


Article Figures & Data
Figures
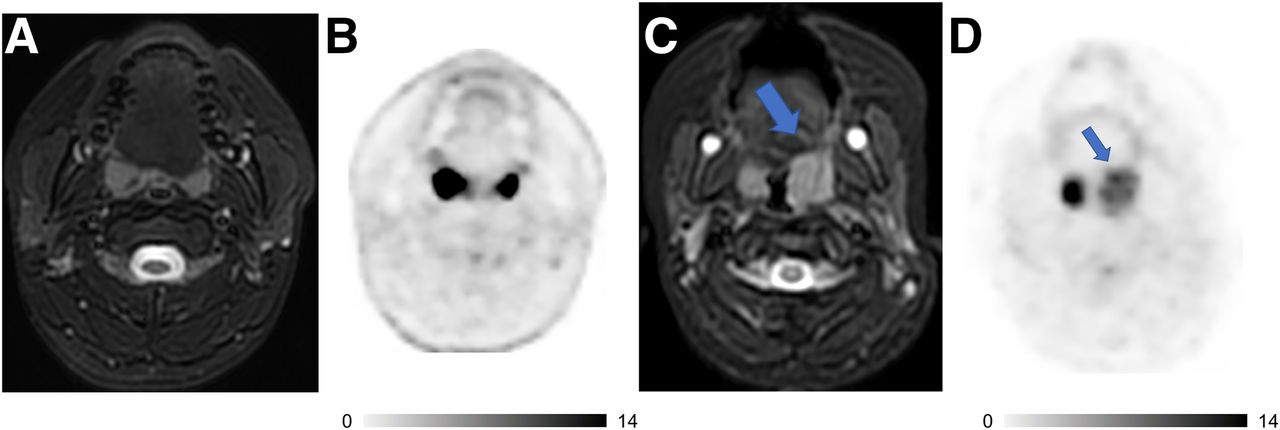
- FIGURE 1.
18F-FDG PET/MRI helps to characterize activity in tonsils and stage patients with lymphoma. (A and B) Axial T2-weighted fat-saturated fast-spin-echo (FSE) image (A) and 18F-FDG PET image (B) of 15-y-old boy with follicular lymphoma show symmetric morphology and marked 18F-FDG uptake of both tonsils with reactive hyperplasia. (C and D) Axial T2-weighted FSE image (C) and 18F-FDG PET image (D) of 4-y-old girl with large B-cell lymphoma demonstrate asymmetric globular enlargement and relatively less intensive 18F-FDG uptake of left tonsil (arrows). Tonsillectomy revealed large B-cell lymphoma in left tonsil and reactive tissue in right tonsil. Intrinsic uptake in tonsil is more avid than lymphomatous involvement on second patient. Radiologists must be cognizant of this caveat and integrate metabolic and morphologic information to increase diagnostic accuracy.
- FIGURE 2.
18F-FDG PET/MRI detects tumor invasion into spinal canal in 18-mo-old boy with metastasized germ cell tumor. (A) Sagittal short-inversion-time inversion recovery image, fused with simultaneously acquired 18F-FDG PET image, demonstrates presacral mass (red arrow), which extends into spinal canal. Also noted is 18F-FDG–avid lesion in S1 vertebra (yellow arrow) and extradural focus posterior to L4 vertebra (blue arrow). (B) Axial T2-weighted fast-recovery fast-spin-echo fat-saturated image shows soft-tissue mass entering spinal canal (red arrow). Also noted are metastatic lesions in S1 (yellow arrow) and right paraspinal muscle (orange arrow). (C) Fast-recovery fast-spin-echo fat-saturated image fused with 18F-FDG PET image shows hypermetabolism of all lesions. Information from PET/MRI helped in staging by showing metastatic disease and extent of disease in spinal canal, hence impacting patient management. Patient started chemotherapy right after PET/MRI.
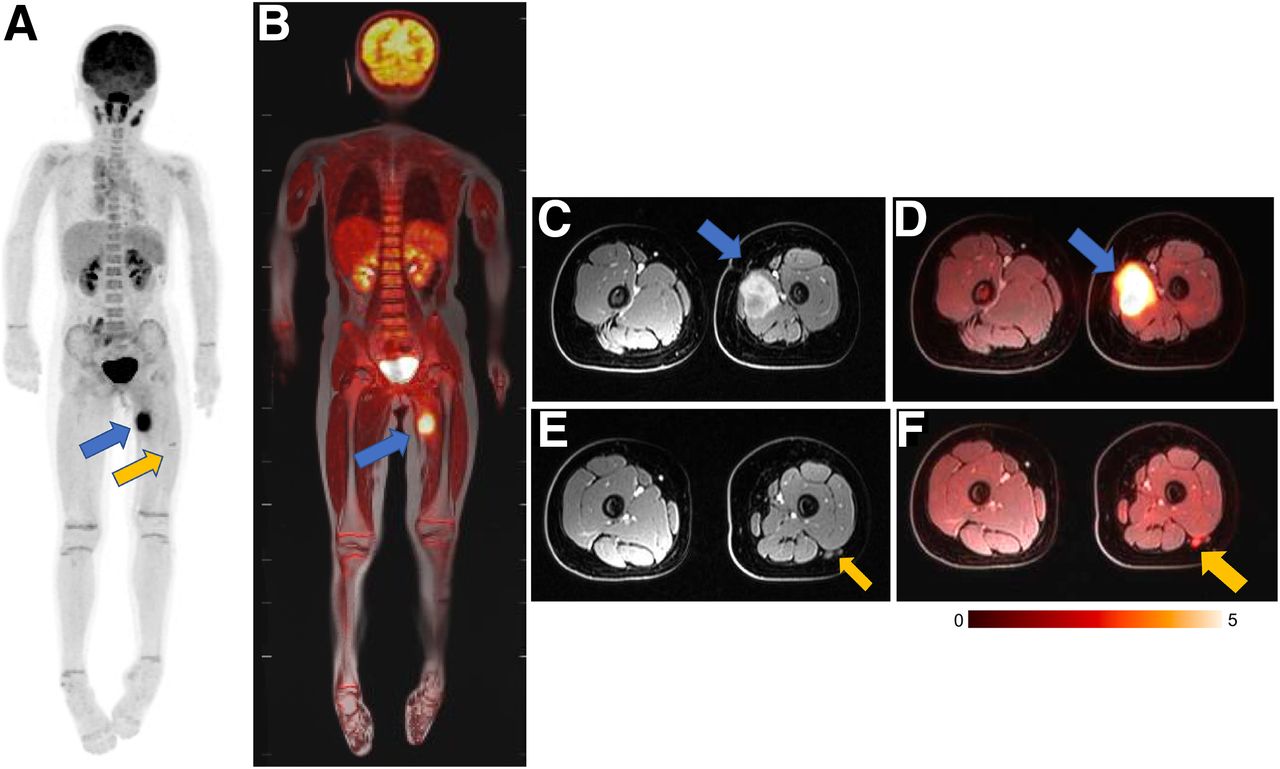
- FIGURE 3.
18F-FDG PET/MRI accurately stages rhabdomyosarcoma in 9-y-old girl. (A and B) Maximum-intensity projection of 18F-FDG PET scan (A) and 18F-FDG PET/MRI scan (B) show avid 18F-FDG uptake in lesion in thigh adductor muscles (blue arrow) and tiny additional 18F-FDG–avid lymph node in lateral thigh (yellow arrow). MRI helps to exclude any bone marrow disease or cortical invasion. (C and D) Axial contrast-enhanced fat-saturated T1-weighted MRI scan (C) and 18F-FDG PET/MRI scan (D) demonstrate relation between primary tumor (arrow) and superficial and deep femoral artery and vein. (E and F) Axial contrast-enhanced fat-saturated T1-weighted MRI scan (E) and 18F-FDG PET/MRI scan (F) demonstrate small lymph node (arrow) posterior to vastus lateralis muscle. Primary tumor and lymph node were resected and positive for sarcoma.
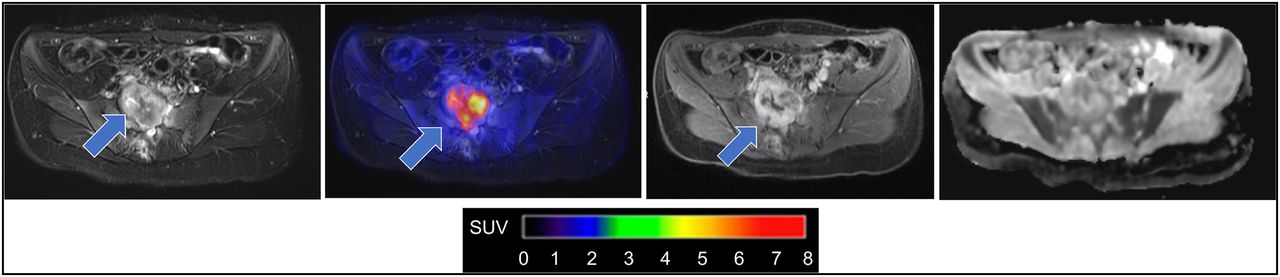
- FIGURE 4.
18F-FDG PET/MRI enabled image-informed surgical planning in 21-y-old patient with neurofibromatosis type 1. From left to right: axial fat-saturated T2-weighted image through pelvis reveals heterogeneous lesion infiltrating sacrum (arrow); 18F-FDG PET fused with T2-weighted MRI scan shows increased glucose metabolism of sacral lesion (SUVmax = 6; arrow); axial contrast-enhanced fat-saturated T1-weighted MRI scan shows heterogeneous tumor enhancement (arrow); apparent diffusion coefficient map demonstrates restricted diffusion of lesion with mean apparent diffusion coefficient of 0.85·10−3 mm2 s, which is suggestive of MPNST. Curative treatment of MPNST is critically dependent on early detection. Combined information from 18F-FDG PET and diffusion-weighted MRI led to tumor resection and histologic confirmation of MPNST.



Tables
- TABLE 1
18F-FDG PET/MRI Basic Protocols for Pediatric Oncology at 4 Different Medical Centers
Institution, scanner model, and FOV Basic protocol for children PET/MRI acquisition time and injected dose Chest CT Children’s Hospital of Philadelphia; GE Healthcare Signa (TOF); FOV, WB WB MRAC axial 3D T1 spoiled gradient echo (LAVA Flex); axial FRFSE Flex WB diffusion-weighted imaging (b = 50, 400, 800) (no intravenous contrast); local imaging if required Varies with patient height; WB scan; 30–60 min; PET, 3 min/bed ≥ 5 y or 4 min/bed < 5 y; injected dose, 3.7 MBq/kg Required Children’s Wisconsin; GE Healthcare Signa (TOF); FOV, WB WB MRAC; axial 3D T1 spoiled gradient echo (LAVA Flex) (sagittal and coronal reformats); axial FRFSE Flex (no intravenous contrast); local imaging if required Varies with patient height; WB scan < 30 min; PET, 3 min/bed; injected dose: 2.96 MBq/kg Only for small lung lesions University of Tübingen; Siemens Biograph mMR; FOV, WB WB MRAC; contrast-enhanced axial 3D T1 Dixon spoiled gradient echo (VIBE); WB STIR coronal; WB DWI (b = 50,800); local imaging if required Varies with patient height; WB scan, 45–90 min; PET, 6 min/bed; injected dose, 3.7 MBq/kg Only if therapeutic consequence is possible (e.g., resection of lung metastases in sarcoma) Stanford University; GE Healthcare Signa (TOF); FOV, WB WB MRAC; contrast-enhanced axial 3D T1 spoiled gradient echo (LAVA Flex); axial FRFSE Flex; WB DWI (b = 50, 600 or 800); local imaging if required Varies with patient height; WB scan, 60 − 90 min; PET, 4 min/bed; injected dose, 3.7 MBq/kg Only if therapeutic consequence is possible Typical WB PET/CT acquisition time for protocols mentioned in table is less than 30 min.
TOF = time of flight; FOV = field of view; WB = whole body; MRAC = MRI attenuation correction; 3D = 3-dimensional; T1 = T1-weighted; LAVA = Dixon liver acquisition with volume acquisition; Flex = fat/water separation; FRFSE = fast relaxation fast spin echo; bed = bed position; VIBE = volumetric interpolated breath-hold examination; DWI = diffusion-weighted imaging; STIR = short-inversion-time inversion recovery.
Tumor type Advantage Overall Simultaneous PET and MRI acquisition (precise registration of MRI and PET) One-stop local and whole-body staging Decreased ionizing radiation Reduced number of total examinations Better characterization of incidental findings More accurate measurement of lesions than with unenhanced CT Lymphoma Increased sensitivity to detect bone marrow involvement Avoidance of core biopsy if PET/MRI results are negative Reduced dose of ionizing radiation (particularly important for patients with therapy-refractory disease who need multiple scans to closely monitor treatment efficacy) Neurofibromatosis 1 and MPNST Detailed depiction of peripheral neurofibromata and central nervous system Optimal alignment of MRI and PET in cases of multiple neurofibromas Comprehensive examination of central nervous system and peripheral lesions in single examination Sarcoma Better characterization of bones and soft tissues Higher sensitivity for bone marrow metastases Improved monitoring of pediatric tumors after immunotherapy
Supplemental Data
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
{kind=link}