


TO THE EDITOR: With great interest, we read the recent article by Renaud et al. entitled “Characterization of 3-Dimensional PET Systems for Accurate Quantification of Myocardial Blood Flow” (1). The authors describe a method to obtain the maximum injected activity for which accurate quantification of myocardial blood flow (MBF) can be achieved. We think that this method majorly contributes to the existing knowledge. It shows that accurate dynamic PET imaging is possible for a range of 3-dimensional PET systems if maximum injected activities are respected to limit peak dead-time losses during the bolus first-pass transit.
The authors translated the maximum activities for accurate MBF as determined by phantom studies to maximum patient-specific tracer activities (in MBq/kg). However, in our opinion, this translation might be an oversimplified approach, because the activity distribution and photon attenuation in patients during the first-pass transit do not solely depend on body weight. We think that application of the presented method may lead to higher counting rates in some patients than the maximum counting rates as derived from the phantom study. These higher counting rates may subsequently hamper accurate MBF quantification.
To ground our viewpoint, we obtained the maximum prompt coincidence counting rate on our PET system (Ingenuity TF; Philips Healthcare) using the same phantom as described by Renaud et al. (1). Next, we retrospectively obtained the maximum accepted counting rates during myocardial perfusion imaging at rest with 82Rb PET for 72 consecutive patients. All patients provided written informed consent for the use of their data for research purposes. An activity of 740 MBq was injected at a flow of 50 mL/min (CardioGen-82; Bracco Diagnostics Inc.) in the phantom and in patients. Next, we studied the effect of using the recommended injected activity per body weight as proposed by Renaud et al. (1). Therefore, we multiplied the measured maximum counting rate, normalized to the injected activity, with body weight and 4.6 MBq/kg for each patient. This way, we obtained a simulated maximum counting rate when using 4.6 MBq/kg. We chose 4.6 MBq/kg because this is the maximum activity per body weight ensuring accurate quantification for a comparable PET system (Gemini; Philips Healthcare) (1). The body weight equivalent of the phantom was set at 50 kg (1).
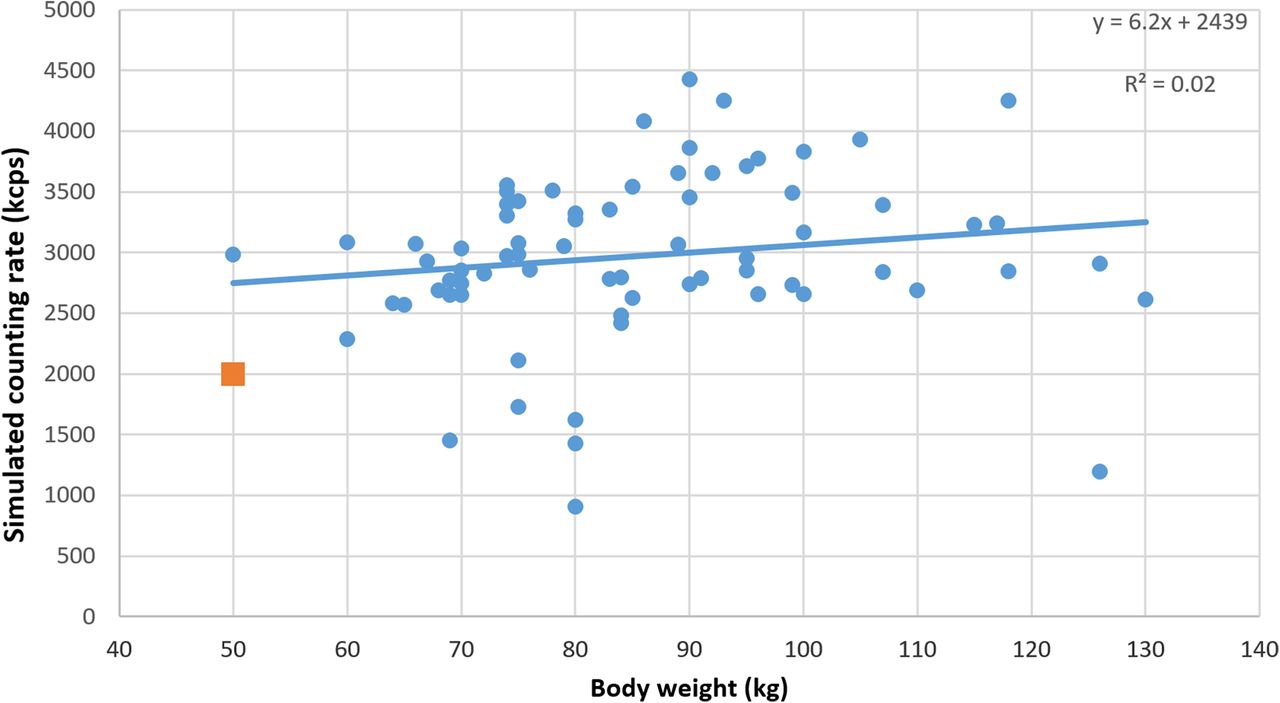
The maximum simulated counting rate for the phantom was 2,001 kcps. The mean body weight of the included patients was 86 ± 17 kg, and the body mass index was 28.6 ± 5.4 kg/m2. We found a mean simulated maximum counting rate of 2,975 ± 681 kcps, with a large range of 909–4,431 kcps (Figs. 1 and 2). In 66 patients (92%), we found a maximum counting rate that was higher than 2,001 kcps, the value that we derived from our phantom study. This implies that the suggested translation to 4.6 MBq/kg may result in counting rates exceeding the 10% activity bias criteria (1) in 92% of the patients, possibly leading to biased MBF measurements. Nevertheless, our results support the use of a weight-based activity, because this resulted in simulated maximum counting rates that were independent of body weight.

Maximum counting rate as encountered in patients (dots) and in phantom (square), normalized to 82Rb tracer activity, as function of body weight. Line represents linear fit. Fit result and coefficient of determination are included in top right corner.

Simulated maximum counting rate in patients (dots) and in phantom (square) when 4.6 MBq/kg of 82Rb was applied as function of body weight. Dashed line represents linear fit. Fit result and coefficient of determination are included in top right corner. Maximum simulated counting rate was higher in 92% of patients than the phantom result. Furthermore, there was no significant correlation between maximum counting rate and body weight when 4.6 MBq/kg was applied.
Applying a lower maximum injected weight–based activity than the one suggested by Renaud et al. (1) can account for the large variation in maximum counting rates encountered in patients and may prevent biased MBF measurements. To ensure accurate MBF quantification with 82Rb PET across all patients, we therefore suggest the inclusion of a correction in the translation of phantom results to the maximum weight–based activity in patients.
Footnotes
Published online Jan. 19, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCE
- 1.↵





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.