


Abstract
Immunotherapy agents are now entering the clinic in a wide array of malignancies and have provided a valuable addition to the therapeutic armamentarium. These agents enhance the global immune response by modulating the tumor microenvironment but can lead to unconventional patterns of response, challenging the conceptual framework that imaging is a robust surrogate for therapeutic efficacy. There is also increasing evidence that an effective antitumor response requires a systemic immune response in primary and secondary lymphoid tissues. However, an enhanced systemic immune response can lead to disruption of immunologic hemostasis in healthy tissues, causing adverse events. Better understanding of the complex interplay between tumoral and systemic immune response has been provided through tissue and liquid biopsy. However, the applicability of these methods is constrained by the biologic, spatial, and temporal heterogeneity of the processes involved. There is a growing interest in molecular imaging of cell-specific lineage markers of the immune system using biomolecules. However, the ongoing role of the more widely available 18F-FDG PET/CT for response assessment is being recognized through ongoing refinement of interpretative guidelines and emerging evidence. These noninvasive methods provide insights into the biologic basis of the global immune response to maximize potential therapeutic benefit. In this review, we aim to provide an overview of the current status of 18F-FDG PET/CT in the monitoring of tumoral and systemic immune response. In a companion review, the role of other imaging probes that might complement 18F-FDG PET/CT will be discussed.
Harnessing the immune system to destroy cancer cells represents an evolving therapeutic strategy in oncology. Research into the complex interaction between multiple cell types and the tumor microenvironment in mediating antitumor immunity has laid the foundation for strategies to enhance cancer eradication. Critical limbs of this response are recognition and presentation of tumor-associated antigens by dendritic cells, priming and activation of peripheral immune cells, trafficking, and infiltration of T cells into the tumor microenvironment, leading to tumor-cell recognition and immune-mediated cell death (1). Therapeutic strategies targeting different elements of this process have demonstrated promising clinical efficacy. These include monoclonal antibodies that act as immune checkpoint inhibitors (ICIs), particularly anticytotoxic T-lymphocyte antigen 4 (anti-CTLA-4) and antiprogrammed death receptor 1 and its ligand (anti-PD-1 and PD-L1, respectively) (2). Anti-CTLA-4 agents primarily invoke T-cell priming and expansion in lymph nodes, whereas anti-PD-1 and PD-L1 agents act predominantly within the tumor microenvironment by blocking immunosuppressive interaction between PD-1 on T cells and PD-L1 on cancer cells (2). These disparate mechanisms of action account, at least partially, for the differing patterns of response seen clinically. There is also increasing evidence that an effective antitumor immune response requires a more global immune response involving secondary lymphoid tissues such as lymph nodes and the spleen (3).
Despite complete and durable responses in a subset of patients, most patients do not respond to current immunotherapy regimens, and new predictors of response and mechanisms of resistance need to be defined. A large body of evidence has been provided by large-scale clinical trials using morphologic imaging indicating the limitations of traditional response assessment posed by unconventional responses, leading to the various reclassifications of response criteria based on CT or MRI (4). Molecular imaging potentially provides noninvasive monitoring of the global immune response during treatment. Although immune-PET, using tracers directed to cell-specific lineage targets or activation markers, offers the promise of enriching our understanding of the immune system, it is in the early stages of development. Despite challenges, the utility of 18F-FDG PET/CT, which is widely accessible worldwide, is being increasingly defined and refined. In this review, we aim to provide an overview of the current status of 18F-FDG PET/CT in monitoring of tumoral and systemic immune response. Recognizing the limitations of morphologic imaging in monitoring of immunotherapy response systemically, we explore the incremental value of 18F-FDG PET and PET/CT in the monitoring of the global immune response. In a companion review, we will detail future opportunities for the use of more specific tracers of immune phenomena and how these might complement the role of 18F-FDG PET/CT.
18F-FDG PET/CT IMAGING OF THE IMMUNE SYSTEM
Glycolysis as a Marker of Immune Activation
The Warburg effect represents metabolic reprogramming of cancer cells to favor glycolytic metabolism (5). This process has underpinned the success of 18F-FDG PET/CT in oncology. Although linked to cancer cell growth and proliferation, there is increasing evidence that aerobic glycolysis is also a key process in immune cell activation and differentiation (6). After antigen-induced activation, metabolism determines the fate of immune cells (7). T cells, importantly of the cytotoxic CD8 subtype, rapidly transition from catabolic states (naïve and memory T cells) to growth and proliferation (effector T cells) during immune response (8,9). Glucose is transported into T cells via the high-affinity glucose transporter 1, the major glucose transporter on both T cells and cancer cells (10). Deconvolving these disparate contributions to metabolic signature in tumor sites from cancer cells, tumor stroma, and infiltrating immune cells poses a challenge to accurate response assessment and has led to modification of conventional response assessment criteria. However, in nontumor tissue, 18F-FDG PET/CT can enhance our understanding of the systemic immune response to immunooncology therapeutic strategies that may manifest as immune-related adverse events (irAEs).
In the following section, the evidence provided by large-scale clinical trials using morphologic imaging will be discussed in the context of the evolving clinical experience with 18F-FDG PET/CT.
Pseudoprogression: Lessons Learned from Morphologic Imaging
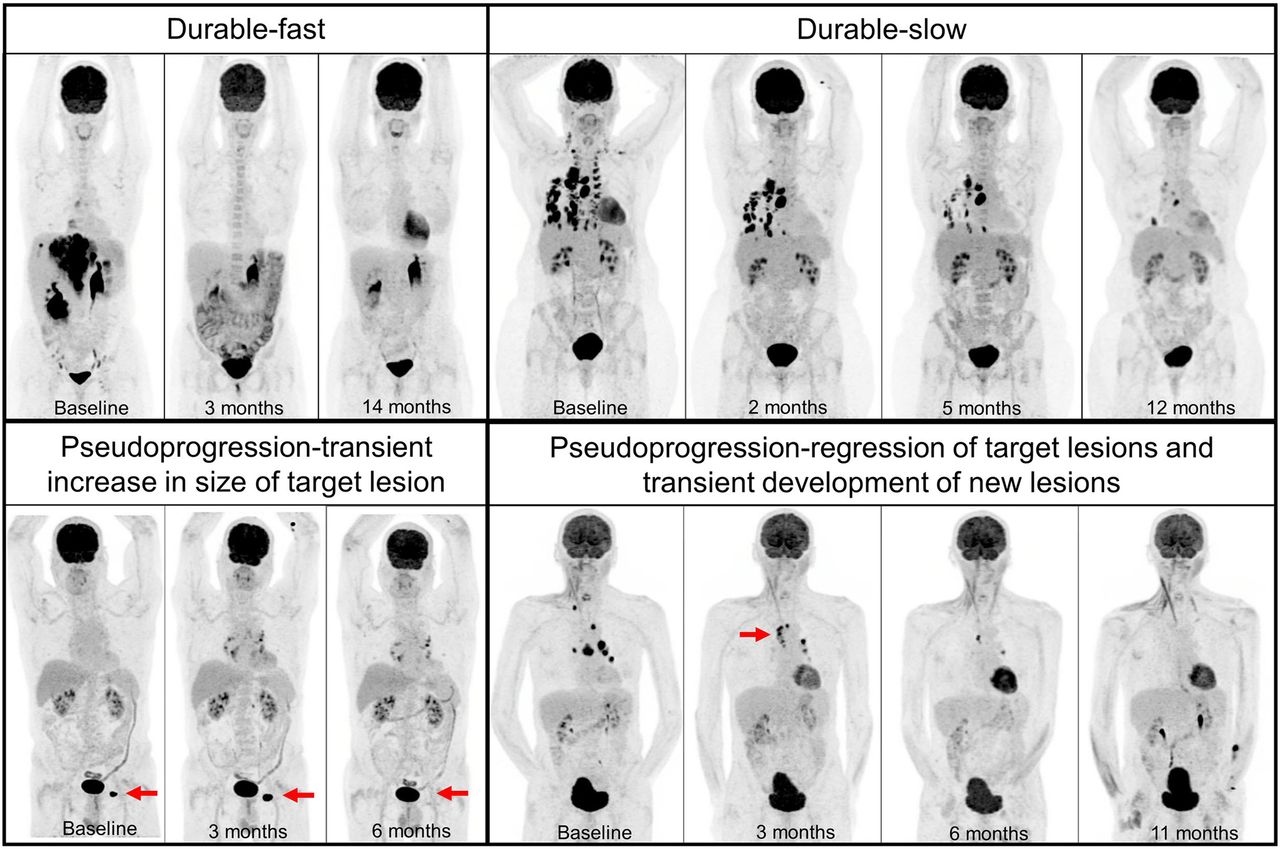
Initial experience with anti-CTLA-4 (ipilimumab) therapy in a phase II study involving 227 patients with advanced melanoma identified 4 distinct patterns of response (11). These included response in baseline lesions—evident by week 12—with no new lesions; stable disease, which in some patients was followed by a slow and steady decline in total tumor burden; responses after an initial increase in total tumor burden; and a reduction in total tumor burden during or after the appearance of new lesions at time points later than week 12 (Fig. 1). Although the first 2 response patterns were captured by conventional response criteria, the latter 2 responses were considered unconventional and later labeled as pseudoprogression. This group constituted approximately 10% of the cohort and had a significantly better survival than nonresponders, supporting the concept of treating beyond conventional morphologic progression. The importance of tumor burden in the immune-related response evaluation criteria was highlighted in this study since even when the measurements of new lesions were included in the calculation of lesion diameters, the net effect was a decline in some patients.

Four patterns of response: durable-fast (metastatic melanoma with early complete metabolic response after 4 cycles of ipilimumab and nivolumab at 3 mo, which had to be stopped because of colitis), durable-slow (metastatic NSCLC with gradual decrease in tumor burden in response to pembrolizumab), pseudoprogression-transient increase in size of target lesion (metastatic melanoma with initial increase in size of left inguinal lymph node [arrow] and subsequent resolution), and pseudoprogression-regression of target lesions and transient development of new lesions (metastatic squamous cell carcinoma with development of new mediastinal lymph nodes [arrow] despite regression of baseline lesions and subsequent complete metabolic response).
The type of ICI may impact the observed rate of pseudoprogression, with a lower rate reported in anti-PD-1/PD-L1 than in anti-CTLA-4. In a subset of patients in KEYNOTE-001 with advanced melanoma receiving pembrolizumab (anti-PD-1), the rate of pseudoprogression was 7.3%, which was lower than the observed rate in the context of ipilimumab despite using the same criteria (12). In two thirds of cases, pseudoprogression was observed before 12 wk (early), whereas in one third it occurred after 12 wk (delayed), potentially impacting the timing and interpretation of early response assessment.
It appears that the rate of pseudoprogression also differs depending on the tumor type. A retrospective analysis of clinical trials using atezolizumab (anti-PD-L1) involving over 800 patients with various malignancies showed a higher rate of pseudoprogression in melanoma than in non–small cell lung cancer (NSCLC), 7.3% compared with 2.3%–2.8%, respectively (13). In this report, only a transient increase in the size of target lesions was considered pseudoprogression when assessed within 90 d of starting atezolizumab. The patients with regression after initial target lesion progression had longer overall survival than those who did not have subsequent regression. In addition, patients with initial progression with new lesions but no progression of preexisting lesions tended to have similar or shorter overall survival than those with initial progression in target lesions. Therefore, the appearance of new lesions on morphologic imaging remains of clinical relevance regardless of the changes in the preexisting lesions.
Pseudoprogression: What 18F-FDG PET/CT May Offer
The optimal timing for evaluating the efficacy of immunotherapy with 18F-FDG PET/CT remains uncertain. Early stratification of response would be desirable to limit the significant toxicity and financial burden of ICIs. Although the early metabolic response has provided a significant advantage for 18F-FDG PET/CT over morphologic imaging in the context of targeted treatment (14), extrapolation of this principle to ICIs has proven challenging. In a pilot study, involving 20 patients with advanced melanoma, predominantly receiving anti-CTLA-4, PERCIST at 1 mo had lower accuracy than RECIST 1.1 to predict the best overall response (15). By combining RECIST and PERCIST, a new set of criteria was devised. This was called the PET/CT Criteria for Early Prediction of Response to ICI Therapy and was demonstrated to have higher accuracy than RECIST or PERCIST (Tables 1 and 2). The additional value of PET was apparent by subclassifying the patients with stable disease (by RECIST) but an increase of more than 15% in 18F-FDG uptake, which was paradoxically associated with eventual clinical benefit. Presumably, this increase reflected immune cell infiltration or activation in the tumor microenvironment. In another study, 18F-FDG PET/CT response at week 6 after starting an anti-PD-L1 ICI (atezolizumab) in the setting of NSCLC was not significantly different from CT response (16). However, in patients with stable disease by CT, an increase in whole-body metabolic tumor volume (wbMTV) was associated with a worse survival outcome emphasizing the incremental value of 18F-FDG PET/CT metabolic parameters.
Immune-Modified 18F-FDG PET Response Criteria—PECRIT, PERCIMT, and imPERCIST
Immune-Modified 18F-FDG PET Response Criteria—LYRIC and iPERCIST
To account for the transient appearance of new lesions (pseudoprogression) on 18F-FDG PET/CT, novel response criteria, termed the PET Response Evaluation Criteria for Immunotherapy, were devised incorporating the number and size of the newly emergent lesions (17). As new-lesion size increased, there was a reduction in the number of new lesions that were required to identify patients at increased risk of death (Tables 1 and 2). Interestingly, the authors also showed that the change in 18F-FDG uptake by the lesions did not significantly differ between responders and nonresponders.
In contrast, in another attempt to address pseudoprogression, the emphasis was put on the intensity of 18F-FDG uptake (Tables 1 and 2) (18). In this study, the change in the sum of 18F-FDG uptake (per PERCIST) by 5 lesions was used, and new lesions did not immediately indicate progressive disease. This criterion was termed Immunotherapy-Modified PERCIST 5, and was compared with PERCIST response using either 1 or 5 lesions. By all 3 methods of response assessment, responders on 18F-FDG PET/CT had markedly improved outcome based on survival at 2 y.
The importance of tumor type in immunotherapy response evaluation was highlighted in nonsolid tumors by 2 studies on Hodgkin lymphoma (19,20). In both studies, Lymphoma Response to Immunotherapy Criteria, which is an immunotherapy-modified version of the Lugano criteria, were applied at approximately 3 mo after commencement of anti-PD-1. The Lymphoma Response to Immunotherapy Criteria differ only in the definition of progression, with introduction of the concept of an indeterminate-response category, which requires either a biopsy or subsequent imaging to confirm or refute progression (Tables 1 and 2) (21). In a multicenter study involving 45 patients, all 16 patients with an indeterminate response at 3 mo had confirmed progression subsequently (20). Lymphoma Response to Immunotherapy Criteria and the Lugano criteria performed identically, and both demonstrated a significant prognostic stratification of patients with progression compared with those without progression. The concept of unconfirmed progressive disease or an indeterminate response, which requires a subsequent confirmatory study, has been used for morphologic imaging in solid tumors (4). Applying the same concept, an immune PERCIST has also been devised in a study on 28 patients with NSCLC receiving nivolumab (Tables 1 and 2) (22). Of 13 patients with unconfirmed progressive metabolic disease, only 4 patients were clinically stable enough to undergo the subsequent confirmatory study 4 wk later, with the remaining 9 patients stopping immunotherapy because of clinical deterioration. Although these studies have enhanced our understanding of the challenges facing response assessment by 18F-FDG PET/CT, current evidence is driven predominantly from single-center studies with a limited number of patients. Therefore, caution should be exercised in extrapolation and validation of these criteria across ever-increasing immunooncology therapeutic indications and strategies.
In summary, given that pseudoprogression is uncommon, the decision to continue immunotherapy beyond progression on either morphologic or conventional molecular imaging criteria should be made with caution and considered in selected patients who do not experience severe toxicity from these agents and whose disease-related symptoms have improved or stabilized on treatment. Assuming clinical stability, in these cases, a confirmatory follow-up study or histologic assessment of the new lesions can be considered. Since the management decisions early in treatment are made primarily on the basis of clinical benefit, the utility of imaging early during treatment could be questioned unless other incremental diagnostic information can be obtained that has prognostic or therapeutic implications. Key among these may be the ability to identify hyperprogression and irAEs.
Surveillance Imaging by 18F-FDG PET/CT in the Setting of Initial Response
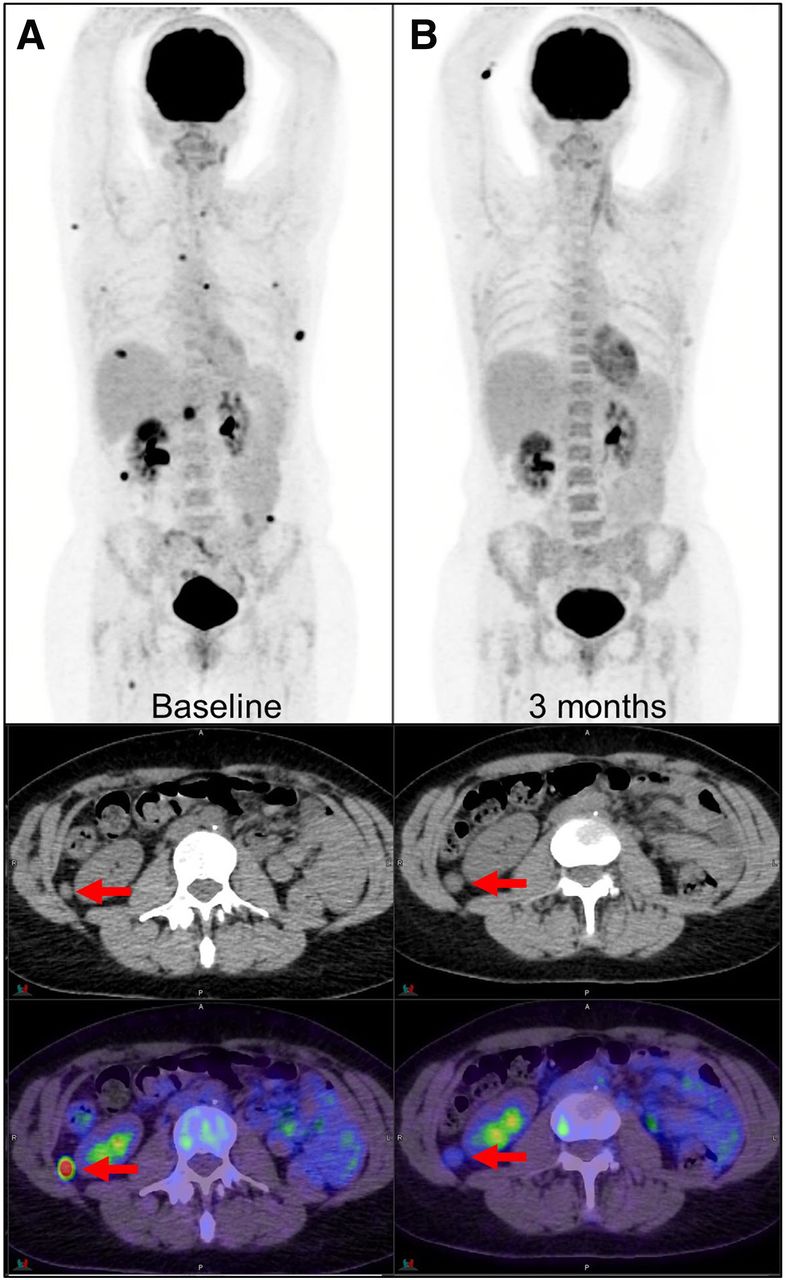
A major hallmark of immunotherapy is its potential to achieve durable and sometimes complete responses in a subset of patients with advanced cancer (23,24). This novel pattern of response challenges the conventional concept of continuing treatment until either disease progression or development of toxicity. It also has implications for the duration of ongoing surveillance. There is no standardized definition for a durable response, and the optimal treatment duration in the case of complete response remains to be defined (25). In a retrospective study involving 104 patients with advanced melanoma who were deemed responsive at 1 y, 28% had complete response, 66% had partial response, and 6% had stable disease on CT, whereas 75% had complete metabolic response, 16% partial metabolic response, and 9% stable metabolic disease or progressive metabolic disease on 18F-FDG PET/CT. Complete metabolic response was observed in 68% of patients with partial response on CT, and almost all patients (96%) with complete metabolic response had an ongoing response to therapy thereafter (Fig. 2) (26). 18F-FDG PET/CT was more predictive of the long-term outcome than CT. This finding might limit the frequency and duration of imaging surveillance, reducing costs and alleviating the anxiety that can accompany ongoing disease surveillance. Further studies are required to determine optimal surveillance paradigms for patients who achieve a complete response and whether cessation of surveillance can be achieved earlier by imaging with 18F-FDG PET/CT/CT than by imaging with CT. A further potential benefit of 18F-FDG PET/CT may be to identify oligometastatic sites of residual disease in the context of a more general systemic response. These may be amenable to local treatments, including surgery or radiotherapy.
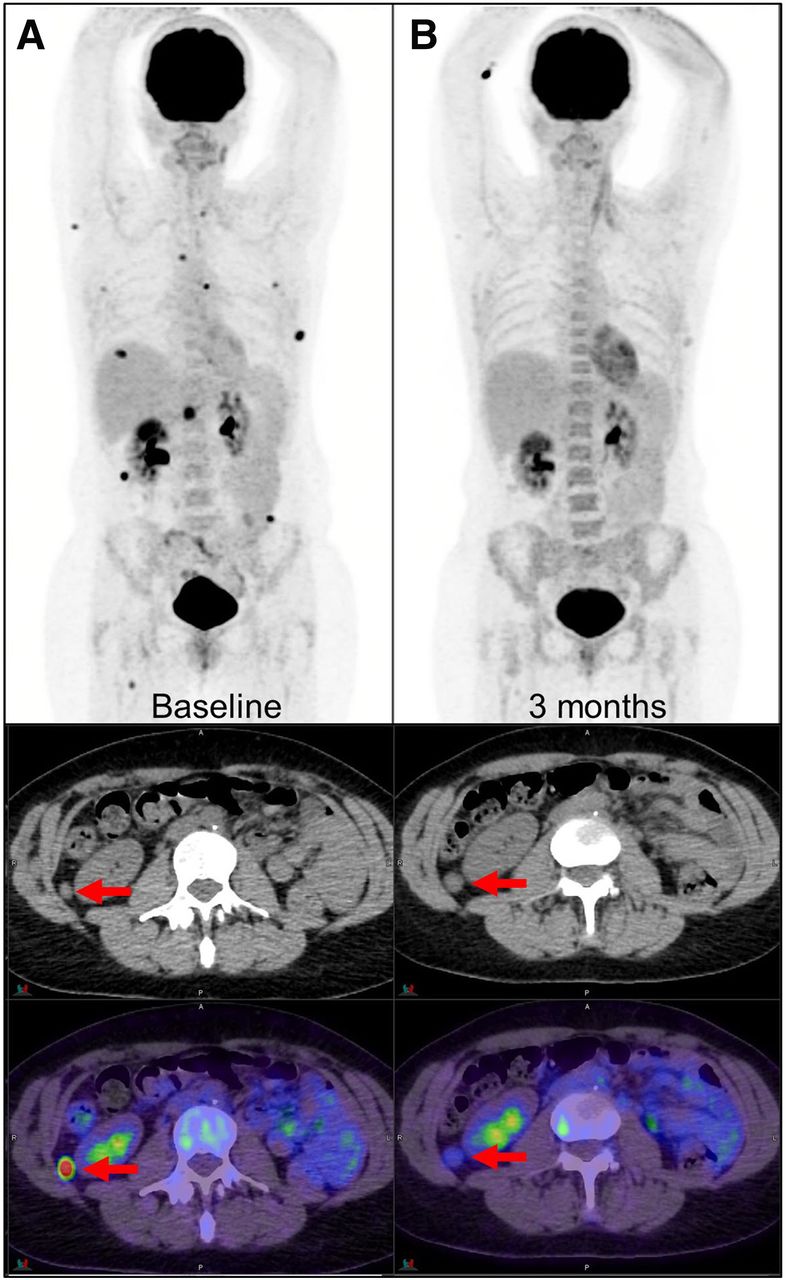
Metabolic response with residual morphologic lesion (arrows) as seen on PET (top), CT (middle), and PET/CT (bottom) images. (A) Metastatic melanoma at baseline shows multiple 18F-FDG–avid metastases. (B) At 3 mo after treatment with 4 cycles of immunotherapy, marked metabolic response is seen on PET, but residual soft-tissue lesions persist on CT (arrows). Diffuse bone marrow 18F-FDG uptake on posttreatment scan is suggestive of systemic immune response.
Evaluation of Possible Hyperprogression
A paradoxic acceleration in tumor growth seems to occur in a subset of patients after the commencement of immunotherapy. This is known as hyperprogression. All studies reporting hyperprogression have involved anti-PD-1 or anti-PD-L1 therapy, with an observed rate of 4%–29% (25). Although the etiology of this phenomenon is not well understood, a preclinical study implicated the role of reprogramming of tumor-associated macrophages by interaction with anti-PD-1 (27). Currently, there is no unified definition for hyperprogression, and different methodologies for assessing tumor growth rate have been used. These have included changes in the size, volume, tumor growth kinetics, or time to treatment failure (25).
Patients with hyperprogression appear to have a very poor survival compared with patients with progression (28). Early and accurate recognition of hyperprogression is therefore of clinical importance, as there is a narrow window of opportunity to switch to another potentially active treatment or simply to withdraw treatment. In this setting, the potential role of 18F-FDG PET/CT was assessed in 50 patients with NSCLC undergoing anti-PD-1 ICI (29). In that study, hyperprogressive disease was significantly associated with baseline wbMTV. In multivariate analysis, wbMTV was independently a predictor of overall survival. Although this finding requires further validation, an increase in wbMTV seems to be more important than the development of new lesions with a stable or decreasing wbMTV, raising the possibility of pseudoprogression, particularly if the patient’s clinical status is stable or improved.
18F-FDG PET/CT Evaluation of Mixed Response or Oligoprogression on Morphologic Imaging
Mixed or differential responses have been reported in a subset of patients, reflecting a combination of immune response in some lesions and evasion in others (30). This pattern of response is not dissimilar to that previously reported in the context of cytotoxic or targeted therapy (31). Primary refractory disease and secondary resistance in prior responders may reflect different mechanisms of immune evasion (Fig. 3). Possible explanations include upregulation of PD-L1 by genomically unstable cancers through mutations in oncogenes or loss of tumor suppressor genes, hence inhibiting T-cell effector functions (32). In the setting of NSCLC treated with anti-PD-1 or anti-PD-L1, the rate of dissociated response was approximately 8%, with some demonstrating a better outcome than in patients with progression (30). Limited available data in this context may be due to difficulty in recognizing this phenomenon by conventional RECIST assessment. 18F-FDG PET/CT may have a potential advantage in this setting by being able to delineate persisting metabolic activity within residual anatomic abnormalities on CT in the context of metabolic response at other disease sites, particularly if amenable to local salvage treatments.

Primary oligoprogression: metastatic melanoma with dissociated response 3 mo after treatment with pembrolizumab demonstrating regression of some sites (solid arrows) and progression of other sites (arrowheads); at 6 mo, solitary hepatic metastasis continued to progress (dashed arrows). Secondary progression: metastatic melanoma with complete response at 5 mo after combination ipilimumab and nivolumab with subsequent secondary progression in solitary left adrenal metastasis (arrow); patient underwent adrenalectomy and continued single-agent nivolumab.
Role of Semiquantitative 18F-FDG PET/CT Parameters
In the context of cytotoxic treatment for several advanced malignancies, metabolic parameters derived from 18F-FDG PET/CT such as wbMTV have been shown to be a strong prognostic factor for patient outcome (33). Despite different mechanisms of action, this concept has also been shown to have prognostic implications in the context of immunotherapy (34,35). In a study of 55 patients with melanoma undergoing anti-PD-1 inhibitor, in multivariate analysis baseline wbMTV on 18F-FDG PET/CT was associated with shorter overall survival (34). Consistent with these findings, in another study the independent prognostic ability of wbTMV was demonstrated in the context of CTLA-4 inhibitor in 142 patients with melanoma (35). These studies have shown wbMTV to be a promising prognostic biomarker that may improve pretreatment risk stratification. However, some challenges need to be addressed, such as consistent methodology, availability of software programs capable of tumor contouring, and validated thresholds for high versus low tumor burden. Increasing availability and ongoing software improvement allow semiautomatic tumor segmentation in a more timely and consistent manner. These advances will, in turn, facilitate further verification of these findings in a larger cohort of patients.
MONITORING OF SYSTEMIC IMMUNE RESPONSE
The initial expansion and recruitment of cytotoxic T lymphocytes after checkpoint inhibition occur in the lymph nodes and may manifest as new 18F-FDG–avid lymph nodes systemically or in the immediate draining nodal stations (36). In the setting of ipilimumab for melanoma, all patients with new mediastinal or hilar nodal uptake on 18F-FDG PET/CT (sarcoidlike lymphadenopathy) demonstrated apparent clinical benefit from treatment (Fig. 4) (37). Dynamic changes in the composition of immune cells in the spleen and bone marrow can also be seen in preclinical and clinical studies, which have translated to the enhanced metabolic activity of the bone marrow on 18F-FDG PET/CT (38). These changes can be observed before or after the treatment and may help predict the favorable or lack of response to ICIs (38). For instance, the baseline increase in bone marrow metabolism on 18F-FDG PET/CT has been independently associated with shorter overall survival in the setting of melanoma (34). Interestingly, in this study increased bone marrow metabolism was associated with transcriptomic profiles, including regulatory T-cell markers. Further translational and clinical studies are required to explore the applicability of these findings in the clinical settings.
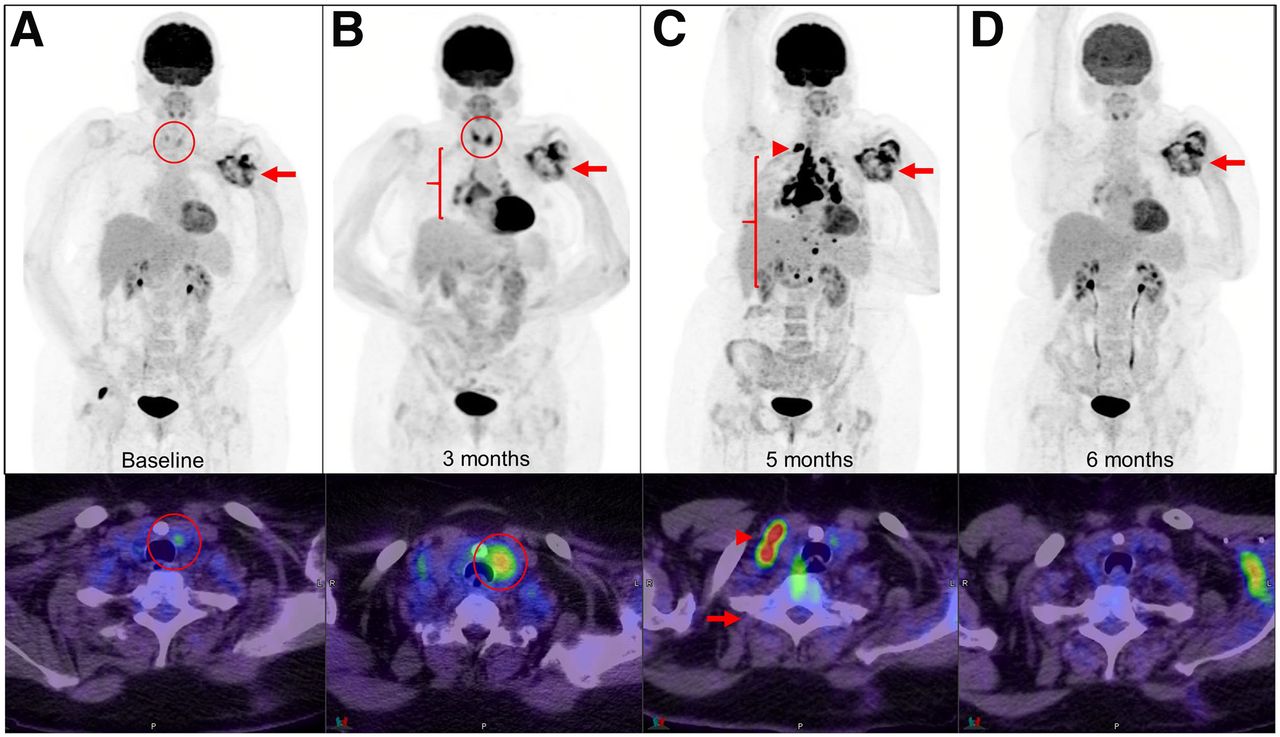
Sarcoidosis with widespread lymphadenopathy. Metastatic squamous cell carcinoma was treated with pembrolizumab, with stable disease in left axillary region (arrows). At 3 mo, sarcoidlike lymphadenopathy in chest was noticed (B, bracket). This finding progressed at 5 mo, with right supraclavicular (C, arrowhead) and upper abdominal nodal involvement. After short course of corticosteroids, sarcoidosis resolved completely. Underlying mild thyroiditis became exacerbated at 3 mo (circled).
Immunotherapeutic strategies can disrupt the immunologic homeostasis in normal organs and lead to inflammatory side effects, which are often termed irAE. Although irAE may involve any organ in the body, the distinct functions of available immunotherapies are reflected in a differing side effect profile (39). For instance, colitis and hypophysitis are more common with anti-CTLA-4 therapy, whereas pneumonitis and thyroiditis appear to be more common with anti-PD-1 agents, and their combination leads to an even higher rate and earlier presentation of these events (39). In fact, the rate of significant irAEs may reach the rate of patients who demonstrate an objective response to combination ICIs and may cause significant or prolonged organ dysfunction, as well as death (40). In the absence of gold-standard tests for some of these events, screening may require a multimodality approach incorporating clinical, biochemical, histopathologic, and imaging surveillance.
The underlying pathophysiologic explanations of irAEs appear to be organ-specific (39) but mostly involve immune-mediated T-cell activation and infiltration (40), providing an opportunity for 18F-FDG PET/CT or cell-specific lineage markers (e.g., anti-CD8 imaging agent) for detection even before clinical presentation. However, the utility of molecular imaging, especially 18F-FDG PET/CT, in the screening and surveillance of irAEs remains largely underappreciated, possibly because of the paucity of systematic studies investigating the performance characteristics of 18F-FDG PET/CT in this setting (41–43). There is a clear need for further studies to confirm the potential utility of this modality, with correlation with the timing, clinical presentation, and severity of these inflammatory events.
CONCLUDING REMARKS AND FUTURE DIRECTIONS
Thanks to the widespread availability of 18F-FDG PET/CT, there is an increasing number of studies assessing the utility of this modality in the monitoring of tumor response, and these studies have also provided an opportunity to surveil global immune activation and its impact on nontumor sites. These studies have sought to address the challenges faced by morphologic imaging but have also unveiled further obstacles to reach an ideal methodology for accurate response monitoring. There remains uncertainty about the optimal timing of response assessment with 18F-FDG PET/CT, the impact of different types of immunotherapy and tumor types, how to handle the development of new lesions, and what parameters should be included in interpretation. Nevertheless, in pursuit of ideal criteria, all principles learned from large-scale clinical trials and evolving experience with 18F-FDG PET/CT need to be thoughtfully contemplated. 18F-FDG PET/CT remains the most commonly used molecular imaging modality in clinical practice and is well poised to become integral in the immunotherapy paradigm by allowing early detection of treatment failure, temporal changes in tumor burden in its entirety and immune-related inflammatory disease, while minimizing the possibility of discarding an otherwise useful treatment too early.
Although 18F-FDG avidity is generally an excellent integrator of the disparate factors that contribute to adverse tumor biology, including proliferation, hypoxia, and inflammation, as shown by the phenomenon of pseudoprogression, immune infiltration and activation are factors that may be precursors of favorable outcomes despite increased 18F-FDG avidity in tumor sites. Accordingly, the ability to image specific components of the immune system may provide vital information on this complex and dynamic process. Much preclinical development work has been done in developing tracers that leverage the unique biology of immune response components. The immense toolbox of agents that could potentially be used to select and monitor immunotherapy has recently been reviewed in detail elsewhere (44). In a companion review, we will discuss agents that are either entering clinical trials or offer immediate promise for selecting or monitoring immunotherapy as a complement to 18F-FDG PET/CT, and we will propose an algorithm for integrating these into clinical practice.
Footnotes
Published online May 22, 2020.
Learning Objectives: On successful completion of this activity, participants should be able (1) to describe the importance of molecular imaging as a noninvasive method for monitoring of the tumor and systemic immune response to immunotherapy; (2) to recognize and differentiate the various conventional and unconventional patterns of tumor response to immune checkpoint inhibitors on 18F-FDG PET; and (3) to develop a framework for more accurate interpretation of 18F-FDG PET studies under immunotherapeutic strategies.
Financial Disclosure: The authors of this article have indicated no relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through July 2023.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication January 4, 2020.
- Accepted for publication May 14, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}