


Abstract
68Ga-DOTATATE PET/CT provides information on the location of somatostatin receptor–expressing tumors. Integrating this imaging data effectively in patient care requires the clinical history; the histopathology and biomarker information; and the grade, stage, and prior imaging results. Previous therapies and technical aspects of the study should be considered, given their ability to alter the interpretation of the images. This includes physiologic biodistribution of the radiotracer, as well as conditions that engender false-positive results. This article provides a guide to the performance and interpretation of 68Ga-DOTATATE PET/CT and describes its role in the diagnostic algorithm of neuroendocrine neoplasms and its overall utility in their management.
Neuroendocrine neoplasms exhibit variable symptomatology, such as tumor mass effects or the biologic consequences of the bioactive amine secretion, frequently delaying diagnosis. Some patients present with symptoms related to inappropriate peptide or amine hypersecretion, but most of these tumors are nonfunctioning. Nonfunctioning tumors are usually discovered when they are large and have metastasized to the liver. Thus, even though the lesions are mostly well differentiated and slow-growing, with a minority of aggressive forms, the outcome may be poor because of diagnostic delay (1).
Somatostatin receptor (SSR) imaging offers an opportunity to identify receptor-expressing neuroendocrine neoplasms (NENs) (2,3). Radiolabeled somatostatin analogs (SSA) were introduced in the 1980s for imaging of NENs (Fig. 1) (4,5).

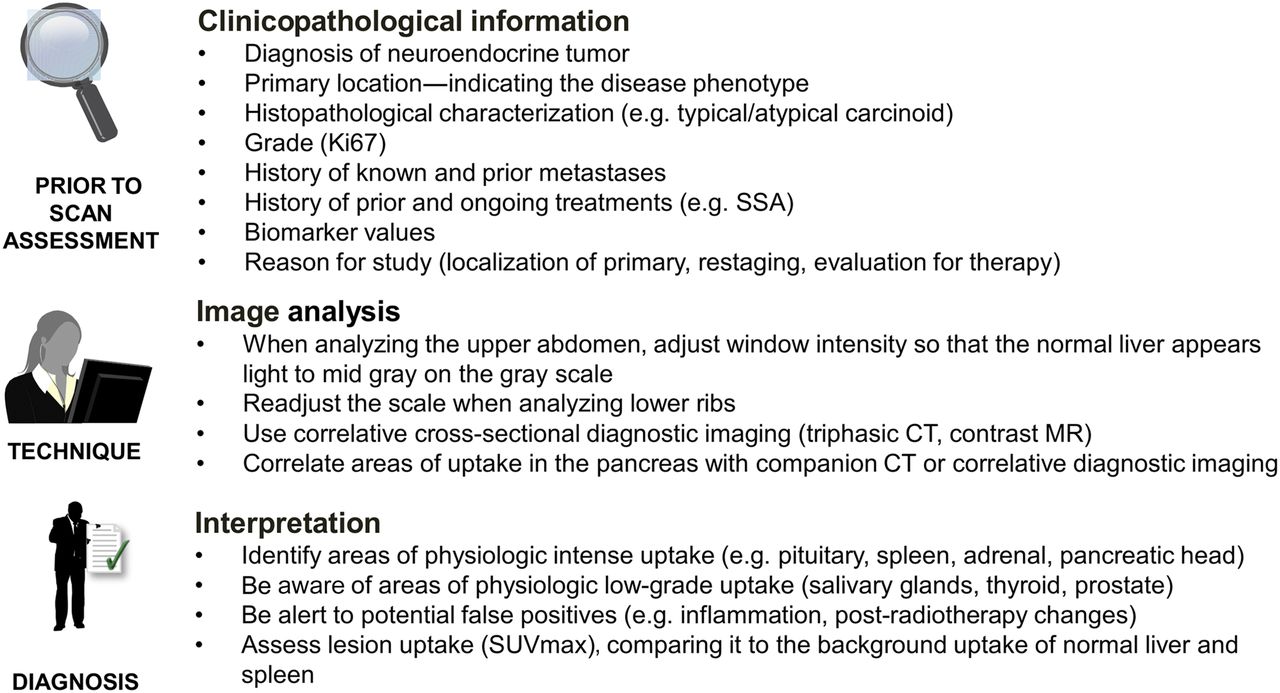
Optimal strategy for 68Ga-DOTATATE PET/CT evaluation.
CLINICAL SCENARIO
NENs are relatively rare tumors originating from ubiquitous neuroendocrine cells distributed throughout the body. These cells synthesize, store, and secrete various circulating hormones and neurotransmitters (Table 1) (6).
Gastrointestinal and Pancreatic Neuroendocrine Cell Types and Secretory Products
NENs constitute 0.66% of all malignancies in the United States, according to the Surveillance, Epidemiology, and End Results database, containing 48,195 NENs from 1970 to 2006, with an incidence increasing at a rate of 3%–10% per year (7). This increment is related to the introduction of more sensitive diagnostic tools and to an increased awareness by clinicians and pathologists (1,8). The prevalence of NENs is substantial given the often indolent nature of the disease process. Most (66%) arise in the gastroenteropancreatic area, and 25% occur in the lung (7). The recognition that the prevalence of NENs as a gastrointestinal cancer is exceeded only by that of colon cancer has increased focus on the problem (1).
Less frequent forms of NENs include pheochromocytoma, paraganglioma, medullary thyroid carcinoma, and neuroblastoma. Pheochromocytoma and paragangliomas derive from sympathetic chromaffin tissue in the adrenal medulla and from the extraadrenal paraganglial system of the thorax and abdomen (9). The frequent malignant propensity of these tumors reflects the genetic background. More than 50% of tumors are due to genetic alterations (10). Pheochromocytoma exhibits an overall incidence of 0.8 cases/100,000/y over 30 y in the white population, according to the Rochester Epidemiology Project (11).
CLASSIFICATION
Since 1963, many NEN classifications have been adopted, based on the embryologic origin of the tumor (foregut, midgut, hindgut), degree of differentiation, and site of origin (12). The term carcinoid has been abandoned for gastroenteropancreatic NENs. The prognostic assessment of gastroenteropancreatic NENs has improved significantly since the introduction of the European Neuroendocrine Tumor Society and World Health Organization 2010 staging and grading systems. The World Health Organization 2010 classification scores gastroenteropancreatic NENs as G1, G2, or G3 on the basis of the morphology and Ki-67 scoring index (gastroenteropancreatic neuroendocrine tumor G1, Ki-67 < 2%; neuroendocrine tumor G2, Ki-67 = 3%–20%; neuroendocrine carcinoma G3, Ki-67 > 20%) and mixed adenoneuroendocrine carcinoma (13). Although most NENs are well differentiated (G1 or G2), around 5.6%–8% are G3 (Ki-67 > 20%) (14). Recent evidence highlights the need to further stratify patients in the G3 group as well-differentiated neuroendocrine tumor G3 (Ki-67 = 20%–50%) or poorly differentiated neuroendocrine carcinoma G3 (Ki-67 > 50%) on the basis of their different clinical behavior and response to treatment.
The current classification of bronchopulmonary NENs includes typical and atypical carcinoid, large cell neuroendocrine carcinoma, small cell carcinoma, and (considered a preinvasive form) diffuse idiopathic pulmonary neuroendocrine cell hyperplasia. A new classification of lung neuroendocrine tumors has been proposed by the World Health Organization (15) and was endorsed by the European Neuroendocrine Tumor Society. Like the system for gastroenteropancreatic NENs, this 3-tier grading system is centered on the Ki-67 index, with specifically generated cutoffs (bronchopulmonary NEN G1, Ki-67 < 4%, no necrosis; G2, Ki-67 = 4%–25% and necrosis in fewer than 10 high-power fields; G3, Ki-67 > 25% and necrosis in more than 10 high-power fields).
The tumor grade, histopathology type, primary site, and stage reflect the potential metastatic spread and, therefore, the impact on tumor burden and the subsequent choice of therapeutic options (Table 2). Knowledge of these characteristics, together with the prior treatment history, is fundamental in the interpretation of a 68Ga-DOTATATE image.
Site and Clinical Presentation of Gastroenteropancreatic and Bronchopulmonary NENs
68GA-DOTATATE PET/CT
Indications
68Ga-DOTATATE is a radiolabeled SSA indicated for use with PET or PET/CT for localization of SSR-positive NENs in adult and pediatric patients (16).
SSR imaging is used for staging and restaging and to select patients for peptide receptor radionuclide therapy (PRRT) with cold or radiolabeled SSAs (17,18). The rationale for SSR imaging is the tumor cell receptor–mediated internalization of the receptor-radio-analog complex and its retention in the cytoplasm.
Three SSA Peptides and Choice of DOTATATE
111In-pentetreotide, or OctreoScan (Mallinckrodt), was the first approved radiopharmaceutical for NEN imaging. Over the past 15 y, this tracer demonstrated the utility of SSR imaging. The development of 68Ga-labeled agents suitable for use with PET/CT has markedly enhanced lesion detection (because of improved resolution) and quantitation with the 68Ga-labeled octreotide derivatives (68Ga-SSA PET/CT) DOTATOC, DOTANOC, and DOTATATE (18–20). These analogs retain an octreotidelike affinity profile and, in particular, high affinity for somatostatin receptor 2 (e.g., 0.2 ± 0.04 nM for somatostatin receptor 2 with 68Ga-DOTATATE, much greater than the 22 ± 3.6 nM with 111In-pentetreotide (21)). Only 68Ga-DOTANOC exhibits substantial affinity for somatostatin receptor 3 (22). Despite these differences in receptor affinity, a clear superiority of one compound over the others has not been demonstrated. A comparison of 68Ga-DOTATOC versus 68Ga-DOTATATE PET/CT in the same patients yielded comparable diagnostic accuracy, despite potential advantages for 68Ga-DOTATOC in the higher number of detected lesions and the higher SUVmax (23). However, a recent comparison of 68Ga-DOTATATE and 68Ga-DOTANOC PET/CT in the same NEN patients showed a higher SUVmax for 68Ga-DOTATATE on a lesion basis and comparable diagnostic accuracy on a patient basis (24). The inconclusive results on this issue reported in the literature possibly reflect the particular receptor configuration of the individual tumors and the lack of internationally recognized criteria for SSR PET interpretation.
On the basis of the demonstrated superiority of 68Ga-DOTATATE PET/CT imaging compared with 111In-octreotide, the U.S. Food and Drug Administration has approved 68Ga-DOTATATE for localization of SSR-positive neuroendocrine tumors in adult and pediatric patients.
Technique
The potential benefits of withdrawal of SSA treatment, or at least of scanning patients at the end of the coverage period of the analog, is still under debate, and no international consensus has been reached. If discontinuation is clinically feasible and performed, short-acting analogs should be stopped for at least 48 h and long-acting formulations for 4–6 wk (16). Recent data investigating the impact of SSA on 68Ga-DOTATATE PET/CT in the same patients studied on and off treatment on 2 consecutive days do not support the need for discontinuation. The authors reported reduced uptake at physiologic sites with unchanged tumor uptake in the patients under treatment, resulting in higher image contrast (25). Since normal organ and tumor uptake tends to increase the later the PET scan occurs after SSA administration (26), and since rigorous data on timing are unavailable, many centers scan patients at the end of the SSA treatment cycle, if possible (e.g., before the subsequent SSA injection), otherwise maintaining the same interval from the SSA injection as in the previous scan.
According to the recent European Association of Nuclear Medicine guidelines and the U.S. Food and Drug Administration–approved label, the recommended activity to obtain good image quality is 2 MBq/kg of body weight (0.054 mCi/kg) up to 200 MBq (5.4 mCi), administered as an intravenous bolus injection.
68Ga-DOTATATE can be supplied either already labeled or as a kit to be reconstituted according to the manufacturer’s (Advanced Accelerator Applications) instructions (http://www.accessdata.fda.gov/drugsatfda_docs/label/2016/208547s000lbl.pdf).
Before injection, the radioactivity should be verified with a dose calibrator. Injected radioactivity should be within ±10% of the recommended dose.
Patients should be encouraged to drink a sufficient amount of water before tracer administration (e.g., 1 L, if tolerated, with or without oral contrast medium) and after tracer administration to increase image quality in the abdomen, and to void frequently.
The PET/CT acquisition typically begins 45–60 min after the intravenous administration of the radiopeptide and proceeds from the top of the skull to the mid thighs, preferably in a 3-dimensional mode. A detailed description of the scanning protocol and image reconstruction is provided in the European Association of Nuclear Medicine procedure guidelines for 68Ga-DOTA-peptides (16,27). The use of intravenous contrast medium may further enhance detection. However, in standard use, unenhanced PET/CT is considered sufficient.
Biodistribution
Clearance of 68Ga-DOTATATE from the blood is rapid. Dynamic PET studies demonstrated that arterial activity shows biexponential elimination, with no radioactive metabolites detected in serum or urine in the first 4 h. Radioactivity in the blood decreases to less than 5.3% of the peak level within 45 min of the dynamic scanning and to 2.2% at 195 min after injection. After 50 min, the accumulation in all organs plateaus, and maximal tumor activity accumulation is reached at 70 ± 20 min after injection (28). Excretion occurs almost exclusively via the kidneys.
Physiologic uptake is high in somatostatin receptor 2–rich organs such as the pituitary gland, spleen, adrenals, liver, pelvicalyceal system of the kidneys, and urinary bladder. Lower uptake may physiologically be observed in the thyroid, pancreatic head, stomach, small and large bowel, and prostate (Fig. 2) (29).
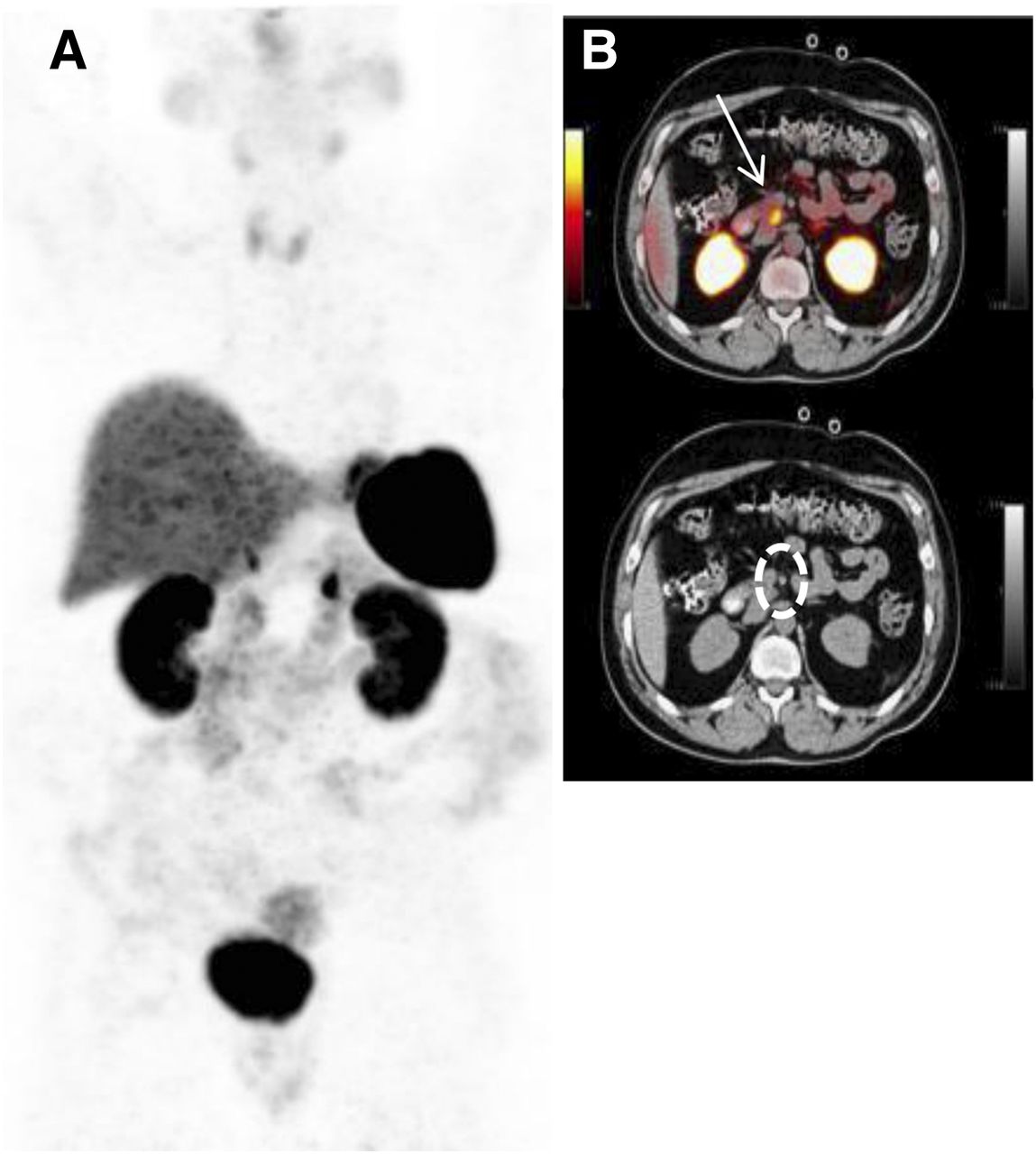
(A) Normal biodistribution of 68Ga-DOTATATE on volumetric (maximum-intensity-projection, MIP) image. (B) Axial PET/CT images showing physiologic intense uptake in pituitary, liver, spleen, kidneys, adrenals, and uncinate process of pancreas (arrow and oval outline) and variable degree of uptake in thyroid, intestine, and urinary bladder.
SUV has been demonstrated to correlate with receptor density up to values of approximately 25, corresponding to the steady-state inhibition constant value of 0.2 mL/cm3/min, after which the relationship is not linear. This may lead to underestimation of receptor expression (28).
Dosimetry
Estimated absorbed doses per injected activity for organs and tissues follow the biodistribution, peaking at 1, 2, and 3 h after injection in the spleen, followed by kidneys, and liver (Table 3). The highest absorbed doses are observed in the spleen and urinary bladder wall, followed by the kidneys, adrenals, and liver. The reported total effective dose was 0.021 ± 0.003 mSv/MBq (30).
Absorbed Doses of 68Ga-DOTATATE in Selected Organs
The effective radiation dose resulting from the administration of 185 MBq (5 mCi) to an adult weighing 75 kg is about 4.8 mSv (31). For this activity, the typical radiation dose to the critical organs, which are the urinary bladder wall, the spleen, and the kidneys, are about 0.125, 0.282, and 0.0921 mSv/MBq, respectively (31). Since the spleen has the highest physiologic uptake, higher uptake and dose to normal or tumor tissues may occur in patients with splenectomy, as demonstrated for 68Ga-DOTATOC (32). The effective dose deriving from the low-dose CT component is generally in the range of 9 mSv for 80-mA low-dose CT, whereas for 10-mA ultra-low-dose CT it is closer to 1 mSv.
Interpretation
Assessment of images should be guided by clinical information. As a general rule, besides areas of physiologic uptake, clearly outlined foci of uptake should be regarded as positive for SSR expression and thus considered to potentially represent NEN (Fig. 3 and Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). 68Ga-DOTATATE has certain limitations that have to be considered in order to adequately interpret the corresponding scans. There are alternative conditions that may exhibit increased SSR expression and, hence, represent potential sources of false-positives (Figs. 4 and 5 and Supplemental Fig. 2). These mainly include areas of inflammation or infection containing activated lymphocytes and macrophages, such as radiation pneumonitis, gastritis, sequelae of recent surgeries, reactive lymphadenopathy, and granulomatous lesions. For example, the thyroid generally exhibits low-grade uptake (SUVmax of 1.4–7.7, SUVmean of 3.0 (29)). More intense diffuse uptake could represent thyroiditis (due to the SSR-positive diffuse lymphocyte infiltration), whereas focal uptake could represent nodular disease (33). An area that requires careful consideration is the head of the pancreas, particularly the uncinate process, which may exhibit a variable physiologic uptake—focal or diffuse—of 68Ga-DOTATATE, related to the great concentration of pancreatic polypeptide cells (16). This represents a potential source of misinterpretation, since the pancreas and the duodenum are frequent sites of NENs. There have been attempts at defining an SUVmax threshold to distinguish benign from malignant pancreatic uptake of DOTA-SSA peptides (34,35). However, given the large overlap between benign/physiologic and malignant uptake and the large interscanner measurement variance, mere uptake should not be used to diagnose pancreatic NENs without the demonstration of a clear lesion on the companion CT image or at correlative diagnostic cross-sectional imaging (36). Other common non–NEN-related sources of uptake include accessory spleens or splenules, which could be erroneously interpreted as lymph nodes. If accessory spleens are sufficiently large, consideration of lesion attenuation and arterial-phase contrast behavior may be of assistance (Fig. 6).

Upstaging of patient with history of small intestine NEN and 6.5-cm lesion within right proximal femur with benign appearance at prior MRI. (A) DOTATATE maximum-intensity-projection image revealed multiple mesenteric and pelvic, as well as multiple unexpected osseous, metastases (arrows). (B) On axial PET/CT, the unexpected soft-tissue and bone metastases were detected in more detail (arrows). Intended treatment was converted from surgery and octreotide to surgery, octreotide, and selective radiotherapy of bone metastases. (Adapted from (66).)
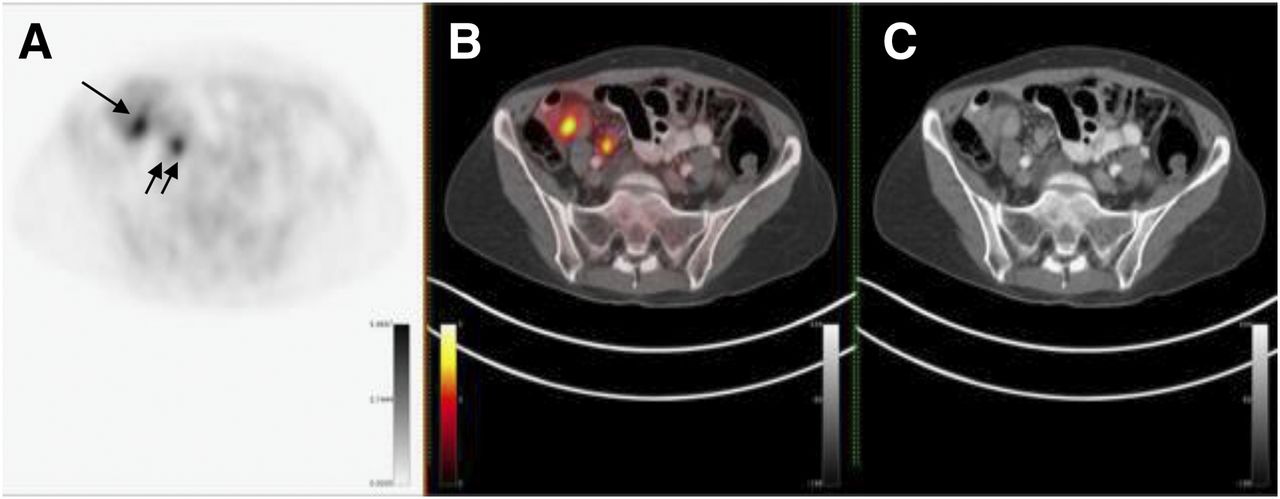
Patient with ileal neuroendocrine tumor (single arrow) who showed additional focal 68Ga-DOTATATE uptake (doubled arrow) in pelvis on imaging. Shown are axial PET (A), PET/CT (B), and CT (C) images. PET/CT images clarified this finding as physiologic uptake in right ureter.

Increased 68Ga-DOTATATE prostatic uptake. Shown are axial PET (A), PET/CT (B), and CT (C) images. Patient had known benign prostatic hyperplasia, and corresponding uptake is therefore non–tumor-specific.

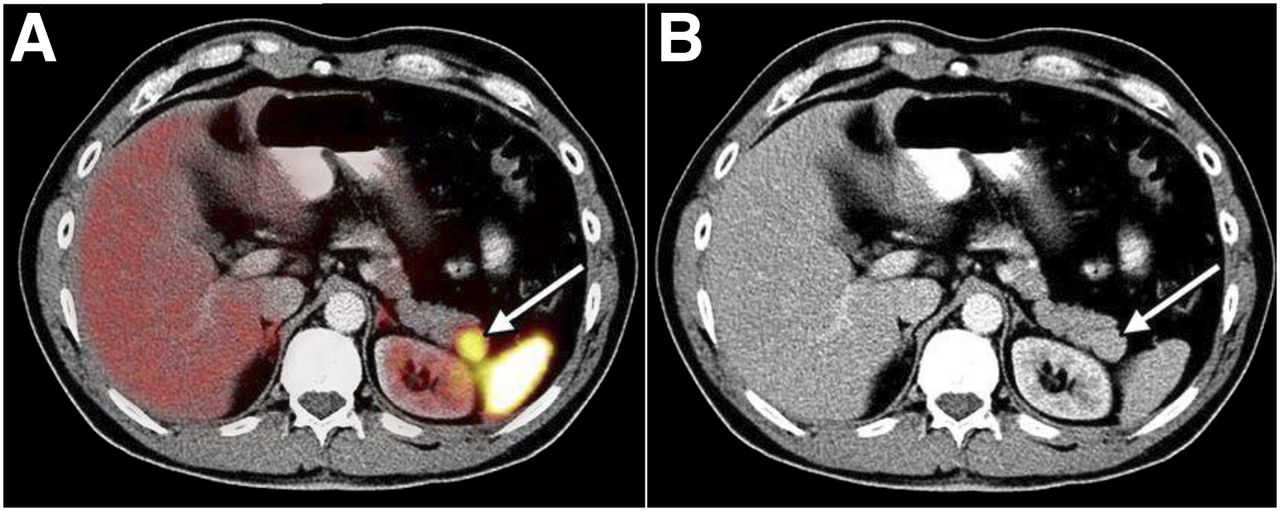
Patient with repeated flushing who underwent 68Ga-DOTATATE PET/CT. Shown are axial PET/CT (A) and CT (B) images. Focal uptake (arrow) in pancreatic tail was characterized on the basis of clinical data and MRI, indicating presence of splenule abutting tail of pancreas. (Reprinted from (47).).
Prolonged therapy with cold SSA may reduce the background physiologic uptake to the spleen and liver.
False-negatives are most commonly related to lesion size (spatial resolution is around 5.5–7 mm, with potential additional detrimental effects due to partial-volume effect, Fig. 7), recent analog therapy (although this issue is debated), alteration of receptor expression by recent chemotherapy, or truly receptor-negative disease (e.g., benign insulinomas and high-grade NENs). In the case of high-grade tumors, correlation with 18F-FDG PET/CT may be useful. High physiologic uptake as previously described in organs such as the spleen, liver, adrenals, pituitary gland; in the pelvicalyceal system of the kidneys and urinary bladder; and to a lesser degree in the thyroid, pancreatic head, stomach, small and large bowel, and prostate can mask isointense or slight pathologic somatostatin receptor 2 expression.

60-y-old woman who had previously undergone ileal neuroendocrine tumor resection, was currently on SSA with associated cholelithiasis, and was scheduled for surgery. Before surgery, 68Ga-DOTATATE PET/CT (volumetric image [A] and axial [B]) and chromogranin A (D, blue circles) were negative. However, circulating neuroendocrine transcript levels (red circles) were positive. Positive transcript levels indicate presence of primary, residual, or metastatic neuroendocrine tumor. At cholecystectomy, there was no evidence of hepatic metastases. Random intraoperative hepatic needle biopsy, however, demonstrated presence of neuroendocrine tumor metastases. (C) Axial CT scan showing cholelithiasis (solid arrow) and simple hepatic cyst (dashed arrow).
Clinical Value
68Ga-DOTA-peptide PET/CT is the gold standard functional imaging modality to study well-differentiated NENs in Europe and is included in European guidelines (16). Over the past decade, many reports have demonstrated the superiority of SSR PET/CT (with 68Ga-DOTATATE, 68Ga-DOTATOC, or 68Ga-DOTANOC) over single-photon scintigraphy (including SPECT/CT), morphologic imaging (CT/MRI), or PET/CT with other radiopharmaceuticals (16,19,20,37–41). In a recent prospective trial including 131 patients with gastroenteropancreatic NENs and unknown primary NENs, 68Ga-DOTATATE showed a higher detection rate (95.2%) than 111In-pentetreotide SPECT/CT (30.9%) or CT or MRI (45.6%) (42).
The largest single study specifically addressing 68Ga-DOTATATE diagnostic accuracy in NENs (39) was retrospective and included 728 patients and 1,258 PET/CT scans. 68Ga-DOTATATE PET/CT showed high sensitivity (>94%) and specificity (>92%) for NEN lesion localization, with the highest accuracy being for primary midgut tumors. The results of that study are in line with those of much smaller previous studies using PET/CT with either 68Ga-DOTATOC or 68Ga-DOTANOC (16,20,43–46). Overall, SSR PET/CT showed a high accuracy (≥96%) for the detection of well-differentiated NENs at either the primary site or the metastatic sites (mostly lymph nodes, liver, bone, and lung) (20,39,44).
Current guidelines indicate the high diagnostic accuracy of SSR PET/CT for detection of disease extension (at both staging and restaging), identification of the unknown primary site, and selection of candidates for PRRT (16).
The role of PET/CT for the assessment of tumor response to treatment is still under debate since a reduction of uptake can indicate a reduction of tumor volume (and of receptor number) but cannot exclude the presence of undifferentiated clones that may be SSR-negative. Considering the fact that SSR PET/CT positivity predicts the localization of cold and radiolabeled SSA-based treatment options, it is evident that the clinical impact of 68Ga-DOTATATE lies not merely in better diagnostic accuracy but also in better therapeutic management with cold SSA or PRRT.
A recently published systematic review (47) (including data from 1,561 patients) reported an overall change in management in 44% (range, 16%–71%) after 68Ga-SSA PET/CT (with either 68Ga-DOTATOC, 68Ga-DOTATATE, or 68Ga-DOTANOC). About half of these cases were provided by a single study using 68Ga-DOTATATE (728/1,561, or 47%) (39). In that study, Skoura et al. found that the treatment plan was changed in 40.9% (515/1,278) of the 68Ga-DOTATATE PET/CT cases because of new, unexpected findings. In most cases, the new treatment comprised chemotherapy or PRRT (362/515, or 70.3%), whereas less frequent options included surgery (after detection or confirmation of the NEN primary site, 52/515, or 10.1%) and second-line chemotherapy (71/515, or 13.8%). Less common management changes included ongoing-treatment discontinuation (2/515), rejection of PRRT (2/515), and selection of liver transplant candidates by excluding extrahepatic disease (2/515). Previous reports on smaller patient populations reported similar findings (42).
68Ga-SSA PET/CT has also been demonstrated to provide relevant prognostic information: since the intensity of uptake is an indirect measure of tumor differentiation, higher uptake correlated with a better prognosis (48).
The role of 68Ga-SSA PET/CT in G3 NENs is debated. By definition, G3 includes poorly differentiated tumors. However, especially in the subgroup with a Ki-67 of 20%–50%, the clinical behavior is more similar to G2 tumors. In this setting, a complementary role with 18F-FDG can therefore be envisioned. Vice versa, 68Ga-SSA PET/CT in cases presenting higher Ki-67 values (>50%), even if positive, will likely not affect management.
The added value of 18F-FDG in well-differentiated NENs (G1 and G2) is still under debate, and no international consensus has been reached (49–53).
According to current evidence, it is not routinely recommended that 18F-FDG should have a role in G1 NENs (a role in which its use could be considered only in selected cases when a specific clinical indication or suspicion is present), whereas 18F-FDG may have a clinical role in G2 NENs, especially for higher Ki-67 values, based on clinical indications (e.g., patients with CT progression or with SSR PET/CT-negative lesions). Recently, it was in fact shown that 18F-FDG PET/CT should be used only in selected cases, with a Ki-67 of less than 12% (53), as in such cases the clinical management uniquely relies on 68Ga-DOTATATE.
Current European Neuroendocrine Tumor Society guidelines (54) indicate a potential role for 18F-FDG only for the G3 group, when surgery is indicated. Several studies, mostly retrospective, investigated the role of combination of 68Ga-SSA PET/CT and 18F-FDG PET/CT in NENs. However, they were hampered by a small patient population and by the heterogeneity of the tumor primary site (a well-known factor affecting 18F-FDG positivity). In a recent multinational, multidisciplinary Delphi consensus meeting of NEN experts (n = 33) (55), 18F-FDG PET/CT was considered valuable for differentiating high- from low-grade tumors and for its prognostic implications. No consensus, however, was reached regarding combining 18F-FDG and 68Ga-SSA PET/CT or their timing in a diagnostic setting.
A combined imaging modality to achieve a complete biologic characterization defining a more aggressive behavior is appealing. In fact, the mere detection of a higher number of lesions or even the detection of 18F-FDG positivity is not necessarily associated with a different management in all cases or in all nuclear medicine or oncology departments. However, there is international consensus on the fact that 18F-FDG positivity correlates with a worse prognosis (56), but the treatment strategies to be implemented in 18F-FDG–positive cases are not standardized. The rationale for using 18F-FDG relies on its ability to identify the presence of aggressive disease foci—an ability that may turn into a better stratification of patients at major risk of progression. The clinical scenario of double-tracer imaging findings ranges from purely SSR-positive/18F-FDG–negative cases to 18F-FDG–positive/SSR-negative cases, with a very heterogeneous intermediate group presenting various patterns of uptake in the same patient with both tracers in the same or in different lesions over time (52). The most important lesson deriving from these studies is the demonstration of the heterogeneous nature of NENs.
SSR imaging is used to select patients for PRRT. Although the criteria are well defined and validated for 111In-pentetreotide with the 4-point Krenning scale, which is based on relative tumor uptake compared with uptake by normal organs (liver, kidneys, and spleen, where grade 1 is uptake less than liver [liver excluded], grade 2 is uptake equal to liver, grade 3 is uptake greater than liver, and grade 4 is uptake much greater than kidneys and spleen) (4), there is no consensus on what should be considered sufficient uptake at 68Ga-SSA PET/CT. Some authors have reported SUVmax thresholds for PRRT enrollment based on retrospective analyses (e.g., an SUVmax of 17.9 (57) or 16.4 (58) for 68Ga-DOTATOC). However, this approach is hampered by the limited reproducibility of SUVmax across different scanners. More frequently in clinical practice, the Krenning scale is adapted to the volumetric 68Ga-SSA PET/CT image, and lesion uptake greater than liver is considered suitable for PRRT.
Integration Within the Diagnostic Algorithm of NENs
Biomarkers are a viable adjunct to image interpretation. The secretory activity of NENs is quantifiable and facilitates their detection. Previously, chromogranin A was considered useful, but rigorous assessment over the last decade has led to decreased enthusiasm about its use, because of normal levels in about 30%–40% of NENs and falsely elevated levels in patients with renal failure, cardiac disease, or proton pump inhibitor therapy (59). Moreover, alterations in circulating chromogranin A levels are often nonconcordant with imaging, and prospective studies have not confirmed a role for chromogranin A in predicting or defining progression (55). To better reflect not only the mere secretory activity but also the complex biologic activities of an evolving neoplasm (cell proliferation, growth factor signaling, and others) that constitute the hallmarks of cancer, and to provide more relevant information on tumor behavior, new approaches have been introduced, including whole-genome sequencing, circulating micro-RNA, and tumor transcripts (60). Evaluation of circulating messenger RNA (transcript analysis) has provided information on disease status that is of substantial clinical utility in the management of NENs (61,62). This strategy uses simultaneous polymerase chain reaction–based analyses of multiple neuroendocrine tumor genes measurable in the blood and algorhythmic transformation into a mathematic index of disease activity (60,63). NEN gene blood levels correlated with 68Ga-DOTA-SSA PET/CT imaging and could define disease status (64).
Current imaging strategies and biomarkers in NEN management addressed at a recent Delphi consensus meeting of NEN experts (55) indicated agreement on the use of CT or MRI in conjunction with functional imaging. Because of its synergistic value, 68Ga-DOTATATE is often used in addition to morphologic imaging modalities such as CT and MRI. PET/CT scanners are widely available, and the corresponding CT, if performed with diagnostic quality and contrast medium, may improve the diagnostic accuracy, particularly in organs with high physiologic 68Ga-DOTATATE uptake and in the lungs. Especially, gastroenteropancreatic NENs are well suited for dedicated PET/MRI, as MRI adds important information to the detection of abdominal lesions, particularly in the liver (Supplemental Fig. 3) (65,66), whereas CT remains superior for the detection and characterization of lung lesions. As discussed, 18F-FDG detects dedifferentiated lesions expressing no or little somatostatin receptor 2 (54). A common indication for 18F-FDG PET/CT is morphologically growing lesions with a discordant 68Ga-DOTATATE finding.
These observations are worthy of further clinical study to provide evidence that the interface of imaging and circulating molecular indices of tumor evolution is likely to enhance dynamic assessment of tumor status.
CONCLUSION
68Ga-DOTA-peptide PET/CT has significantly advanced the approach to NENs. Its widespread implementation is based on its proven clinical utility and facilitation of clinical management. Overall, it represents the gold standard functional imaging modality for the assessment of well-differentiated NENs in conjunction with anatomic imaging (CT or MRI). An unmet need is the evaluation of the clinical impact of the dual-approach 18F-FDG and 68Ga-SSA PET/CT in the decision-making algorithm, given the numerous indications from the literature of the prognostic impact of 18F-FDG avidity in terms of overall and treatment-specific survival. A further significant advance needed is the development of an accurate, personalized interpretation of the individual disease status. This personalization may be accomplished by an algorithmic integration of the clinical, histopathologic, imaging, and molecular information available for the neoplasm of each subject.
Footnotes
Published online Aug. 17, 2017.
Learning Objectives: On successful completion of this activity, participants should be able to describe (1) the role of 68Ga-DOTATATE in neuroendocrine tumor management, (2) the interpretation of 68Ga-DOTATATE PET/CT images, and (3) the integration of 68Ga-DOTATATE PET/CT in the diagnostic and management algorithm for neuroendocrine tumors.
Financial Disclosure: Dr. Bodei is a consultant/advisor for Ipsen and AAA Pharmaceutical, and Dr. Herrmann is a consultant/advisor for Ipsen, Curium, and Sofie Biosciences and an investigator for AAA Pharmaceutical. The authors of this article have indicated no other relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA category 1 credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through November 2020.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 8, 2017.
- Accepted for publication July 27, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging Pathway of a Pediatric Patient with Succinate Dehydrogenase B-Deficient Paraganglioma
- Practical Considerations for Implementation of 177Lu-DOTATATE Neuroendocrine Tumor Treatment Programs
- The Future of Nuclear Medicine as an Independent Specialty
- SSTR-RADS Version 1.0 as a Reporting System for SSTR PET Imaging and Selection of Potential PRRT Candidates: A Proposed Standardization Framework
- Aetna and 68Ga-DOTATATE: A Sequel to "The Injustice of Being Judged by the Errors of Others" (1)