


Article Figures & Data
Figures
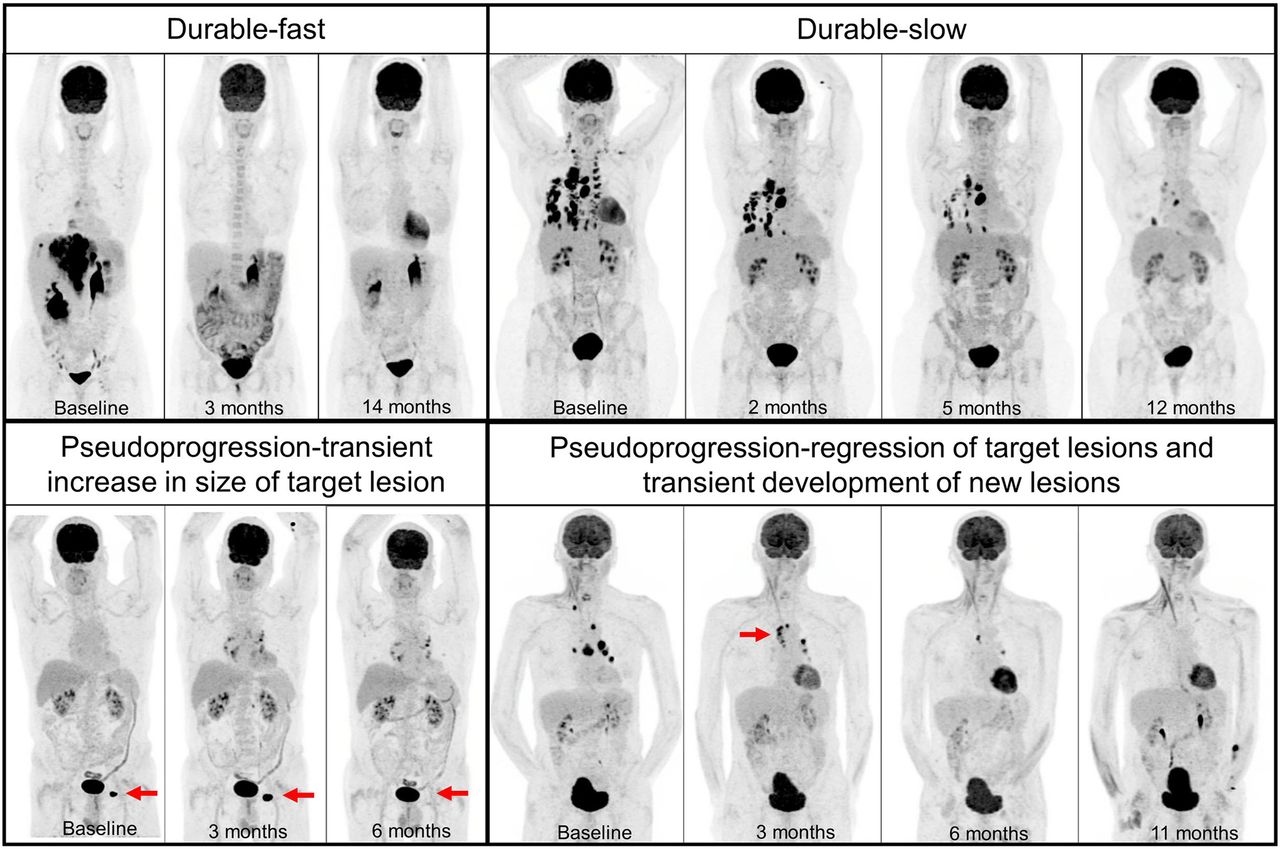
- FIGURE 1.
Four patterns of response: durable-fast (metastatic melanoma with early complete metabolic response after 4 cycles of ipilimumab and nivolumab at 3 mo, which had to be stopped because of colitis), durable-slow (metastatic NSCLC with gradual decrease in tumor burden in response to pembrolizumab), pseudoprogression-transient increase in size of target lesion (metastatic melanoma with initial increase in size of left inguinal lymph node [arrow] and subsequent resolution), and pseudoprogression-regression of target lesions and transient development of new lesions (metastatic squamous cell carcinoma with development of new mediastinal lymph nodes [arrow] despite regression of baseline lesions and subsequent complete metabolic response).
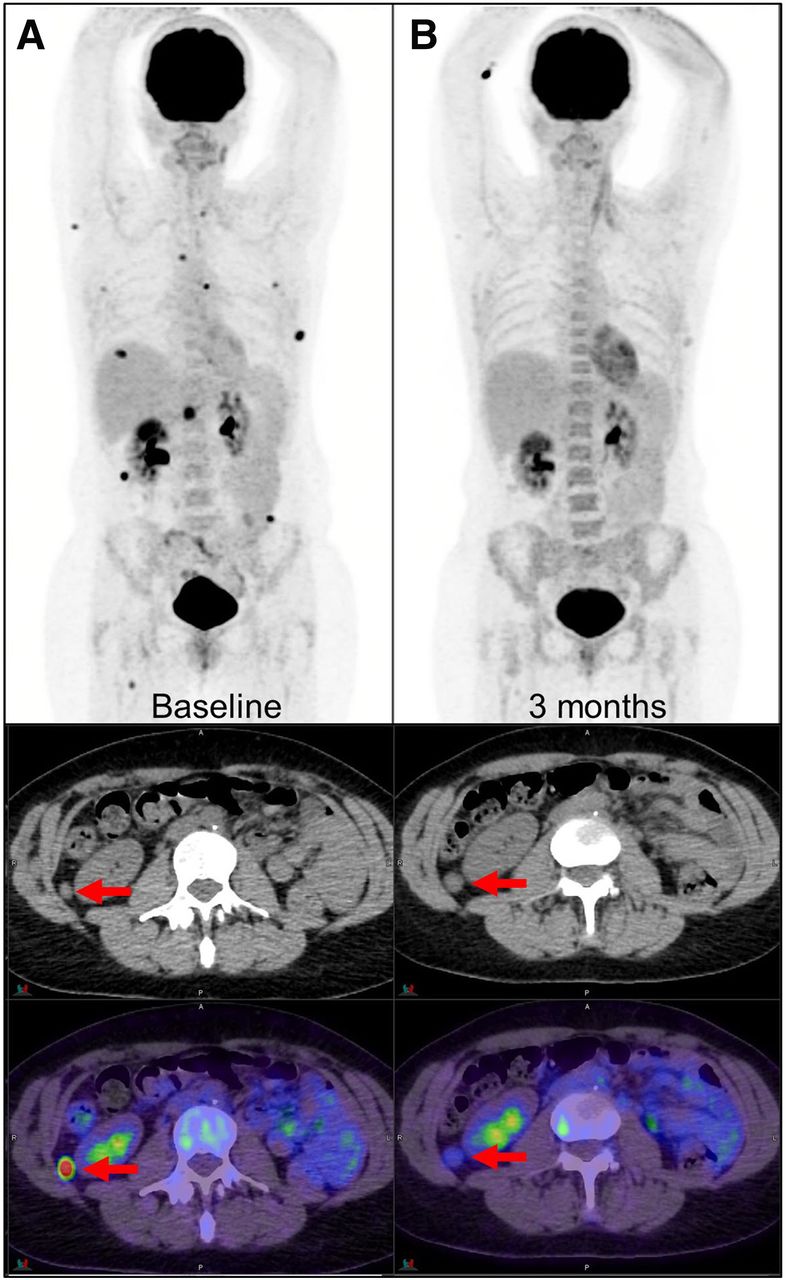
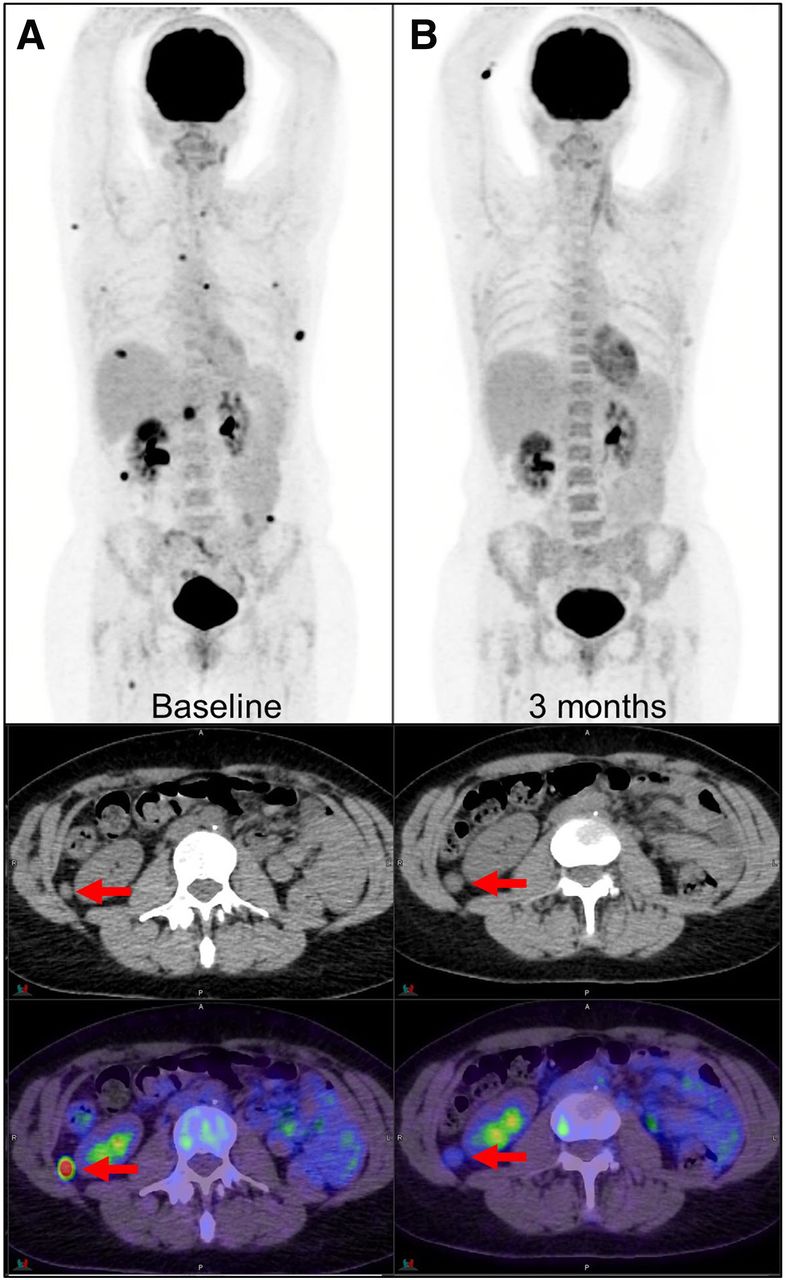
- FIGURE 2.
Metabolic response with residual morphologic lesion (arrows) as seen on PET (top), CT (middle), and PET/CT (bottom) images. (A) Metastatic melanoma at baseline shows multiple 18F-FDG–avid metastases. (B) At 3 mo after treatment with 4 cycles of immunotherapy, marked metabolic response is seen on PET, but residual soft-tissue lesions persist on CT (arrows). Diffuse bone marrow 18F-FDG uptake on posttreatment scan is suggestive of systemic immune response.
- FIGURE 3.
Primary oligoprogression: metastatic melanoma with dissociated response 3 mo after treatment with pembrolizumab demonstrating regression of some sites (solid arrows) and progression of other sites (arrowheads); at 6 mo, solitary hepatic metastasis continued to progress (dashed arrows). Secondary progression: metastatic melanoma with complete response at 5 mo after combination ipilimumab and nivolumab with subsequent secondary progression in solitary left adrenal metastasis (arrow); patient underwent adrenalectomy and continued single-agent nivolumab.
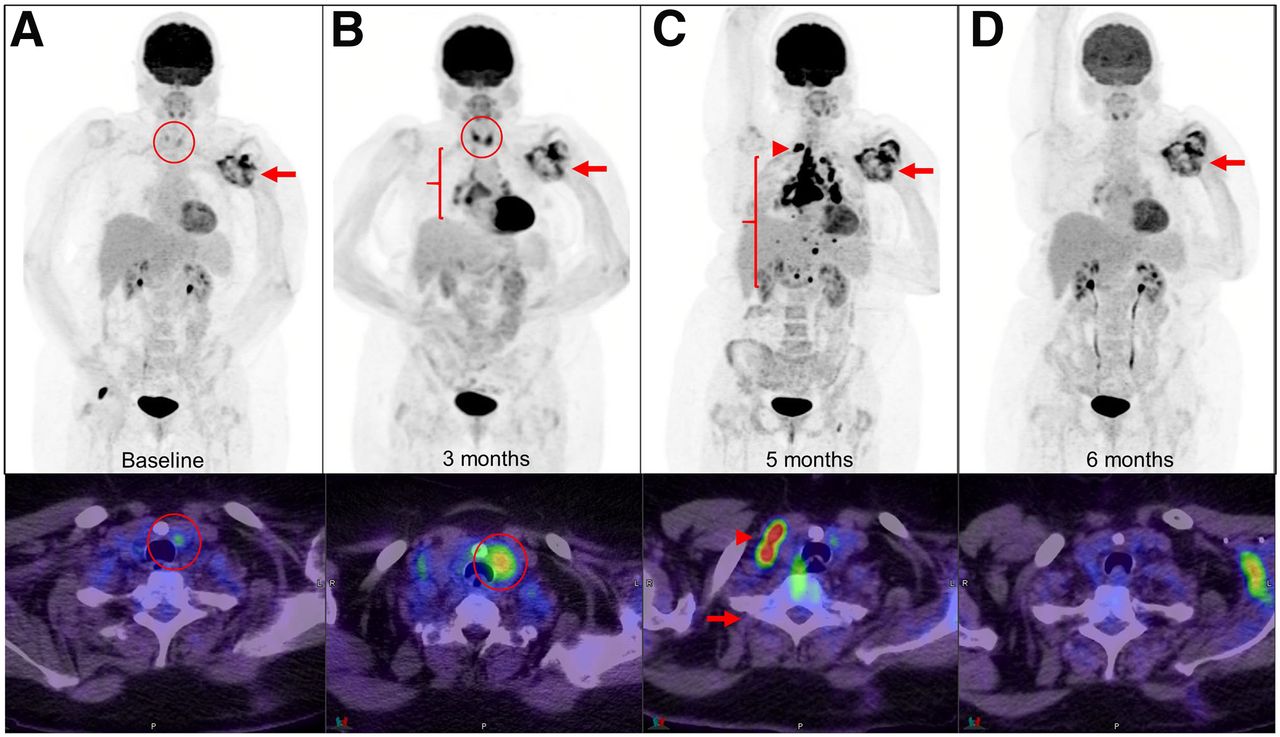
- FIGURE 4.
Sarcoidosis with widespread lymphadenopathy. Metastatic squamous cell carcinoma was treated with pembrolizumab, with stable disease in left axillary region (arrows). At 3 mo, sarcoidlike lymphadenopathy in chest was noticed (B, bracket). This finding progressed at 5 mo, with right supraclavicular (C, arrowhead) and upper abdominal nodal involvement. After short course of corticosteroids, sarcoidosis resolved completely. Underlying mild thyroiditis became exacerbated at 3 mo (circled).


Tables
Parameter PECRIT (15) PERCIMT (17) imPERCIST 5 (18) Tumor type Melanoma Melanoma Melanoma ICI Anti-CTLA-4 Anti-CTLA-4 Anti-CTLA-4 n 20 41 60 Timing 3–4 wk 3 mo 3 mo Standard of reference Clinical benefit: PR or CR at 4 mo or SD ≥ 6 mo per RECIST 1.1 (45) Clinical benefit: composite of clinical follow-up, 18F-FDG PET/CT, brain MRI, and LDH Follow-up and overall survival Definition of response CR or PR: per RECIST 1.1 CR: resolution of all lesions on PE, 18F-FDG PET/CT, and brain MRI; decrease or no increase in LDH; no new lesion CR, PR, or SD: per PERCIST in 5 lesions PR: decrease in size or resolution of lesions on PE, 18F-FDG PET/CT, and brain MRI; decrease or no increase in LDH; no new lesion SD: per RECIST 1.1 and >15.5% increase in SULpeak per PERCIST (46) SD: neither CR/PR nor PD Definition of progression Per RECIST 1.1 No clinical benefit and new lesions on 18F-FDG PET/CT as follows Change in sum of SULpeak in 5 lesions > 30% For lesions < 1 cm require ≥ 4 new lesions For lesions 1–1.5 cm require ≥ 3 new lesions New lesions can be incorporated For lesions > 1.5 cm require ≥ 2 new lesions Emphasis and advantages Combining anatomic and metabolic criteria Incorporation of clinical benefit in criteria New lesions are incorporated to sum of metabolic activity of lesions and not immediately considered PD Early response assessment Number and metabolic size of new lesions on 18F-FDG PET/CT PECRIT = PET/CT Criteria for Early Prediction of Response to ICI Therapy; PERCIMT = PET Response Evaluation Criteria for Immunotherapy; imPERCIST = Immunotherapy-Modified PERCIST; LYRIC = Lymphoma Response to Immunotherapy Criteria; iPERCIST = Immune PERCIST; HL = Hodgkin lymphoma; PR = partial response; CR = complete response; SD = stable disease; LDH = lactate dehydrogenase; PE = physical examination; CMR = complete metabolic response; PMR = partial metabolic response; SMD = stable metabolic disease; PD = progressive disease; SULpeak = lean body mass–corrected SUVpeak; PMD = progressive metabolic disease; UPMD = unconfirmed PMD; IR = indeterminate response; SPD = sum of product of diameters; CPMD = confirmed progressive metabolic disease; PPD = product of perpendicular diameters.
Parameter LYRIC (19,20) iPERCIST (22) Tumor type HL NSCLC ICI Anti-PD-1 Anti-PD-1 n 16 28 Timing 3 mo 2 mo Standard of reference Multidisciplinary experts’ consensus based on clinical and imaging results Clinical benefit and confirmatory 18F-FDG PET/CT or CT 4 wk later Definition of response CR or PR: per Lugano (21) CMR, PMR, or SMD: per PERCIST Definition of progression Per Lugano with following exceptions PMD as per PERCIST is considered UPMD IR1: ≥50% increase in SPD in first 12 wk IR2a: <50% increase in SPD with new lesions UPMD needs to be confirmed by second 18F-FDG PET/CT at 4–8 wk later to be classified as CPMD IR2b: <50% increase in SPD with ≥50% increase in PPD of lesion or set of lesions at any time during treatment IR3: increase in 18F-FDG uptake without concomitant increase in lesion size meeting criteria for PD Emphasis and advantages Introduction of concept of IR categories until biopsy or subsequent imaging confirms either pseudoprogression or true progression Introduction of concept of UPMD with clinical stability Allowing treatment continuation PECRIT = PET/CT Criteria for Early Prediction of Response to ICI Therapy; PERCIMT = PET Response Evaluation Criteria for Immunotherapy; imPERCIST = Immunotherapy-Modified PERCIST; LYRIC = Lymphoma Response to Immunotherapy Criteria; iPERCIST = Immune PERCIST; HL = Hodgkin lymphoma; PR = partial response; CR = complete response; SD = stable disease; LDH = lactate dehydrogenase; PE = physical examination; CMR = complete metabolic response; PMR = partial metabolic response; SMD = stable metabolic disease; PD = progressive disease; SULpeak = lean body mass–corrected SUVpeak; PMD = progressive metabolic disease; UPMD = unconfirmed PMD; IR = indeterminate response; SPD = sum of product of diameters; CPMD = confirmed progressive metabolic disease; PPD = product of perpendicular diameters.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Approaches to Imaging Immune Activation Using PET
- CD70-Targeted Immuno-PET/CT Imaging of Clear Cell Renal Cell Carcinoma: A Translational Study
- Fibroblast Activation Protein and Glycolysis in Lymphoma Diagnosis: Comparison of 68Ga-FAPI PET/CT and 18F-FDG PET/CT
- Signaling Pathways That Drive 18F-FDG Accumulation in Cancer