


Abstract
18F-FDG–avid thyroid incidentaloma (TI) is seen in approximately 2.5% of patients imaged for staging or response assessment of malignancy and represents thyroid cancer in approximately 35% of cases. Consequently, the 2015 American Thyroid Association guidelines strongly recommend investigation of all 18F-FDG–avid nodules 1 cm or larger with ultrasound and fine-needle aspiration cytology (FNA). This study aimed to assess the overall and thyroid cancer–specific survival in a large cohort of patients with 18F-FDG–avid TI with long-term follow-up to assess the validity of this approach. Methods: Retrospective review of 45,680 PET/CT scans performed at a comprehensive cancer center from January 2007 to January 2015 identified 2,588 18F-FDG PET/CT reports referring to the thyroid. After exclusion of nonavid thyroid nodules, diffuse 18F-FDG uptake, known thyroid cancer, abnormalities adjacent to the thyroid, and repeat studies, 500 patients (1.1%) with TI were identified, of whom 362 had confirmed death or more than 12 mo of clinical follow-up. Variables including age, sex, primary malignancy, overall survival, thyroid cancer–specific survival, FNA, and histopathology were collected until January 2016. Multivariate logistic regression and survival analysis were performed. Results: The 362 analyzed patients (65% female) had a median age of 65 y (range, 19–96 y) and follow-up of 24 mo (range, 1–103 mo). Lymphoid, lung, and colorectal malignancy were the most common staging indications. Median overall survival was 20 mo (interquartile range, 9.5–39 mo). Most of the 180 observed deaths were due to the primary malignancy under investigation (92.2%) or to causes not related to cancer (7.2%); one patient (0.6%) died from incidentally detected medullary thyroid cancer. 18F-FDG avidity in the index malignancy, an advanced stage for that malignancy, and a clinician decision not to investigate 18F-FDG–avid TI were all predictors of mortality, with hazard ratios of 8.5, 3.0, and 3.3, respectively, and 95% confidence intervals of 4.6–15.8, 2.3–3.9, and 2.0–5.0, respectively (P < 0.001). Of 131 patients suitable for cytologic or histopathologic evaluation, 47 (36%) had incidental thyroid cancer (24 papillary, 11 malignant FNA, 5 oncocytic/Hürthle cell, 2 medullary, 1 follicular, and 4 metastases from underlying malignancy). Conclusion: Overall survival with 18F-FDG–avid TI was poor because of the prognosis associated with underlying malignancy, which must be considered before investigation of 18F-FDG–avid TI and certainly before aggressive treatment. Active surveillance should be considered in this group of patients.
PET/CT with 18F-FDG is an accurate functional imaging technique increasingly used in diagnosing, staging, and monitoring the treatment of many common malignancies. The enhanced uptake of glucose (or its analog 18F-FDG) by cancer cells due to inefficient aerobic glycolysis—termed the Warburg effect (1)—is the hallmark of in vivo cancer imaging with 18F-FDG PET/CT. However, incidental foci of 18F-FDG uptake unrelated to the primary malignancy pose a significant problem for the reporting nuclear medicine specialist, treating physician, and surgeon. Our department has previously analyzed the outcomes of incidental nonthyroidal 18F-FDG uptake and shown that most can be appropriately categorized as benign or of unlikely clinical significance by experienced PET readers, thereby avoiding the costs, anxiety, and potential complications of unnecessary investigation (2). However, 18F-FDG–avid thyroid incidentaloma (TI)—defined as abnormal focal 18F-FDG uptake confined to the thyroid gland—is a relatively common finding (2.5%), and a large metaanalysis confirmed that this represents thyroid cancer in approximately 35% of investigated cases (3). Consequently, the 2015 American Thyroid Association guidelines (4) strongly recommend investigation of such nodules, when 1 cm or larger, with thyroid ultrasound and fine-needle aspiration cytology (FNA) without consideration of the prognosis of the underlying malignancy.
Nevertheless, the overall outcome of most oncology patients with 18F-FDG–avid TI is likely determined by the underlying malignancy, given the excellent prognosis associated with thyroid cancer, especially that detected incidentally on imaging. Therefore, the costs, anxiety, and risks associated with investigation and surgical management of incidental 18F-FDG–avid thyroid cancer need to be carefully balanced. The relative clinical impact of an incidental, asymptomatic thyroid cancer in the context of active nonthyroidal malignancy is unknown but critically important information to guide the interpretation and management of this finding.
Our study aimed to assess the clinically relevant outcomes of overall and thyroid cancer–specific survival, and the risks of recurrent or metastatic thyroid cancer, in a large cohort of patients with 18F-FDG–avid TI—irrespective of investigation status—managed at a comprehensive cancer center with long-term follow-up. Secondary outcomes included determining predictors of mortality and the incidence of malignant, benign, Hürthle cell, and metastatic disease within 18F-FDG–avid incidental thyroid nodules in this cohort.
MATERIALS AND METHODS
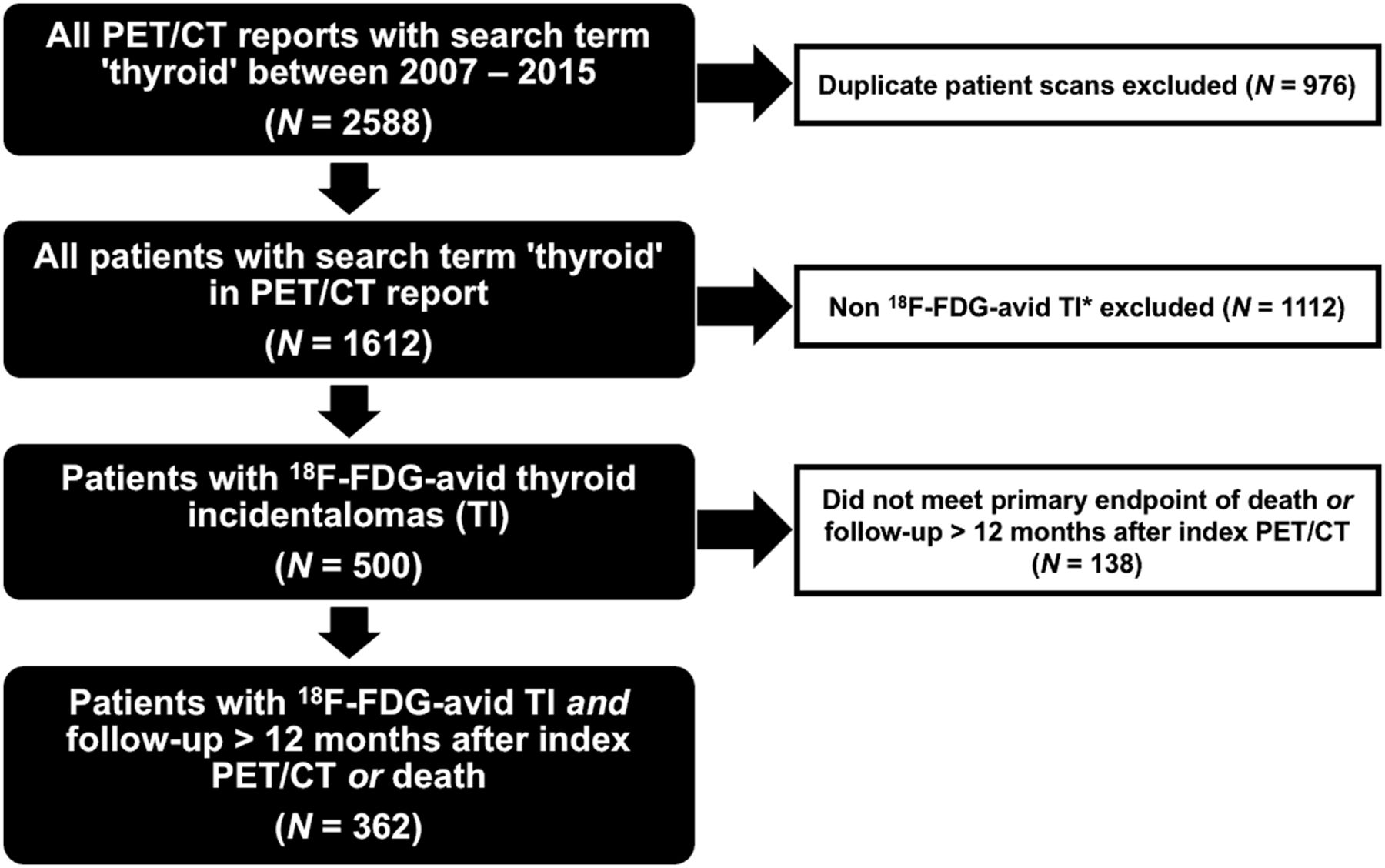
This study involved retrospective review of 45,680 consecutive PET/CT scans performed at a single comprehensive cancer center from January 2007 to January 2015 for the purpose of diagnosis, staging, or treatment-response evaluation in relation to the patient’s known or suspected malignancy. The institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived. A key word search of the departmental database identified 2,588 PET/CT reports referring to the thyroid and 1,612 patients after exclusion of duplicate and follow-up PET/CT reports. Five hundred patients with TI were identified for survival analysis and histopathologic/cytologic outcome after exclusion of nonavid thyroid nodules, diffuse 18F-FDG uptake, known thyroid cancer, abnormalities adjacent to the thyroid, and use of non–18F-FDG radiotracers (68Ga-prostate-specific membrane antigen, 68Ga-DOTATATE) based on review of electronic medical records. Ninety-six (19.2%) of these cases were referred to our center only for PET imaging and thus did not have available clinical follow-up data, and 42 (8.4%) cases were lost to clinical follow-up. Until data cutoff in January 2016, 362 patients had follow-up data to death or for more than 12 mo—necessary to capture a rapidly progressive poorly differentiated or anaplastic carcinoma, which would be expected to become clinically apparent during this period—and were included in the analysis (Fig. 1). The variables that were collected included primary malignancy type and stage according to the seventh edition of the AJCC Cancer Staging Manual (5), 18F-FDG avidity within the primary malignancy on index PET/CT (i.e., the first scan to identify an 18F-FDG–avid TI), extent of thyroid investigation (histologic or cytologic), overall survival, thyroid cancer–specific survival, and structural incomplete response of thyroid cancer. The etiology of investigated 18F-FDG–avid TI was classified according to histopathologic diagnosis (including the presence and size of vascular invasion) and the result of FNA according to the Bethesda classification (6) was used when histopathologic diagnosis was not obtained.
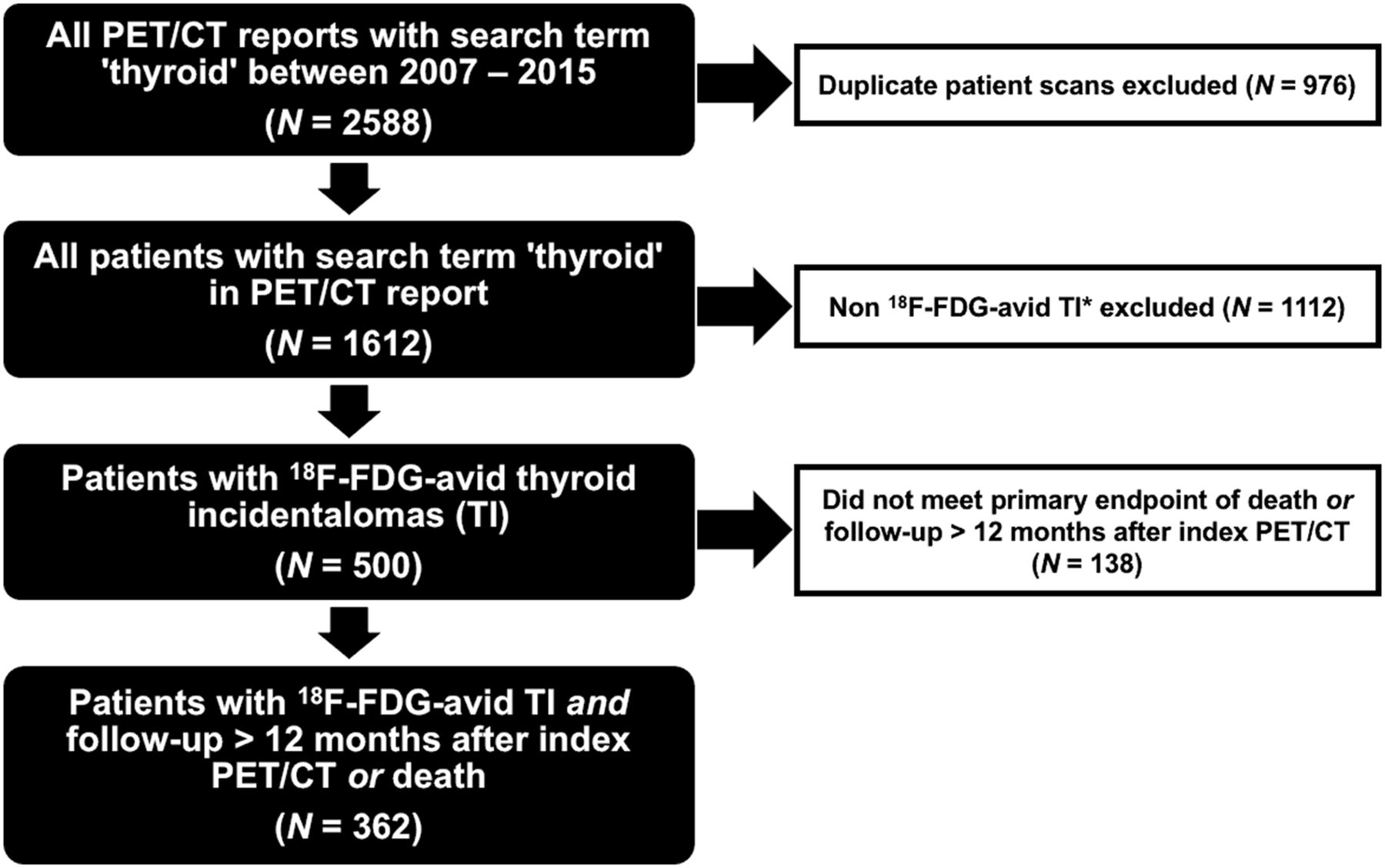
Consort flow diagram demonstrating identification and selection of study population. *Non–18F-FDG–avid TIs comprise nonavid thyroid nodules, diffuse thyroid 18F-FDG uptake, patients with known thyroid cancer, abnormalities adjacent to thyroid (parathyroid adenomas and lymphadenopathy), and use of non–18F-FDG radiotracers (68Ga-prostate-specific membrane antigen, 68Ga-DOTATATE).
Univariate analysis using simple logistic regression was performed to assess for any associations between mortality (dependent variable) and multivariate predictors (independent variables, including presence of 18F-FDG avidity in nonthyroidal malignancy, American Joint Committee on Cancer tumor stage, TI investigation status, nonthyroidal malignancy type, age, and sex). Factors found to be significant were included in the multivariate logistic regression model to determine whether they still predicted patient death. The Kaplan–Meier curve was used to assess the individual impact of each predictor on survival time. Crude and adjusted odds ratios were calculated. Statistical analysis was performed using Stata12 (Stata Corp.). A P value of less than 0.05 was considered statistically significant.
RESULTS
In total, 362 patients (35% male and 65% female) met the inclusion criteria to assess the primary outcome of overall and thyroid cancer–specific survival, with a median age of 65 y (range, 19–96 y) and median follow-up of 24 mo (interquartile range, 13–46 mo). The index PET/CT study of 272 (75%) patients demonstrated 18F-FDG avidity associated with the underlying nonthyroidal malignancy, indicating the presence of persistent metabolically active disease. Lymphoid malignancy (19%), lung malignancy (16%), colorectal malignancy (12%), and melanoma (9%) were the most common diagnostic and staging indications (Table 1). Of 4 cases of carcinoma of unknown primary (1.5%), 2 18F-FDG–avid TIs were confirmed papillary thyroid microcarcinoma, and the PET/CT appearance of the remaining 2 was inconsistent with anaplastic thyroid carcinoma. The median overall survival from the primary malignancy was 20 mo (interquartile range, 9.5–39 mo). Overall, 180 patients (50%) died, and most of these (166 [92%]) were positive for 18F-FDG avidity on the index PET/CT scan (Table 2). Most deaths were due to the primary malignancy under investigation (166 [92.2%]) or other non–cancer-related causes (13 [7.2%]). One patient (0.6%) died from the incidentally detected medullary thyroid cancer (Fig. 2).
Baseline Demographic and Clinical Data of Study Population (n = 362)
Follow-up and Clinical Outcome Data in Patients with Follow-up > 12 Months or Death (n = 362)
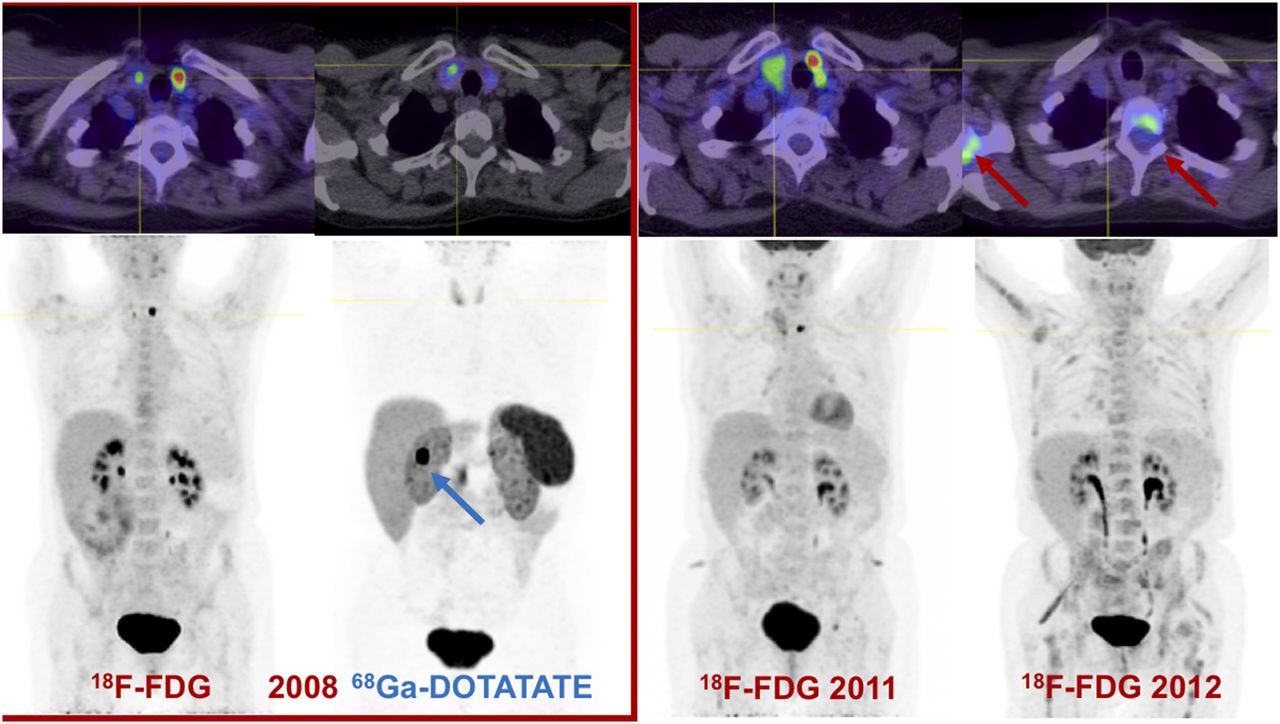
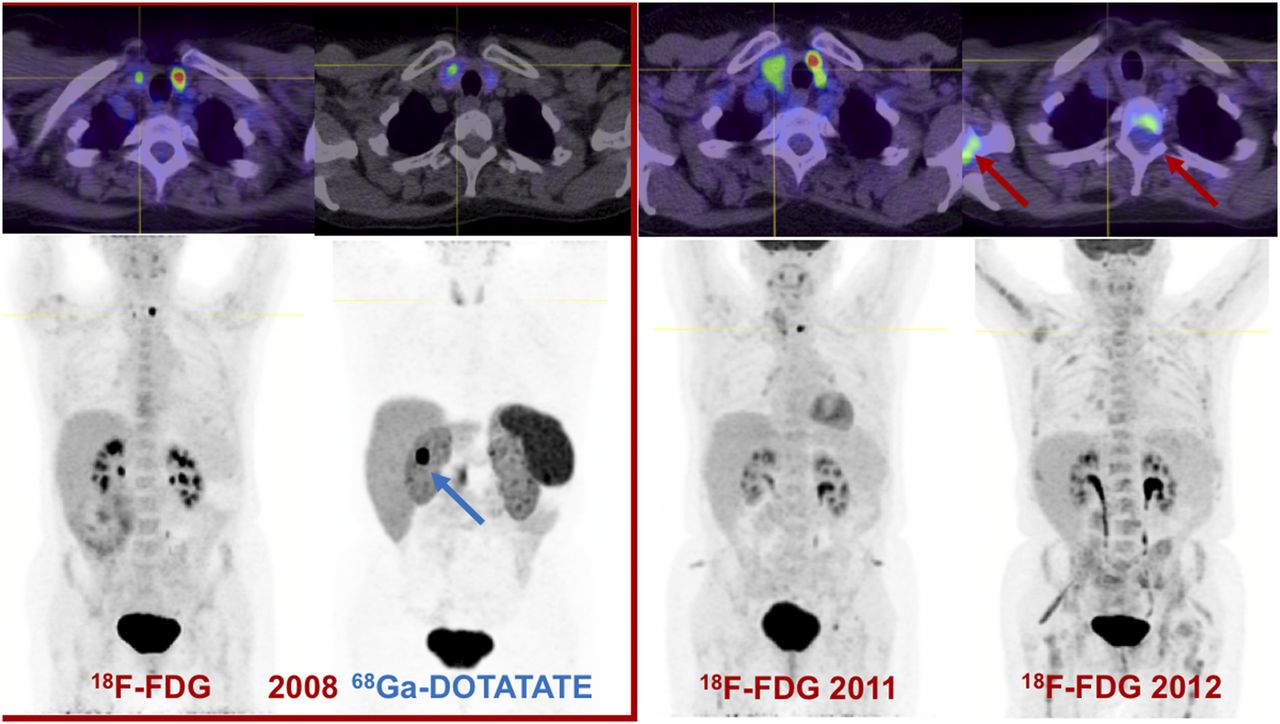
18F-FDG PET/CT performed on 61-y-old woman with metastatic duodenal carcinoid tumor (blue arrow; grade 2, Ki-67 of 15%) showed mildly avid (SUVmax, 4.4) right thyroid nodule and intensely avid (SUVmax, 16) left thyroid nodule. 68Ga-DOTATATE PET/CT revealed concordant mild DOTATATE uptake in right thyroid nodule, and evaluation for medullary thyroid carcinoma was recommended. Subsequent PET-directed biopsy of mildly 18F-FDG/DOTATATE–avid thyroid nodule confirmed progressive medullary thyroid carcinoma with extrathyroidal extension and lymphovascular invasion. Total thyroidectomy confirmed that intensely 18F-FDG–avid left thyroid nodule was benign follicular adenoma. Patient died approximately 18 mo later from progressive metastatic medullary thyroid cancer (red arrows).
18F-FDG avidity, an advanced stage for the known malignancy at the time of the index PET/CT that detected the TI, and a decision by the clinician not to investigate the 18F-FDG–avid TI were statistically significant predictors of mortality, with crude odds ratios of 8.5 (95% confidence interval [95% CI], 4.6–15.8), 3.0 (95% CI, 2.3–3.9), and 3.3 (95% CI, 2.0–5.0), respectively (P < 0.001). These associations persisted when all factors were included in the model, with adjusted odds ratios of 4.0 (95% CI, 2.0–8.2), 2.5 (95% CI, 1.8–3.3), and 1.7 (95% CI, 1.04−3.3), respectively (P < 0.001). The impact of these predictors on survival estimates are graphically demonstrated on Kaplan–Meier survival curves in Figure 3. Lymphoid neoplasm predicted improved survival relative to other malignancies, with crude and adjusted odds ratios of 0.3 (95% CI, 0.1–0.5) and 0.3 (95% CI, 0.2–0.8), respectively (P < 0.001). There was no statistically significant association between survival and other nonthyroidal malignancy types, age, or sex (Table 3).

(A) Kaplan–Meier survival distribution of patients who had 18F-FDG–avid (SUVmax > 3) primary disease at time of identification of 18F-FDG–avid TI on index PET/CT and patients who did not have 18F-FDG–avid primary disease. (B) Kaplan–Meier survival distribution among patients who did not undergo cytologic or histopathologic investigation of 18F-FDG–avid TI and among patients who did undergo further investigation. (C) Kaplan–Meier survival distribution of patients stratified according to American Joint Committee on Cancer stage of primary malignancy. HR = hazard ratio.
Results of Simple and Multivariate Logistic Regression for Death Outcome
The majority (231) of the 362 patients with 18F-FDG–avid TI and adequate clinical follow-up were not investigated at the time of the index PET/CT scan. Of the 131 patients who underwent histologic or cytologic investigation, 47 (36%) had incidental thyroid cancer (24 papillary, 11 malignant on FNA, 5 oncocytic/Hürthle cell, 2 medullary, 1 follicular, and 4 confirmed metastatic from underlying malignancy) (Table 4). At the completion of follow-up, 42 of 43 patients (98%) with confirmed thyroid cancer were either stable under observation or had no clinical evidence of disease recurrence. Seventy-two investigated nodules (55.0%) had benign pathology, and 12 (9.1%) had nondiagnostic or indeterminate FNA without further evaluation. The incidence of 18F-FDG–avid thyroid nodules at our PET center was 1.1% during the 8-y study period.
Pathologic Characteristics of 18F-FDG–Avid TI
DISCUSSION
Our data demonstrated high mortality—median overall survival of 20 mo—in this large cohort of patients with 18F-FDG–avid TI undergoing 18F-FDG PET/CT at a comprehensive cancer center. However, this high mortality appears to be due almost exclusively to the poor prognosis associated with the underlying malignancy rather than to adverse outcomes related to incidentally detected 18F-FDG–avid thyroid cancer. In contrast, the 18F-FDG–avid TI had no discernible clinical impact—excluding that associated with medical investigation and management of this asymptomatic incidental finding—in 361 (99.7%) of 362 patients after a median of 24 mo of follow-up; it is uncertain if earlier intervention would have prevented the single death from incidental medullary thyroid carcinoma. This observation highlights the importance of considering the prognosis of the underlying malignancy when deciding whether further investigation and management are appropriate, as the potential benefits of intervention may not be realized because of the short life expectancy.
Efforts to identify the cohort of patients who will potentially benefit from further evaluation and treatment have not been successful. Most previous studies have focused on guiding the decision to biopsy by using the intensity of focal 18F-FDG uptake to identify the patients at highest risk of thyroid cancer. Although some studies have indicated an SUVmax threshold (7–9), many have found no such association (10–12), and a large metaanalysis by Bertagna et al. (3) confirmed that there is significant overlap of 18F-FDG avidity between benign and malignant lesions, without an SUVmax threshold to guide the decision to biopsy. This finding is consistent with a growing body of literature indicating that the 18F-FDG avidity of TI is often driven by mechanisms other than poorly differentiated malignancy. For example, it is increasingly recognized that oncocytic/Hürthle cell lesions (irrespective of benign or malignant etiology) demonstrate intense 18F-FDG avidity (13) due to an intrinsic mitochondrial defect driving inefficient glycolytic metabolism (14,15). Other causes of very intensely 18F-FDG–avid benign TI include degenerate nodules (16), follicular adenomas, and adenomatous hyperplasia (17). The limitation of this approach is evident from the low 18F-FDG uptake (SUVmax, 4.4) in the only clinically significant thyroid cancer in our study (Fig. 2) compared with the intensely avid benign follicular adenoma in the opposite lobe (SUVmax, 16).
In contrast, our study findings enable identification of those cases with a poor prognosis from underlying malignancy, in which further evaluation is unlikely to be of clinical benefit (Fig. 4), and emphasize the need to consider the broader clinical context. The presence of 18F-FDG avidity within the underlying malignancy conferred a significant crude hazard ratio of 8.5 for mortality (P < 0.001) beyond the overall poor prognosis seen in our entire patient cohort. This finding is consistent with the large body of literature confirming the superior prognostic value of 18F-FDG avidity across a spectrum of malignancies, including non–small cell lung carcinoma (18), gastroenteropancreatic neuroendocrine tumors (19), medullary thyroid carcinoma (20), and established metastatic differentiated thyroid carcinoma (21). This finding suggests that clinicians should take a cautious approach to investigating 18F-FDG–avid TI in the setting of 18F-FDG avidity in a known or suspected malignancy, especially if metastatic, because, unsurprisingly, an advanced tumor stage according to the criteria of the American Joint Committee on Cancer was also a statistically significant prognostic indicator, with a crude hazard ratio of 3.0 (95% CI, 2.3–3.9).
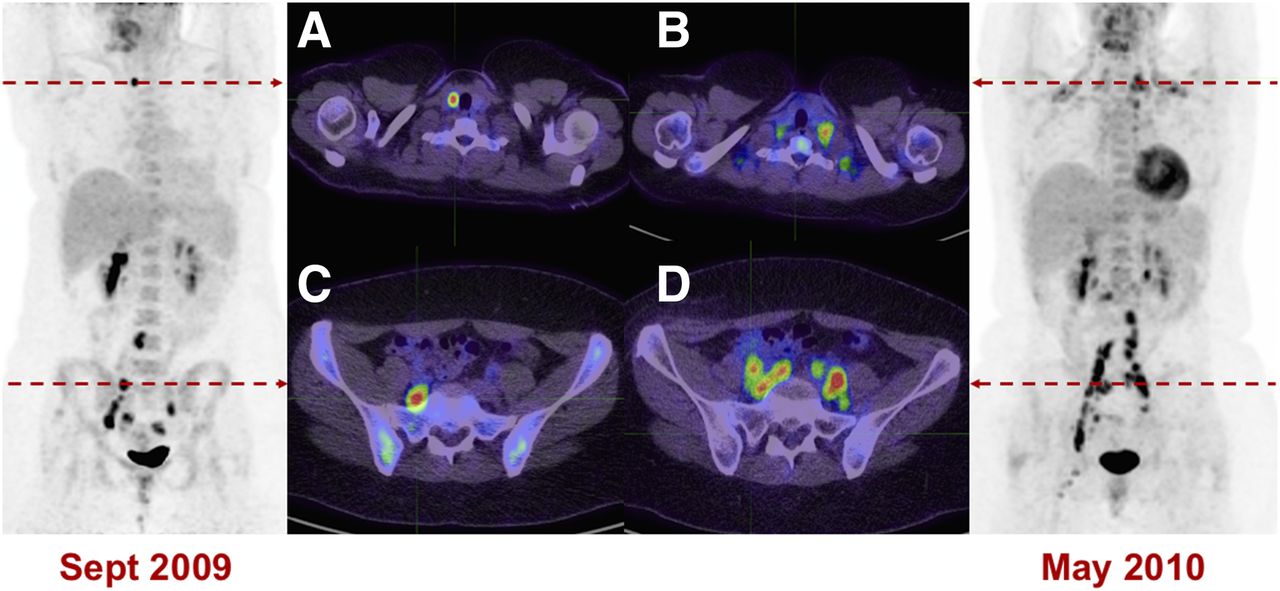
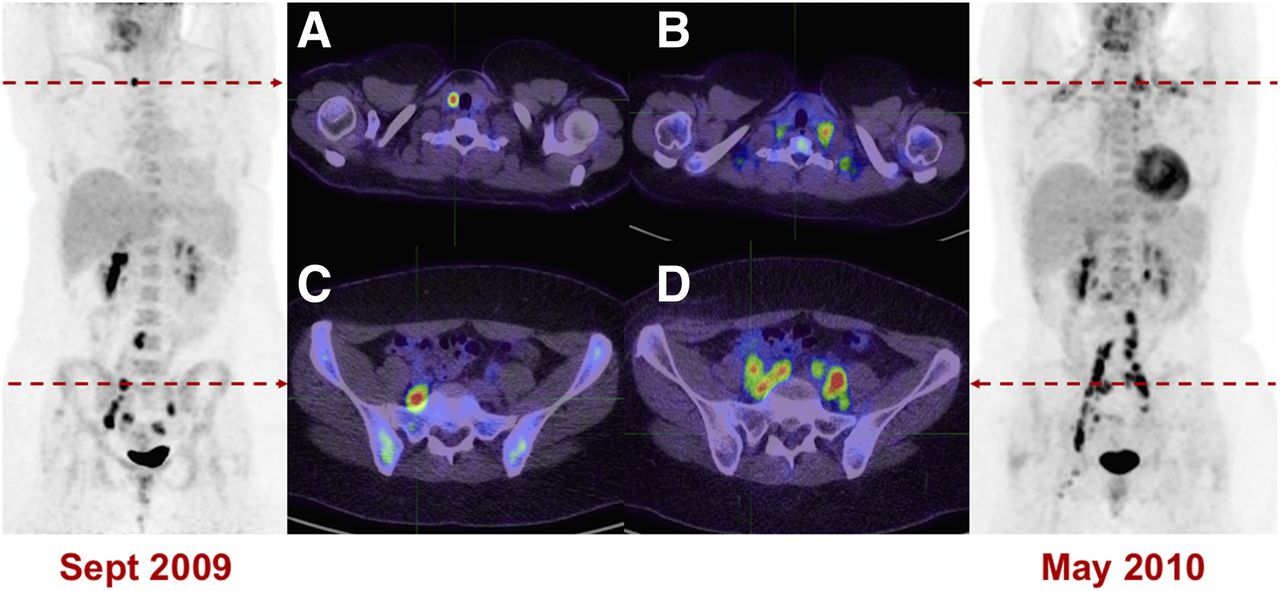
Intensely 18F-FDG–avid TI (SUVmax, 16) was identified on staging 18F-FDG PET/CT scan of 28-y-old woman with stage IIIB poorly differentiated cervical carcinoma and persistent 18F-FDG–avid pelvic nodal disease. Ultrasound-guided cytologic evaluation demonstrated 5-mm papillary thyroid carcinoma with no adverse features, which was treated with total thyroidectomy. (A and B) Baseline 18F-FDG–avid thyroid nodule (A) and subsequent cervical carcinoma metastases to supraclavicular nodes (B). (C and D) Baseline 18F-FDG–avid pelvic lymphadenopathy (C) with subsequent disease progression (D). Patient died 10 mo after baseline PET/CT scan from progression of metastatic poorly differentiated cervical carcinoma.
Although this high prognostic value of 18F-FDG avidity in oncology has contributed to a level of anxiety associated with 18F-FDG–avid TI, the lack of an SUV threshold for these lesions is supported by increasing evidence that 18F-FDG avidity associated with incidentally detected thyroid cancer does not add prognostic value beyond TNM staging (22). A potential explanation for this paradox is that a proportion of incidentally detected apparently 18F-FDG–avid thyroid malignancies actually represent incidental findings in pathology specimens, further supporting a more conservative approach to managing 18F-FDG–avid TI. A careful histopathologic and imaging correlation revealed that 20% (3/15) of presumed 18F-FDG–avid incidental thyroid carcinomas in fact represented incidental malignancies identified by the pathologist and did not correlate with the avid lesion at all (16). This finding is plausible given that autopsy studies have identified incidental thyroid malignancy in up to 36% of specimens (23). In another study, exclusion of such microcarcinomas based on their not being clearly associated with the imaged abnormality because of partial-volume artifacts reduced the incidence of true 18F-FDG–avid incidental thyroid malignancy from 32% to 14% (24).
Our finding that the clinical decision not to investigate an 18F-FDG–avid TI was associated with a worse overall prognosis confirms that the underlying malignancy likely did influence the decision to investigate incidentalomas in this cohort. The exceptionally low incidence of persistent clinically significant thyroid cancer in this series suggests that this decision was generally made appropriately. The proportion of investigated 18F-FDG–avid TI in a large metaanalysis (3)—mean, 35% (range, 11%–100%)—is similar to our cohort (36%) and suggests that this principle is also applied variably in other centers.
Our study findings support a more cautious contextual approach to the investigation and management of 18F-FDG–avid TI. In the first instance, we advocate an individualized approach to further investigation, recognizing that further evaluation of 18F-FDG–avid incidentalomas may be associated with patient anxiety, additional costs, and potential morbidity associated with aggressive investigation (2). Notably, our findings suggest that the management of incidental thyroid cancer in this setting is likely to have negligible impact on the patient’s outcome despite additional risks associated with potentially unnecessary surgery and delay of definitive treatment of the underlying malignancy. We recommend limiting further investigation to patients with an otherwise favorable prognosis for whom diagnosis of incidental thyroid carcinoma may be clinically relevant. This decision involves careful consideration of factors associated with the patient (age, nononcologic morbidity), the underlying malignancy (persistent 18F-FDG avidity, stage), and local features such as adjacent 18F-FDG–avid neck nodes on the PET scan. In many patients (particularly those with a condition, such as lymphoma, for which 18F-FDG PET is routinely used in restaging), investigation of the 18F-FDG–avid TI can be deferred until after successful treatment of the underlying malignancy. As previously highlighted by Ginsberg, the reporting nuclear medicine specialist may practically convey this message by stating that “incidental FDG-avid thyroid nodule is of doubtful clinical relevance in the context of FDG-avid metastatic malignancy” (25).
If a diagnosis of papillary thyroid cancer is confirmed, we strongly recommend consideration of active surveillance (Fig. 5) (26), consistent with the recommendations of the American Thyroid Association guidelines for patients with a relatively short life expectancy in whom the benefits of intervention may not be realized (4). A period of observation provides a clearer understanding of the prognosis associated with the underlying malignancy in addition to the biology of the incidental thyroid carcinoma. Moreover, some of these patients will have serial 18F-FDG PET studies for the underlying malignancy, providing a further opportunity for surveillance of the incidental thyroid lesion without performing additional investigations. It is important that all clinicians, from the PET reporting nuclear medicine specialist to the referring oncologist, endocrinologist, and thyroid surgeon, be informed of this approach from the outset to provide a consistent message to the patient.
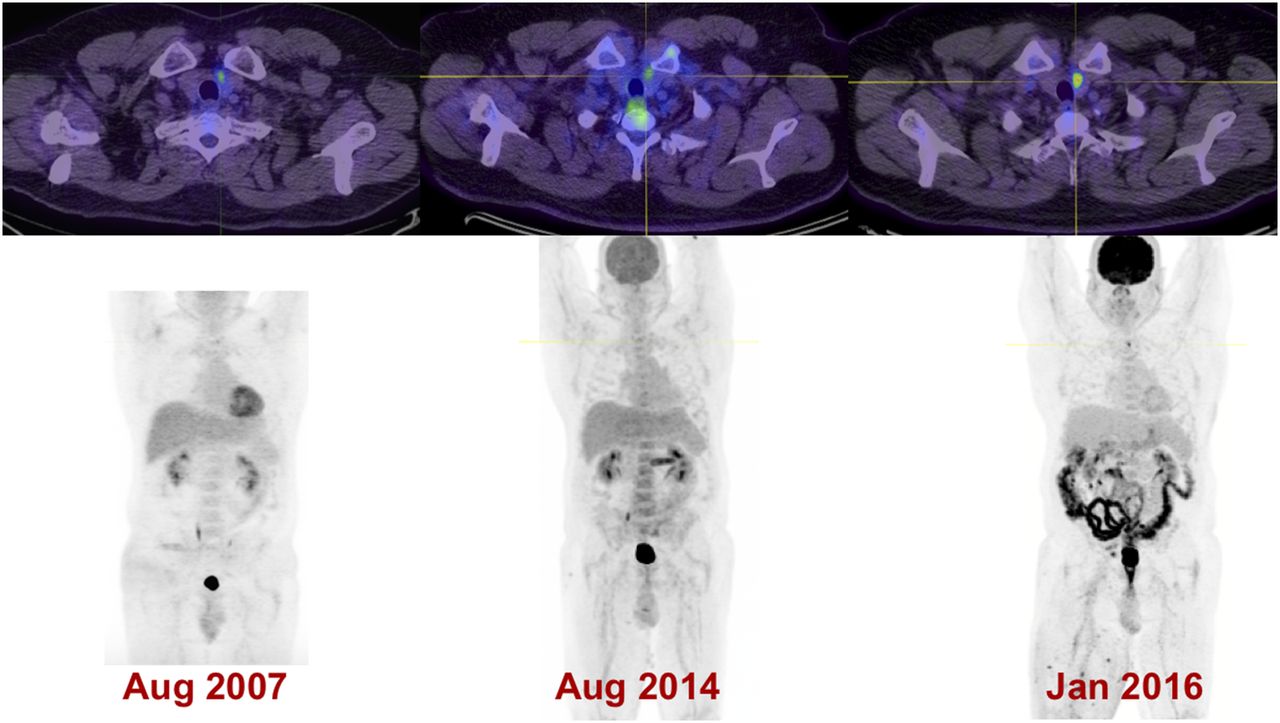
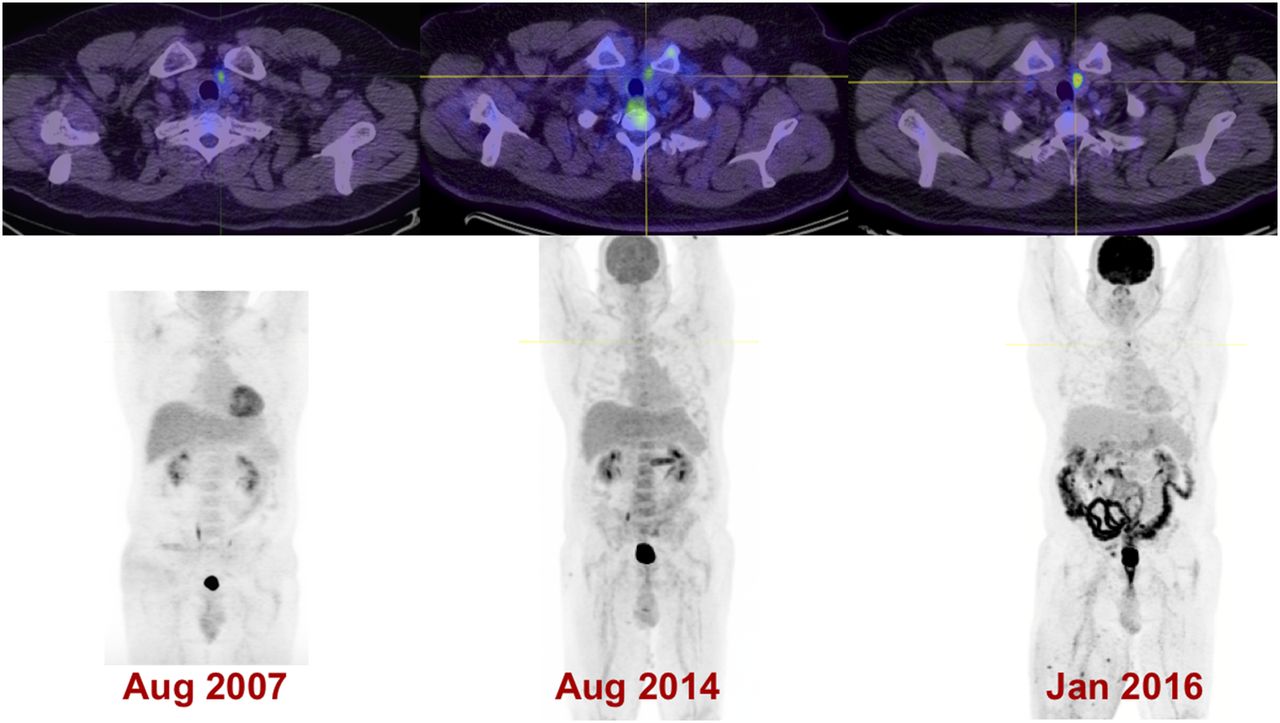
Mildly 18F-FDG–avid TI (SUVmax, 3.1) was initially identified on staging 18F-FDG PET/CT of 59-y-old man with metastatic melanoma in 2007. FNA (performed to exclude metastatic melanoma) confirmed incidental papillary thyroid malignancy, which remains stable under surveillance imaging and of limited clinical significance in setting of metastatic melanoma under active treatment.
The retrospective nature of the study is a potential limitation, and 28% of identified cases of 18F-FDG–avid TI were excluded from analysis. However, most of these are explained by the fact that the patient was attending our referral center only for PET imaging, not for clinical follow-up, and only a modest 8.4% of the total identified cases received less than 12 mo of clinical follow-up. Furthermore, a prospective study would be challenging to implement for a relatively rare incidental pathology in this patient cohort, and the overall proportion of investigated patients was similar to that seen in other studies. Importantly, the follow-up for meaningful clinical outcomes in all patients (irrespective of the extent of thyroid investigation) is an advantage of our study design that eliminates the potential for verification bias seen in most prior studies of 18F-FDG–avid incidentalomas. Referral bias to a comprehensive cancer center is a possible limitation of this study. However, we believe the results remain generalizable because malignancy remains the most common PET indication and most PET scans were performed for standard approved indications.
Our study identified only cases of 18F-FDG–avid thyroid cancer, and incidental thyroid cancer that was not 18F-FDG–avid was also likely to have been present in this patient population. Furthermore, metastatic thyroid cancer exists on a spectrum from well-differentiated (typically iodine-avid) to poorly differentiated (typically 18F-FDG–avid) disease described as the flip-flop phenomenon (27). However, both types of disease may be present in the same patient because of metastatic disease heterogeneity, and in one study up to 33% of metastatic lesions demonstrated both iodine and 18F-FDG uptake (28). This has important management implications in determining suitability for radioactive iodine therapy, and consequently, a combination of both iodine and 18F-FDG PET/CT imaging has been advocated in the treatment of advanced thyroid cancer (29).
A strength of this study is the focus on the presence of the clinically meaningful thyroid cancer outcomes of structural incomplete response or death in this patient population with a limited life span. Furthermore, the large population and long duration of follow-up—362 patients for a median of 2 y—adds to the validity of the study findings.
CONCLUSION
Overall survival in this large cohort of patients with 18F-FDG–avid TI was poor because of the prognosis associated with the underlying malignancy, compared with a minimal survival impact from 18F-FDG–avid TI. 18F-FDG avidity in the known malignancy, and to a lesser extent advanced stage of this malignancy and a decision not to investigate the 18F-FDG–avid TI, were significant predictors of overall mortality in this cohort. The prognosis of the underlying malignancy should be considered before 18F-FDG–avid TI is investigated, as the potential benefits of intervention may not be realized because of the short life expectancy. Active surveillance of patients diagnosed with incidental 18F-FDG–avid papillary thyroid carcinoma should be considered.
DISCLOSURE
Rodney Hicks is supported by a National Health and Medical Research Council of Australia Practitioner Fellowship. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We gratefully acknowledge assistance from Elizabeth Drummond (research assistant) for access to the database, Jason Callahan (nuclear medicine technologist) for access to the PET/CT workstation, and Professor Michael Henderson (deputy director of the Department of Surgical Oncology).
Footnotes
↵* Contributed equally to this work.
Published online Oct. 12, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 23, 2017.
- Accepted for publication September 11, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}