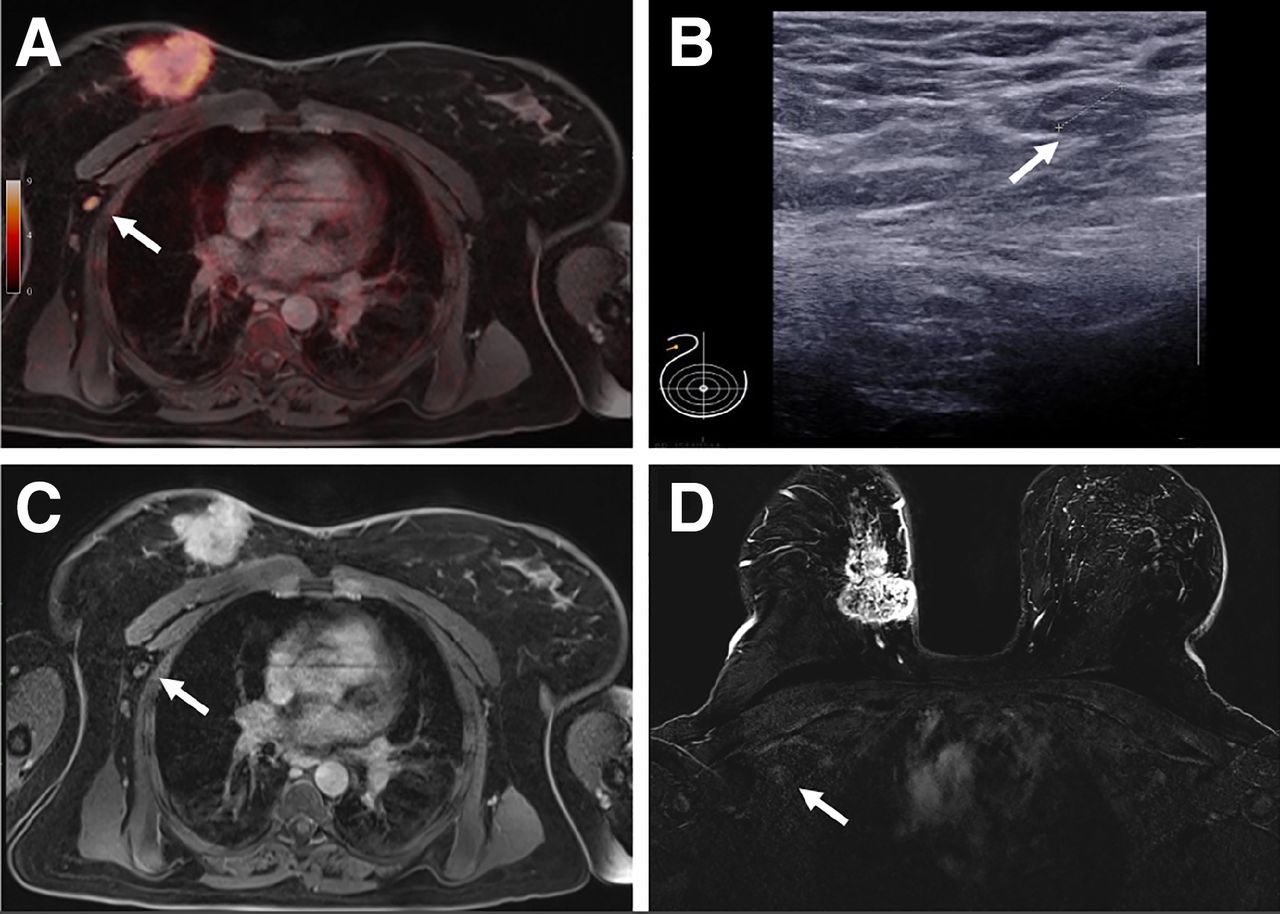
Pathologically confirmed axillary lymph node metastasis (arrows) that was correctly identified on 18F-FDG PET/MRI (A) because its tracer uptake was above background level (SUVmax, 4.3). It was also identified on axillary sonography (B) because of its cortical enlargement to 3.8 mm (short-axis diameter, 8 mm). This lymph node was rated nonsuggestive on thoracic MRI (C) and breast MRI (C). Large primary is seen in right breast.
Correct and False-Positive, as Well as Correct and False-Negative, Findings for the 4 Modalities
Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value, and Accuracy for the 4 Modalities
According to the reference standard, 8 of 44 nodal-positive patients (18.2%) were missed on thoracic PET/MRI; these patients were rated false-negative by the other 3 imaging modalities as well. Four of these patients received primarily operative therapy. The latency time between imaging and histopathologic sampling was 39.25 ± 4.38 d in these 4 patients. The remaining 4 patients received neoadjuvant chemotherapy, and the latency time between imaging and the start of chemotherapy was 18.25 ± 5.54 d.
Axillary sonography showed only one false-positive rating and the highest specificity. This patient was rated false-positive as well in breast MRI, thoracic MRI, and thoracic PET/MRI (Fig. 5). Thoracic PET/MRI showed 3 false-positive ratings, in 2 of which the primary tumor had previously been marked by a clip. These false-positive lymph nodes showed an SUVmax significantly lower than that of the correctly positive lymph nodes (3.73 ± 0.75 with a range of 3.0–4.5, vs. 6.31 ± 3.96 with a range of 2.6–17.7; P = 0.002).

Suggestive right axillary lymph node (arrows) seen on all imaging modalities. As no signs of malignancy were seen on histopathology, this lymph node was rated false-positive on all modalities. (A) Thoracic PET/MRI: 9 mm lymph node with loss of fatty hilum, very slight perifocal edema, and 18F-FDG uptake slightly above background level (SUVmax, 3.7). (B) Sonography: hypoechogenic lymph node with loss of fatty hilum (10 mm). (C) Thoracic MRI: 9-mm lymph node with loss of fatty hilum and very slight perifocal edema. (D) Breast MRI: 8-mm lymph node with loss of fatty hilum and contrast agent affinity.
DISCUSSION
In this study, we compared the diagnostic performance of 4 state-of-the-art imaging modalities regarding their ability to determine the axillary nodal status of 112 patients with newly diagnosed breast cancer. The results indicate that thoracic 18F-FDG PET/MRI is superior to thoracic MRI, prone breast MRI, and axillary sonography. While 18F-FDG PET/MRI offers the highest sensitivity, accuracy, and AUC for detecting locoregional lymph node metastases, axillary sonography is the imaging modality with the highest specificity.
Correctly identifying nodal status is crucial in patients with newly diagnosed breast cancer, because it is a major factor in choosing the optimal treatment strategy (21–24). Until some years ago, complete axillary dissection was the standard for axillary staging and at the same time was a procedure to achieve regional control (25). Because various studies have shown sentinel lymph node biopsy to be equal to axillary dissection for staging purposes, sentinel lymph node biopsy or equivalent procedures have evolved as the standard for patients with a clinically low risk of axillary nodal metastases (26–28).
Our results are in line with other studies, as they underscore that breast MRI has a minor role in evaluating the axillary nodal status of breast cancer. This limited role is due mostly to the limited field of view of breast MRI using dedicated breast coils that do not allow a complete assessment of the axillary region. Despite the introduction of more advanced MRI protocols or lymph node–specific contrast agents, the data have remained insufficient from an oncologic perspective (29).
Sonography comes with the advantage of low cost and wide accessibility, but the quality of the examination depends on the skill and experience of the examiner. Our data show axillary ultrasound to have a high specificity (98.5%) but a limited negative predictive value (83.8%). This drawback of axillary ultrasound has also been described by Farrell et al., who reported a high specificity of 100% but a risk of underestimating the number of affected lymph nodes (30).
In our study, 18F-FDG PET/MRI demonstrated the best diagnostic performance in detecting nodal-positive patients, compared with the other modalities (AUC of 0.892). Previous PET/MRI studies in primary breast cancer showed conflicting results regarding nodal staging: whereas Botsikas et al. and Grueneisen et al. found an equal or superior diagnostic performance for MRI alone compared with PET/MRI (31,32), van Nijnatten et al. showed an added value of dedicated axillary PET/MRI compared with MRI alone (33). Further studies even indicated that PET/MRI could lead to treatment changes or could replace invasive sampling, compared with conventional staging with MRI, ultrasound, or full-field digital mammography (12). In our study, 18F-FDG PET/MRI still missed about 18% of the nodal-positive patients while having the best negative predictive value of all imaging modalities (89%), emphasizing its high reliability in excluding malignancy in locoregional lymph nodes.
The highest specificity, on the other hand, was achieved by axillary sonography, which depicted only 1 false-positive finding, whereas PET/MRI lead to 3 false-positive ratings. Two of these 3 false-positive patients had previously undergone clip marking of the primary tumor, pointing to a reactive 18F-FDG uptake in these lymph nodes.
False-positive lymph nodes showed a significantly lower SUVmax than correctly positive lymph nodes. However, because the ranges in SUVmax in the 2 groups overlapped and the number of false-positive lymph nodes was very low, there is no reliable SUVmax cutoff.
There were limitations to this study. Most importantly, some samples were taken after neoadjuvant systemic therapy and therefore had to be evaluated retrospectively, taking into account indirect histopathologic indicators for metastasis such as focal posttherapeutic fibrosis or necrosis (18,19). Furthermore, several samples were taken as a percutaneous biopsy, representing only a part of a lymph node. In contrast to lymph node excision, this sampling method also bears a small residual risk of missing tumor cells. Furthermore, the prospective study design intended axillary sonography to be the first examination, as it was conducted in the same session as breast sonography and histopathologic sampling of the primary tumor to ensure accordance with the patient inclusion criteria. Therefore PET/MRI and MRI examinations were often performed after clip marking of the breast, which may have caused reactive axillary lymphadenopathy. Therefore, the number of false-positive findings in PET/MRI and MRI might be artificially increased.
Our data suggest that 18F-FDG PET/MRI provides the highest overall diagnostic performance, that 18F-FDG PET/MRI should be used to exclude metastatic spread to axillary lymph nodes, and that axillary sonography should be used to confirm the diagnosis of suspected nodal positivity. Consequently, future workflows should consider performing 18F-FDG PET/MRI as a searching tool before clip marking of the primary tumor, if applicable in clinical workflow, and to add axillary sonography afterward to specify findings. If both imaging modalities show a positive nodal status, one might even consider dispensing with axillary histopathologic sampling. Although tissue pathology will be the final determiner of the N stage, knowledge that PET/MRI is more sensitive than the other modalities will help in the growing field of targeted biopsy in the future. However, further prospective studies would be needed to investigate the potential replaceability of sampling by this approach.
CONCLUSION
18F-FDG PET/MRI outperforms axillary sonography, breast MRI, and thoracic MRI in determining the axillary lymph node status. In a clinical setting, the combination of 18F-FDG PET/MRI and axillary sonography might be considered to provide even greater accuracy in diagnosis.
DISCLOSURE
Wolfgang P. Fendler is a consultant for Endocyte and BTG, and he received fees from RadioMedix, Bayer, and Parexel outside the submitted work. The study was funded by the Deutsche Forschungsgemeinschaft (DFG), the German Research Foundation (BU3075/2-1; KI2434/1-2). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is the diagnostic performance of thoracic 18F-FDG PET/MRI better than that of thoracic MRI, breast MRI, and axillary sonography?
PERTINENT FINDINGS: Thoracic 18F-FDG PET/MRI showed the highest sensitivity (81.8%) and highest AUC (0.892) in assessing axillary nodal status, whereas axillary sonography was the most specific imaging modality (98.5%).
IMPLICATIONS FOR PATIENT CARE: PET/MRI might be used to exclude axillary metastatic disease, and axillary sonography might be added afterward to specify findings if PET/MRI shows nodal involvement.
Footnotes
Published online May 20, 2021.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication January 25, 2021.
- Revision received March 19, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of 18F-FDG PET/MRI on Therapeutic Management of Women with Newly Diagnosed Breast Cancer: Results from a Prospective Double-Center Trial
- Clinical Decision Support for Axillary Lymph Node Staging in Newly Diagnosed Breast Cancer Patients Based on 18F-FDG PET/MRI and Machine Learning
- Virtual Biopsy: Just an AI Software or a Medical Procedure?