


Article Figures & Data
Figures
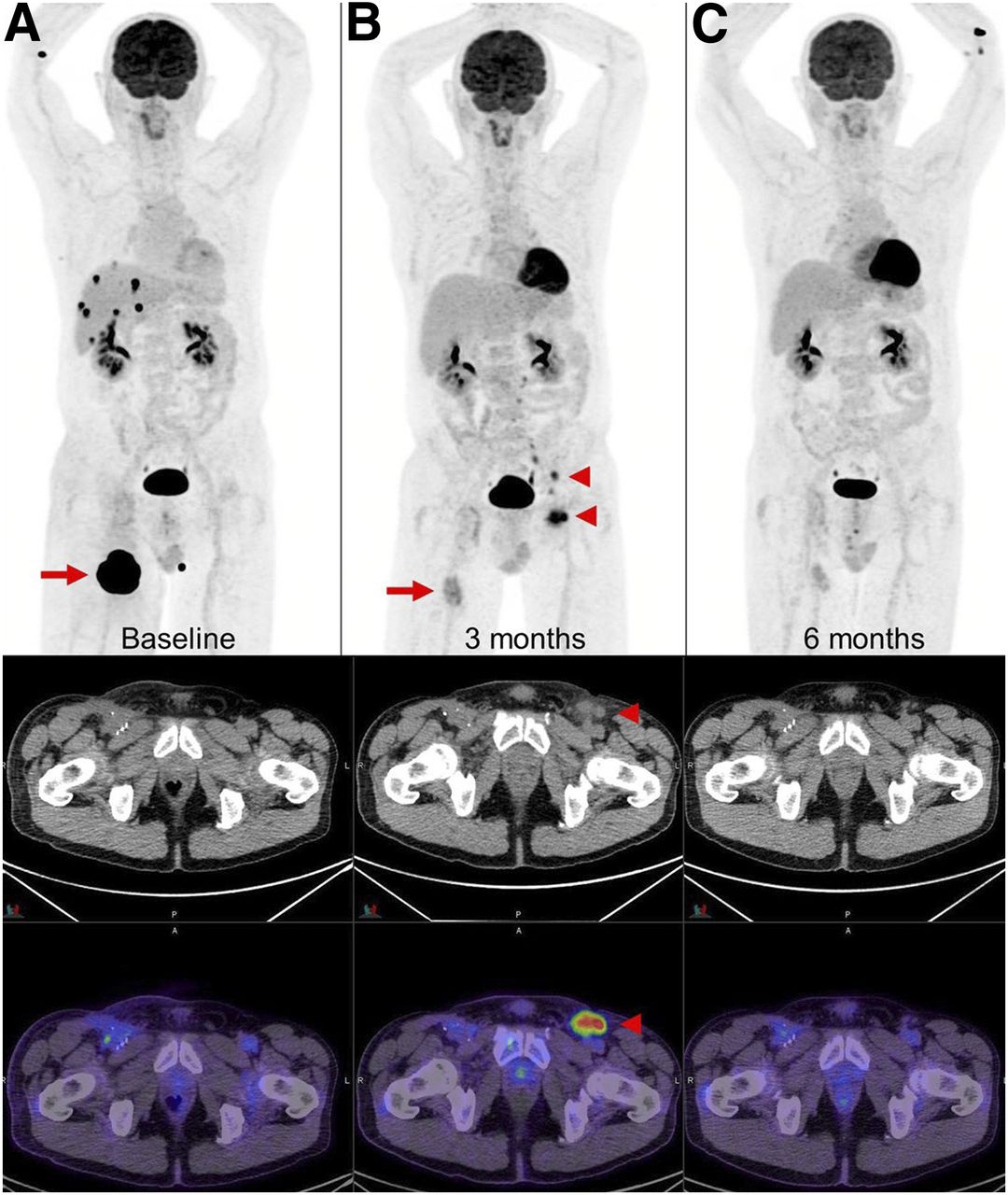
- FIGURE 1.
New lymph nodes in draining basin of regressing metastasis. (A and B) Metastatic melanoma (A, arrow) after 4 cycles of combination ipilimumab and nivolumab demonstrated marked regression of right thigh lesion and complete metabolic response of multiple liver and adrenal metastases (B, arrow); however, new 18F-FDG–avid lymph nodes were noted in left inguinal and iliac regions (B, arrowheads). (C) Biopsy of these lymph nodes showed reactive T cells that resolved on subsequent scan. Transient appearance of reactive lymph nodes contralateral to responding right thigh lesion was attributed to likely aberrant nodal drainage to contralateral nodes due to prior ipsilateral inguinal dissection. Immune-PET targeting CD8+ T cells, such as 18F-Ara-G/granzyme B, may allow noninvasive characterization of some cases with suspected pseudoprogression.
- FIGURE 2.
Hyperprogression vs. pseudoprogression. (A and B) Patient with metastatic melanoma at baseline (A, arrows) and 2 mo after start of combination ipilimumab and nivolumab demonstrates marked progression of liver metastasis (B, arrows). (C) As patient was clinically well, immunotherapy was continued, and further follow-up at 4 mo showed marked improvement of liver lesion (arrows). Immune-PET targeting CD8+ T cells, such as 18F-Ara-G/granzyme B, may allow pseudoprogression to be distinguished from hyperprogression in challenging cases.
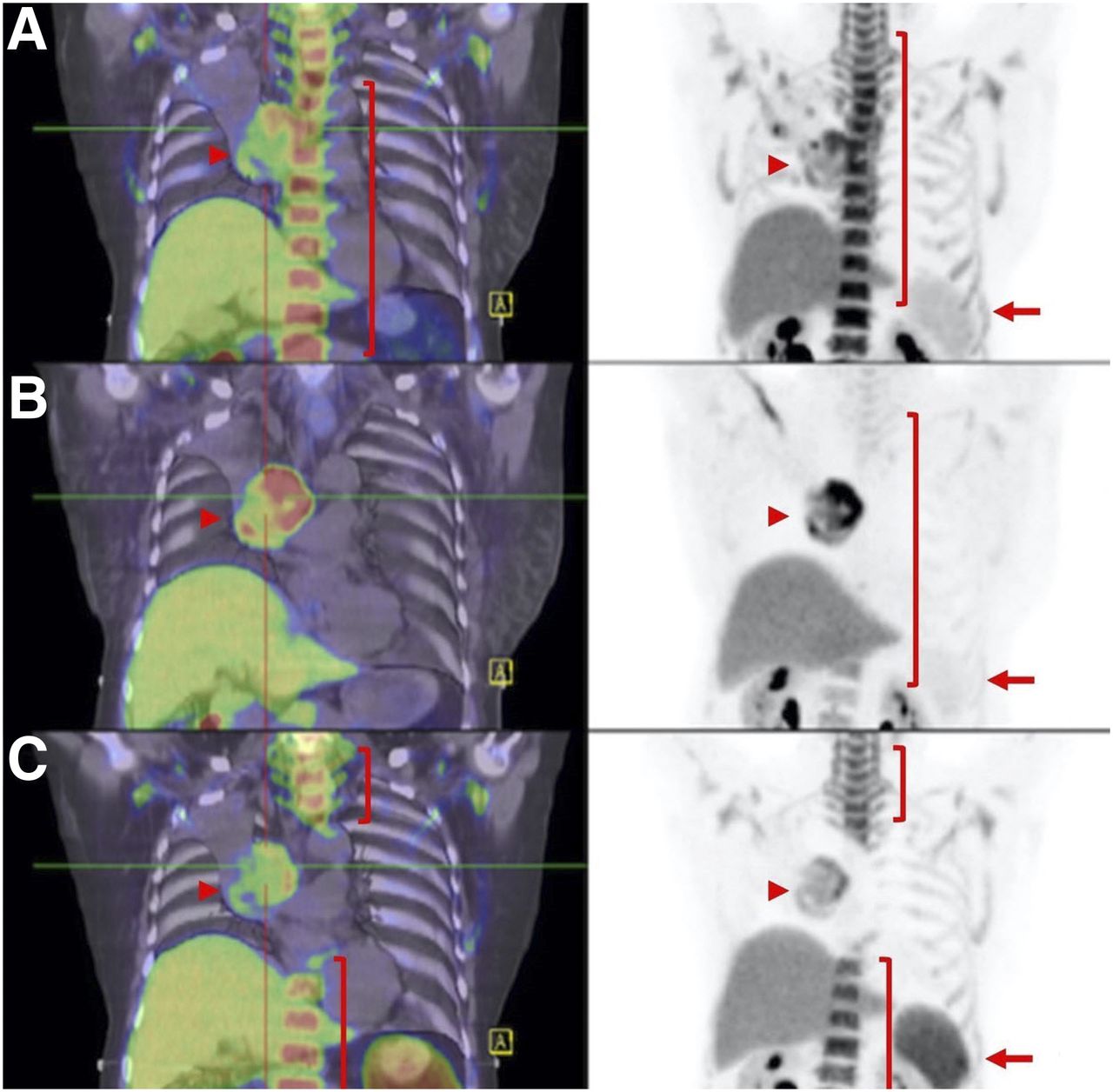
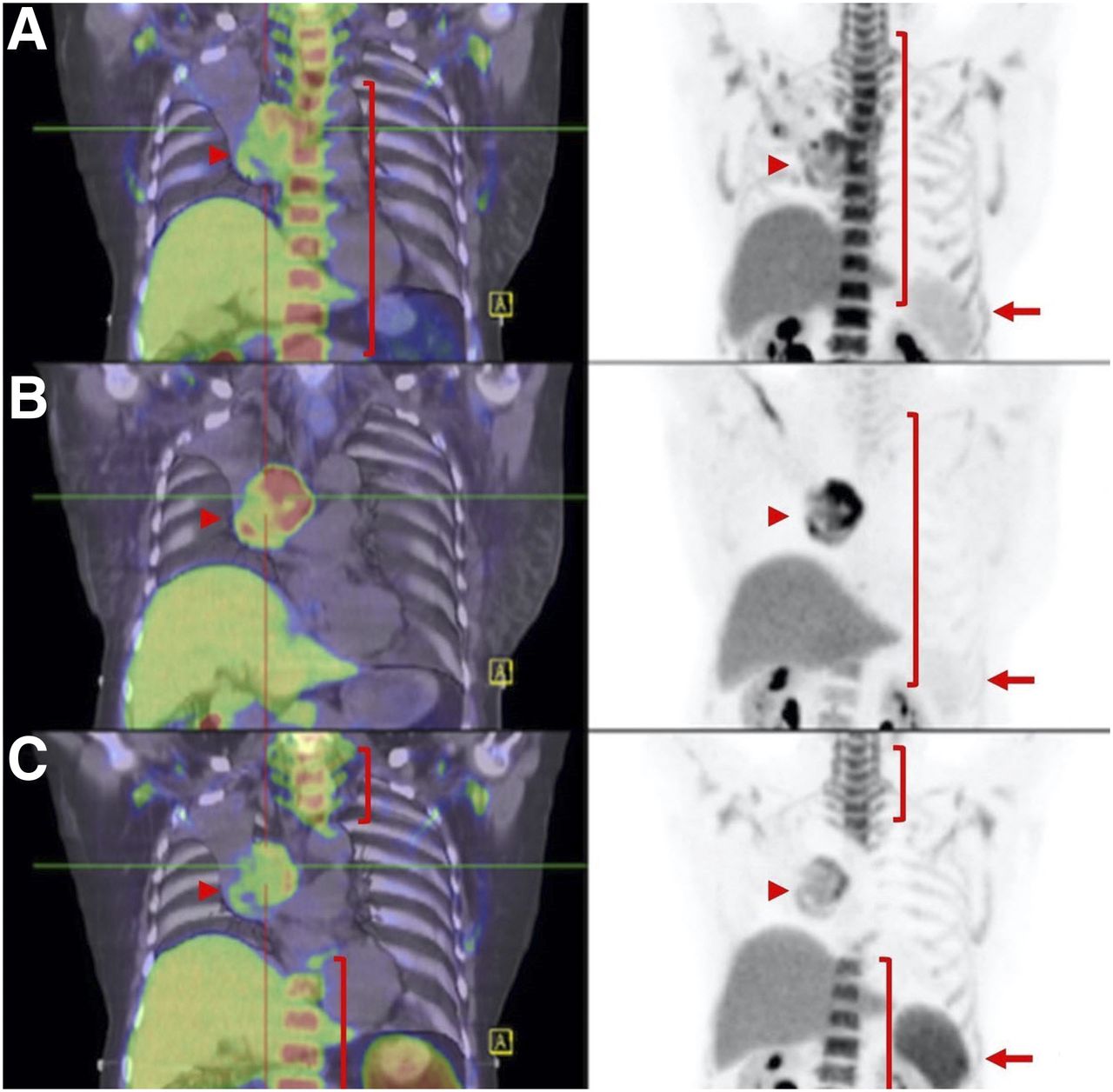
- FIGURE 3.
Serial imaging with 3′-18F-fluoro-3′-deoxythymidine PET/CT of non–small cell lung cancer before and after chemoradiotherapy. (A) At baseline, there is low uptake in spleen (arrow), which is primarily a repository of immune cells, but high uptake in proliferating bone marrow (bracket), as well as in tumor in right hilum (arrowhead). (B) Early in treatment, reduction in bone marrow activity is observed (bracket), particularly within radiation treatment volume, but persistence of low uptake in spleen (arrow) and higher uptake in tumor (arrowhead). (C) At 3 mo after radiotherapy, there has been recovery in marrow proliferation beyond high-dose radiation field (brackets) but development of increased uptake in spleen (arrow) and lower uptake in tumor (arrowhead). This potentially reflects proliferation of immune cells representing immune response to release of tumor-associated antigens.
- FIGURE 4.
Speculative diagnostic algorithm using PET agents to interrogate immune therapy. Through combination of baseline 18F-FDG PET/CT and biopsy, prognostic factors for response to ICIs, including whole-body metabolic tumor volume and TILs, could be assessed. For disease with low or absent TILs on biopsy, imaging with CD8+ agents could provide baseline for assessment of interventions to enhance immune cell infiltration, particularly including anti-CTLA-4 therapy or use of radiotherapy to induce T-cell priming by release of tumor-associated antigens. For those with high TILs, radiolabeled anti-PD-1/PD-L1 or 18F-adnectin PD-L1 agents could be used to select patients for ICI monotherapy against these targets. Early (6–8 wk) during given therapy, 18F-FDG PET/CT could be repeated. Conventional 18F-FDG PET/CT response would enable ongoing treatment, whereas increase in 18F-FDG uptake or development of new lesions could be further assessed by 18F-Ara-G or granzyme B imaging to detect T-cell activation as manifestation of pseudoprogression. Although not shown in this algorithm, 3′-18F-fluoro-3′-deoxythymidine PET/CT may also be helpful for demonstrating enhanced proliferation in tumor in case of hyperprogression or draining nodes and spleen in case of pseudoprogression. In patients receiving anti-CTLA-4 monotherapy agents but not responding on 18F-FDG PET/CT, reimaging with CD8+ T-cell agents to confirm efficacy of T-cell recruitment or empiric addition of anti-PD-1/PD-L1 agents may be appropriate, whereas for patients already on such treatment, withdrawal of treatment might be contemplated. Therapeutic agents that target immunosuppressive factors might also be considered in such cases. CMR = complete metabolic response; PMD = progressive metabolic disease; PMR = partial metabolic response; SMD = stable metabolic disease; wbMTV = whole-body metabolic tumor volume.


Tables
- TABLE 1
Learning Points and Speculation on Future Directions for Imaging Immune System with 18F-FDG and New Tracers
Point Description 1 Type of ICI may impact rate of pseudoprogression, with lower rate reported in anti-PD-1/PD-L1 than in anti-CTLA-4 2 Rate of pseudoprogression may differ depending on tumor type, with highest rate reported in melanoma, which also has one of highest response rates 3 Early after commencement of ICIs, change in metabolic parameters on 18F-FDG PET/CT may further predict response in patients with stable morphologic imaging 4 Although pseudoprogression most commonly occurs within 12 wk of starting ICIs, about of one third happen beyond 12 wk; therefore, timing of first follow-up scan may be important 5 Early and marked metabolic response with or without morphologic response commonly indicates durable response 6 18F-FDG PET/CT performed for response monitoring should also be thoroughly interrogated for manifestations of immune-related adverse events 7 It appears that number and size of new lesions on 18F-FDG PET/CT are important factors in differentiating true progression from pseudoprogression 8 Whole-body metabolic tumor volume on 18F-FDG PET/CT is promising metabolic parameter at baseline or during treatment. At baseline, high whole-body metabolic tumor volume is associated with hyperprogressive disease and may be predictive of adverse overall survival 9 18F-FDG PET/CT may have role in further risk stratification of patients who achieve partial response on morphologic imaging, hence guiding length of immunotherapy 10 18F-FDG PET/CT may have role in patients with dissociated or mixed response on morphologic imaging, to guide local treatment to limited sites of progressive disease while continuing immunotherapy 11a Decision to continue immunotherapy beyond progression on either morphologic or 18F-FDG PET/CT criteria should be made with caution and considered in selected patients who do not experience severe toxicity from these agents and whose disease-related symptoms have improved or stabilized on treatment 11b If immunotherapy is continued or there is any doubt about imaging findings, to differentiate pseudoprogression from true progression biopsy or confirmatory scan at short interval (4 wk) may be helpful or, immune-PET targeting activated CD8+ T cells, such as 18F-Ara-G or 68Ga-granzyme B can be considered; 3′-18F-fluoro-3′-deoxythymidine PET/CT may have a role in differentiating pseudoprogression from hyperprogression. 13 Immune-PET targeting CD8+ T cells may distinguish immune-desert from immune-inflamed tumors, whereby allowing rational selection of ICIs or combination ICIs 14 18F-Ara-G and 68Ga-granzyme are promising tracers that can differentiate activated CD8+ T cells from exhausted CD8+ T cells 15 After pharmacologic intervention or radiotherapy, serial immune-PET targeting CD8+ T cells, including 18F-Ara-G or 68Ga-granzyme, may allow monitoring of T-cell trafficking within tumor sites 16 Radiolabeled tracers targeting PD1/PD-L1 can demonstrate inter- and intrapatient heterogeneity of these immune checkpoints and can potentially be predictive of response to ICIs but are subject to inherent limitation of PD1/PD-L1 as predictive biomarkers





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Approaches to Imaging Immune Activation Using PET
- Preclinical Evaluation and Pilot Clinical Study of CD137 PET Radiotracer for Noninvasive Monitoring Early Responses of Immunotherapy
- ICAM-1 orchestrates the abscopal effect of tumor radiotherapy
- FAPI PET/CT: Will It End the Hegemony of 18F-FDG in Oncology?