


Abstract
1192
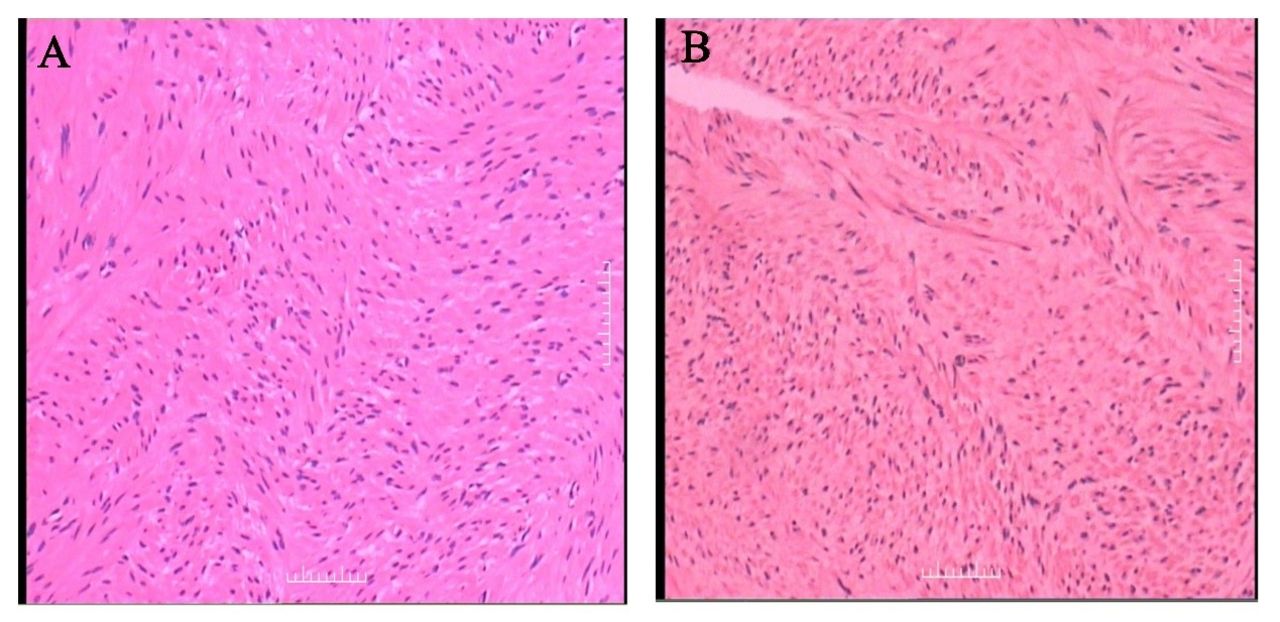
Objectives: 1. Highlight the indications of PET imaging in BML. 2. Evaluate the characteristics of MRI in BML. 3. How to analyze and integrate the two imaging methods to make a correct diagnosis of BML. Abstract: Benign metastasizing leiomyoma (BML) is a rare disease entity that usually occurs in females of reproductive age with a prior history of uterine leiomyoma. Patients are usually asymptomatic and the tumors tend to grow gradually. 18FFDG PET/CT is useful for distinguishing malignant leiomyosarcoma from benign leiomyoma. The metabolic behavior of most BML cases in 18FFDG PET/CT is lacking/low uptake, and only a few cases have high FDG uptake. A 37-year-old female patient presented with a double adrenal mass upon routine physical examination. Ultrasonography suspected adrenal malignant metastases. To distinguish tumors from malignancy, the patient underwent PET/CT scans which showed low 18F-FDG uptake. More masses were detected in the left lower abdominal wall, uterus and pelvic cavity. The FDG activity in all the masses was unremarkable, which means those masses suggested to be benign. In this case, the relationship between the mass and the adrenal gland was determined by MRI. Dynamic contrast enhancement revealed a gradual contrast enhancement of masses, which is the characteristic appearance of leiomyoma enhancement on MRI. Retrace the patient history, the patient has a history of laparoscopic minimally invasive surgery for uterine fibroids when she was 35-year-old, the mass of the left lower abdominal wall was sited on the minimally invasive surgical site. Combined with the patient's history of uterine fibroids, it is straightforward to make a diagnosis of BML. The result of histological examination demonstrated BML from the retroperitoneum. When evaluating a retroperitoneal mass, the physician should remember that BML might arise from this region. Figure 1. The MIP of 18F-FDG PET (A), the axial slice of the CT (B, D, F, H), and the fused PET/CT (C, E, G, I) images of masses (white arrow) showed unremarkable FDG activity. Figure 2. The lesions (white arrow) on the T1-weighted image (A), the T2-weighted image (B), the T2-weighted coronal plane (C), dynamic contrast enhancement (D-G), the diffusion weighted image (H). Several masses (white arrow) showed low signal on the T2WI (I-K). Figure 3. Histopathological findings (hematoxylin-eosin stain, magnification×100) (A) had an appearance that consisted of interlaced bundles of spindle shaped tumor cells. Immunohistochemistry images (B) revealed the cells were positive for Smooth Muscle Antigen (SMA), desmin, and actin, consistent with a diagnosis of leiomyoma.



In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.