


Abstract
Methionine transport across plasma membranes occurs via the large amino acid transporter, which is overexpressed in malignant cells, leading to tracer accumulation within tumors. We investigated the uptake of 11C-methionine (11C-MET) in children and young adults with Hodgkin lymphoma (HL) or non-Hodgkin lymphoma (NHL) and compared the biodistribution of 11C-MET PET/CT with that of 18F-FDG PET/CT. Methods: Conducted under an investigational new drug authorization, we prospectively enrolled patients with newly diagnosed HL (n = 19) and NHL (n = 2) onto the Institutional Review Board–approved investigation of 11C-MET PET/CT. After a minimum 4-h fast, patients received 740 MBq/1.7 m2 (maximum, 740 MBq [20 mCi/1.7 m2; maximum, 20 mCi]) of 11C-methionine intravenously. PET/CT was performed 5 min after injection from the vertex to thighs at 3 min per bed position. In a separate session, patients received 5.5 MBq/kg (maximum, 485 MBq [0.15 mCi/kg; maximum, 12 mCi]) of 18F-FDG with imaging initiated approximately 1 h after radiopharmaceutical administration. All studies were reviewed by consensus of 2 senior imaging specialists. The presence of metabolic activity on baseline studies was compared among 17 nodal groups. Results: Eighteen patients (11 male; median age, 15.2 y; age range, 9.5–22.6 y) comprised the study cohort. All had paired 11C-MET PET/CT and 18F-FDG PET/CT studies at diagnosis. At baseline, 3 nodal groups demonstrating discordant metabolic activity by both 18F-FDG PET/CT and 11C-MET PET/CT were Waldeyer’s ring, paraaortic region, and the liver. All others were found to have concordant metabolic activity. Normal intense 11C-MET uptake in the pancreas and liver reduced sensitivity for disease detection in these regions. At follow-up, 14 of 15 study pairs had concordant results. Conclusion: 11C-MET uptake is elevated in most regions involved with lymphoma at diagnosis and follow-up. Its utility in the abdomen is limited by uptake in normal structures.
Protein formation is integral for cellular growth and replication. Methionine is a naturally occurring essential amino acid critical not only for protein formation but also for phospholipid synthesis through intermediate compounds. When labeled with 11C, a radioactive isotope of the naturally occurring carbon-12, the distribution of methionine can be determined noninvasively using a PET camera. Imaging with 11C-methionine (11C-MET) has proven useful for a variety of neoplasms, because of its increased uptake via large amino acid transporter (LAT1) (1).
Despite the interest in 11C-methionine imaging for brain tumors, results of few other investigations regarding the role of this agent in tumor imaging are available. Thus, we sought to characterize the activity of LAT1 in pediatric and young adult patients with lymphoma, assess the biodistribution of the tracer in tumor sites, and compare with 18F-FDG PET/CT used for staging and response (2).
18F-FDG is a valuable radiopharmaceutical tracer to stage, monitor response to therapy, and detect relapsed disease in lymphomas occurring in both adults and children. Nevertheless, 18F-FDG has limitations to its use (3). 18F-FDG uptake largely reflects glucose transport, which is increased not only in many tumors, but also in common nonneoplastic conditions such as infections and inflammation. Thus, 18F-FDG is a sensitive tracer for detecting increased glucose metabolism, but nonneoplastic etiologies may mimic tumor uptake, thus reducing specificity when screening for cancer (3–5). There is therefore a need for more tracers with greater specificity for malignancy.
We evaluated the activity of LAT1 in sites of lymphoma using the tracer 11C-MET as a transporter substrate. We examined the potential usefulness of PET/CT imaging with 11C-MET in the evaluation of children and young adults with lymphoma in initial disease staging, and in response to therapy, and compared response assessment of disease between 11C-MET and 18F-FDG.
MATERIALS AND METHODS
Our investigation was initiated after obtaining Institutional Review Board approval and was conducted under an investigational new drug authorization. Data management complied with the Health Information Portability and Accountability Act of 2013.
Recruitment Process
With agreement from the primary institutional attending physician and on determination of the patient’s eligibility, the patient was approached for enrollment. Patients included in this report were recruited from August 2009 through November 2013. Patients of any age were eligible for enrollment if they had known or suspected lymphoma, had scheduled clinical imaging evaluations that included 18F-FDG PET/CT within 4 wk of entry, and had provided an informed consent form (signed by participant, parent, or guardian) and assent according to the guidelines of the Institutional Review Board. The Institutional Review Board approved this study. To be evaluable, newly diagnosed patients with Hodgkin lymphoma (HL) or non-Hodgkin lymphoma (NHL) could not have started therapy before the initial 11C-MET PET/CT or 18F-FDG PET/CT scans (Fig. 1).

Consort diagram. BAT = brown adipose tissue.
Exclusion criteria included pregnancy, treatment having already started, and the inability or unwillingness of research participant, parent, or legal guardian/representative to give written informed consent; female participants could not be breast feeding because of the theoretic potential of harm to the infant from exposure to ionizing radiation from the radiopharmaceutical.
Technical Factors for 11C-MET
Participants fasted for at least 4 h before imaging. Patients then received 740 MBq (20 mCi) of 11C-MET per 1.7 m2 of body surface area (maximum prescribed dose, 740 MBq [20 mCi]) intravenously. Transmission CT image acquisitions, for attenuation correction and lesion localization, and PET image acquisitions were initiated approximately 5 min later using a Discovery LS PET/CT or a Discovery 690 PET/CT system (GE Healthcare). Images from the top of the head to the mid thighs were acquired at 3 min per bed position.
Technical Factors for 18F-FDG
After a minimum of 4 h of fasting, blood glucose was assessed before 18F-FDG injection. If blood glucose was determined to be within normal limits, 5.5 MBq/kg (0.15 mCi/kg) of 18F-FDG (maximum, 444 MBq [12 mCi]) were injected intravenously. Patients were kept in a quiet, dark room after injection and were instructed to relax with their arms at their sides in a recumbent position. Approximately 1 h later, transmission CT images, for attenuation correction and lesion localization, and PET emission images were acquired using a Discovery LS PET/CT or a GE Discovery 690 PET/CT system (GE Healthcare). Images were obtained from the top of the head through the feet at 5 min per bed position on the Discovery LS in 2-dimensional mode and 3–5 min per bed position on the GE Discovery 690 PET/CT in 3-dimensional mode.
The scans were typically obtained an average of 4 d between the 2 studies (median, 1.5 d). For those for whom the studies were performed on the same day, 11C-MET PET/CT was performed first, with injection of 18F-FDG administered 2 h after 11C-MET. 18F-FDG PET/CT scans were thus obtained 3 h after the injection of 11C-MET, at which time less than 0.2% of the injected dose of 11C-MET would remain.
Technical Factors for CT Obtained for Attenuation Correction and Lesion Localization
CT acquisition parameters included a slice thickness of 0.5 cm, tube rotation of 0.8 s, table speed of 1.5 cm/rotation, and pitch of 1.5:1, at 120 kV and 90 mA, with dose modulation. PET and CT data were reconstructed into multiplanar cross-sectional images using standard vendor-supplied software and displayed on a nuclear medicine workstation (Hermes Medical Solutions) for analysis.
Imaging Review
18F-FDG and 11C-MET PET/CT data were all reviewed by a nuclear medicine physician and a pediatric radiologist, each with more than 25 y of experience, and scored by consensus. To avoid bias, studies were reviewed in groups by study type (i.e., all 18F-FDG PET/CT images were reviewed as 1 group, and 4 wk later 11C-MET PET/CT images were reviewed as a separate group). Study review was performed without knowledge of clinical findings or the results of other studies of each patient.
Individual lymph nodes; nodal masses; and lung, skeletal, and solid organ lesions were coded as positive if the metabolic activity exceeded that of adjacent background tissues. Individual lymph nodes were then classified into 17 groups: Waldeyer’s ring (including nasopharyngeal, tonsillar, and base of tongue), right and left neck (including supraclavicular nodal groups), right and left axilla, mediastinum (including epicardial, internal mammary, diaphragmatic nodes), right and left pulmonary hila, abdominal (including paraaortic, porta hepatic, retroperitoneal, mesenteric, and celiac nodal groups), liver, spleen (including splenic hilar), and pelvic (right and left iliac, and right and left inguinal/femoral). Lung, bone, or bone marrow involvement was each classified as individual sites. The range, median, and maximum SUVs were recorded for each site for both radiopharmaceuticals.
RESULTS
Staging
Between August 2009 and the end of November 2013, 21 of 85 (25%) potentially eligible patients with HL (n = 67) or NHL (n = 18) were enrolled (median age, 15.2 y; age range, 9.5–22.6 y). Eleven patients were boys. Eighteen patients with paired studies were evaluable at diagnosis, because 1 patient had to be excluded due to extensive uptake in brown adipose tissue and 2 had missing paired studies. Of this population, 17 had a diagnosis of HL and 1 of NHL.
At the time of diagnosis, 14 of 17 regions evaluated showed concordant uptake of both tracers (Figs. 2 and 3). Three nodal groups demonstrated discordant metabolic activity between 18F-FDG and 11C-MET: Waldeyer’s ring, paraaortic region, and liver (Fig. 4). Intense 11C-MET uptake in the pancreas and liver interfered with disease detection in the liver, porta hepatis, and upper retroperitoneum (Table 1; Fig. 4).

A 22-y-old woman with mediastinal lymphadenopathy. Biopsy showed nodular sclerosing HL. (A) Maximum-intensity-projection images (11C-MET left, 18F-FDG right) show intense though variable uptake of both tracers throughout mediastinal masses. Small focus of 11C-MET appearing over right midchest lay within tubing leading to the central line. Images are normalized to SUVmax of 5.0 for 11C-MET and 8.0 for 18F-FDG. (B) Transverse images (left column, PET; middle column, attenuation-correction CT; right column, fusion) through lower aspect of mediastinal mass (11C-MET top, 18F- FDG bottom). Uptake of both tracers is slightly heterogeneous, but regional distribution is largely concordant. Images are normalized to SUVmax of 5.0 for 11C-MET and 8.0 for 18F-FDG.

A 17-y-old girl with mixed cellularity HL. Maximum-intensity-projection images (11C-MET left, 18F-FDG right) show intense uptake in left cervical and supraclavicular masses. Images are normalized to SUVmax of 7.0 for 11C-MET and 5.0 for 18F-FDG.
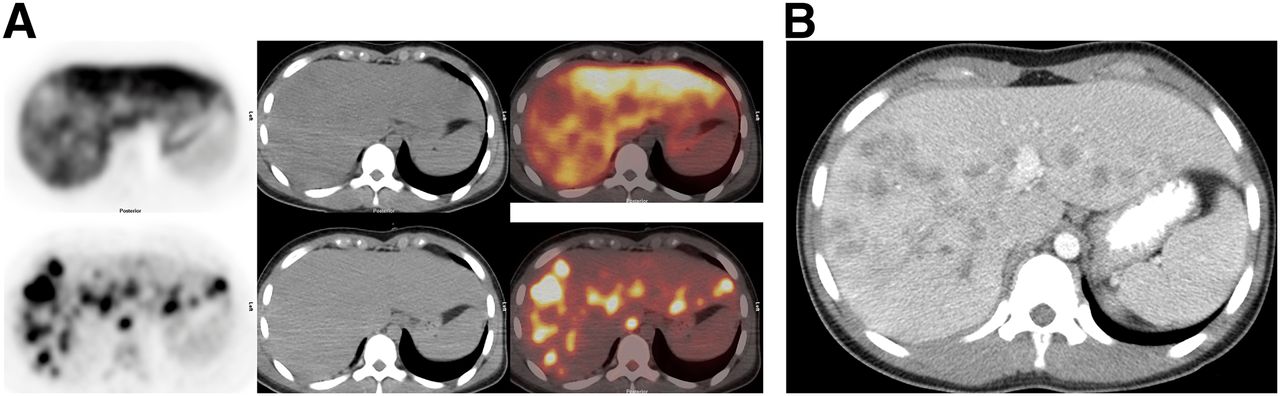
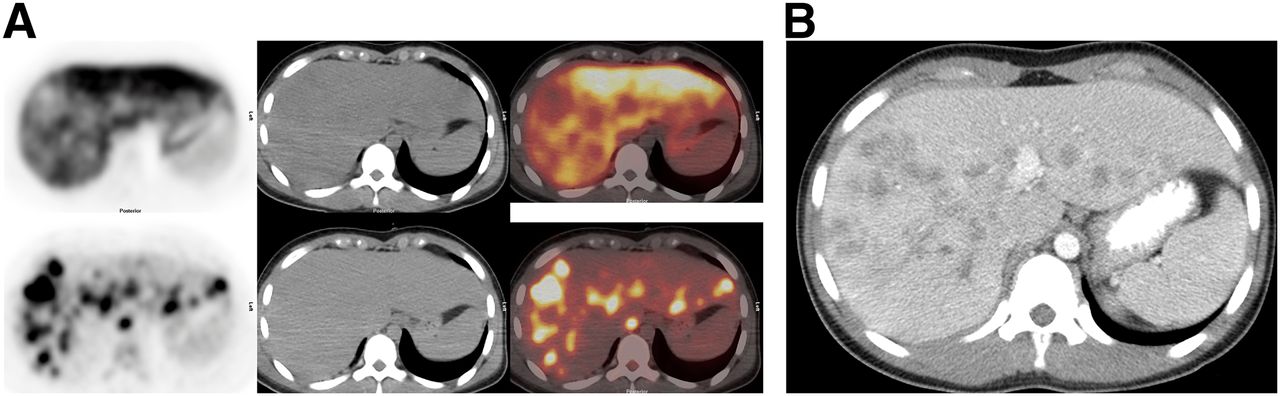
A 15-y-old girl with widespread nodular sclerosing HL. (A) Transverse images (left column, PET; middle column, attenuation-correction CT; right column, fusion) through upper aspect of liver (11C-MET top, 18F-FDG bottom). Intense uptake of 11C-MET renders hepatic metastases to appear as areas of low activity in comparison to normal liver. Hepatic metastases are quite discernible on 18F-FDG images. Images are normalized to SUVmax of 15.0 for 11C-MET and 7.0 for 18F-FDG. (B) Contrast-enhanced CT scan through same region shows many areas of low attenuation consistent with extensive liver involvement.
Comparison of Number of Cases at Study Entry Demonstrating Metabolic Activity by 18F-FDG and 11C-MET by Anatomic Regions
The number of abnormal sites of metabolic activity was nearly identical for both tracers except for nearly one-third more foci being identified within the abdomen with 18F-FDG than with 11C-MET (Table 2). Further, the median intensity of activity as represented by SUVs was similar in most regions. However, the range of uptake was greater with 18F-FDG, particularly in the mediastinum, hila, and abdomen in which the SUVmax was 2–3 times greater than with 11C-MET (Table 2).
Comparison of Metabolic Activity (SUV) by 11C-MET and 18F-FDG by Anatomic Region
Restaging
All patients were treated according to institutional guidelines or enrolled on protocol when available. Of the 18 enrolled patients, the patient with diffuse large B cell lymphoma (NHL) was treated according to previously published standard therapy (4). Eleven HL patients were treated with a modified Stanford V protocol (5,6), 4 according to a modified German Pediatric Oncology/Hematology-Hodgkin Disease 2002 regimen (7), 1 according to German Hodgkin Study Group-14 trial (8), and 1 with stage IA lymphocyte predominant HL was observed without further treatment after complete excision of the affected lymph node. After 8 wk of therapy, paired follow-up imaging was available for 15 patients (1 patient underwent 11C-methionine follow-up imaging but lacked the corresponding 18F-FDG study, and 2 patients declined further participation) (Fig. 5). In 14 patients, uptake of 11C-MET and 18F-FDG was concordant. In 4 patients, both 18F-FDG and 11C-MET remained positive, and in 10 patients abnormal uptake of both tracers resolved. In 1 patient, metabolic activity was minimally discordant where the 18F-FDG study had normalized but the 11C-MET study remained slightly positive in the right internal mammary and left infraclavicular nodal regions. Subsequent review of the studies in combination indicated only slight discrepancy in uptake, likely due to lower mediastinal background in 11C-MET images. This patient is alive and well without relapse more than 3 y from diagnosis. None of the patients in this study had documented bone marrow disease.
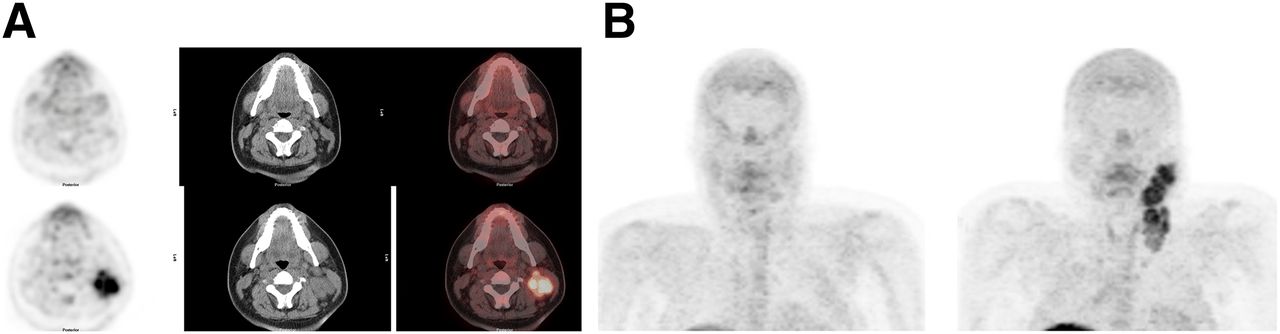
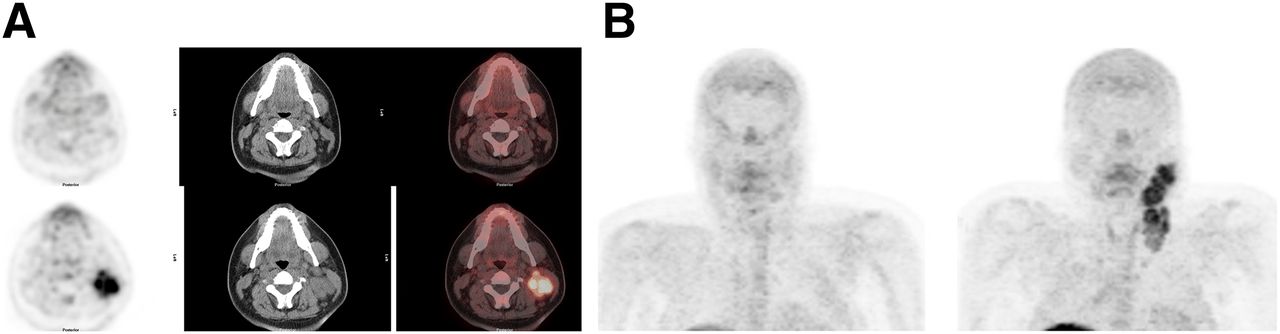
A 16-y-old boy with mixed cellularity HL. 11C-MET images after 8 wk of chemotherapy and at presentation. (A) Transverse images after 8 wk of chemotherapy (top row) and at presentation (bottom row) (left column, PET; middle column, attenuation-correction CT; right column, fusion). There has been resolution of abnormal 11C-MET activity and considerable reduction in size in left cervical sites. (B) Maximum-intensity-projection images after 8 wk of chemotherapy (left) and at presentation (right) show that activity within neck has become normal during treatment.
Outcomes
There were no adverse events associated with the study, and all patients remain alive at a median of 3 y (range, 1.0–5.7 y) from diagnosis. Three patients developed disease recurrence at a median of 0.4 y (range, 0.3–2.3 y), and 1 patient with HL developed a secondary NHL (diffuse large B cell lymphoma) at 1.4 y from original diagnosis; all patients have been seen in our institution within the last 6 mo.
DISCUSSION
Within the neck and axilla, the number of abnormal foci independently identified without reference to the other studied tracer was nearly identical for 11C-MET and 18F-FDG. This finding may be due to the low background uptake of either tracer in the neck and axilla, facilitating detection of abnormal foci, as well as the most common sites of disease in this patient population. Nearly 3 times as many abnormal foci were discovered within the abdomen and pelvis with 18F-FDG than with 11C-MET, reflecting the intense, normal uptake of 11C-MET within the liver and pancreas, which may obscure foci of abnormal uptake, as also reported by Sutinen et al. in a cohort of 55 adult patients with lymphoma (9). Too few lesions were noted in the spleen to allow for comparison of detection between 18F-FDG and 11C-MET. Except for the axilla and pelvis, median uptake was about 1.5–2.5 greater with 18F-FDG than with 11C-MET.
The value of determining metabolically active disease regardless of the anatomic characteristics of lymphoma has been well-established (10). 18F-FDG serves as a sensitive but not entirely tumor-specific agent widely used for detection and response evaluation of lymphomas, but its lower specificity for malignant disease may complicate study interpretation (11). 18F-FDG has been used to identify most lymphomas although slightly fewer sites in indolent lymphomas were detected using 18F-FDG than 67Ga scintigraphy (12). The authors further reported that 11C-MET showed all sites of lymphoma identified by 18F-FDG, which contrasts with our finding of 11C-MET identifying fewer sites of metabolically active disease in the abdomen and pelvis than 18F-FDG. The ability of 11C-MET to distinguish between high- and low-grade lymphomas has not been conclusively established (13,14).
Most studies describing amino acid tracers in oncologic imaging using 11C-MET have been for central nervous system neoplasms, and its role in clinical management has been described (15). 11C-MET has also been explored for its potential utility in patients with lymphomas (16). Nuutinen et al. found that 11C-MET accumulated in 31 of 32 lymphomas (27/28 NHL, 4/4 HL), the exception being a superficial skin lesion. The sensitivity was 97%, and there were no false-positive findings. 11C-MET accumulation was high in all grades of lymphoma. When kinetic analysis was performed, the difference in 11C-MET uptake between high-, intermediate-, and low-grade tumors was statistically significant. Yoshida showed that 11C-MET activity in lymphomas (6 patients with NHL, 1 patient with HL) peaked about 10 min after injection and remained nearly constant for at least 30 min. The authors compared methods using blood samples with DAR (differential absorption ratio, now referred to as SUV) obtained using images only and found they were highly correlated (r = 0.875). They concluded that the DAR gave almost the same result as the more complicated dynamic analyses using blood sampling (17). In our article, we chose SUV for semiquantitative comparisons between tumor uptake of 11C-MET and 18F-FDG, recognizing that comparison between tracers reflects multiple factors, including the injection to imaging interval, the background biodistribution of the tracers, and the tumor avidity for the particular agent.
Ogawa et al. (18) used 11C-MET in the follow-up of radiotherapy of primary central nervous system lymphoma. Nine patients with primary brain lymphoma and 1 patient with secondary central nervous system involvement were the subjects. As has been documented in primary central nervous system tumors, 11C-MET uptake was higher in tumor than in uninvolved brain before therapy. In most patients, the extent of 11C-MET uptake correlated well with contrast enhancement on MRI and CT, but in 2 patients, the extent of 11C-MET uptake was larger than the areas of enhancement on CT and MRI. The uptake intensity of 11C-MET declined after radiotherapy, but the extent of uptake was larger than the areas of enhancement on CT and MR in 8 patients. One patient had a recurrence at the site of residual 11C-MET uptake after radiotherapy. Uptake in the tumor declined from an SUV of 4.3 ± 1.8 to an SUV of 1.9 ± 0.5 after radiotherapy. Importantly, the uptake in normal, uninvolved brain did not change (SUV of 1.4 ± 0.3 at baseline and 1.6 ± 0.3 after radiotherapy). As do others, the authors believed that a larger area of 11C-MET uptake compared with contrast enhancement on MR and CT indicated tumor infiltration beyond the borders of contrast enhancement. The authors concluded that 11C-MET PET might be useful for detecting residual tumor after treatment and for early diagnosis of recurrent intracranial disease.
Methionine and other neutral amino acids with large, branched, or aromatic side chains, including phenylalanine and tyrosine, are transported into cells by LAT1 (19). LAT1 is also the transporter for amino acid–related molecules such as l-dopa, thyroxine, and tri-iodothyronine as well as the chemotherapeutic agent melphalan (L-phenylalanine mustard) (20). LAT1 is found in the brain, placenta, and liver, and it is overexpressed in many types of tumors including gliomas (21). Inhibition of LAT1 has been reported to have antitumor activity in vitro and in vivo (20). If effective therapies using LAT1 inhibitors are developed, it is possible that tracers that examine the functional integrity of LAT1, such as 11C-MET or other amino acids and amino acid derivatives such as 18F-FET (fluoroethyl tyrosine) (22), could serve as a method to assess antitumor efficacy.
Other radiotracers have been used to assess the activity of lymphomas (23). 18F-FLT is the thymidine analog 3′-deoxy-3′-18F-fluorothymidine (24–26). Buck demonstrated that in a mouse model, 18F-FLT showed a response to chemotherapy before changes in tumor size occurred. Buchmann showed that 18F-FLT could be used to image both aggressive and indolent NHL. However, there was substantial normal accumulation in bone marrow and liver, which, similar to 11C-MET, may interfere with disease assessment in these organs. Kasper examined 15 patients with HL and 33 with NHL who had residual masses larger than 2 cm after treatment. Both 18F-FDG and 18F-FLT were useful in distinguishing between patients with long or short overall survivals, predicting those at greater risk for disease relapse. Those patients with 18F-FDG– or 18F-FLT–negative scans were found to have improved survival compared with those whose scans remained positive after therapy. The authors concluded that combining 18F-FLT with 18F-FDG in this clinical situation provided no additional information.
CONCLUSION
We have found that most sites of tumor involvement in children with HL and NHL are well visualized using 11C-MET PET/CT. Tumor sites in the neck and chest were particularly evident because of the low background uptake of methionine in these areas. However, within the abdomen, we found that uptake in the liver was more intense than tumor. Thus, sites of tumor appeared as cold spots. Furthermore, we expect that normal bone marrow uptake will interfere with detection of tumor bone marrow involvement. Tumor uptake declined markedly with treatment, in most patients resolving in 8 wk, indicating that the activity of LAT1 decreases with effective tumor treatment. Thus, amino acid imaging using 11C-MET demonstrates consistent overexpression of LAT1 in pediatric lymphomas at diagnosis and subsequent decline in expression in most patients during therapy, similar to glucose transporters.
DISCLOSURE
No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 8, 2016.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 8, 2016.
- Accepted for publication August 22, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Enzyme-mediated depletion of serum L-Met abrogates prostate cancer growth via multiple mechanisms without evidence of systemic toxicity
- Reply: The Need for Prudence When Using 18F-FDG PET as a Reference Standard for Lymphoma Detection
- The Need for Prudence When Using 18F-FDG PET as a Reference Standard for Lymphoma Detection