


Abstract
Patients with von Hippel–Lindau disease (VHL) are at risk to develop multiple tumors. The growth of lesions is unpredictable, and regular surveillance is critical for early treatment to control local damage. Vascular endothelial growth factor A (VEGF-A) produced locally is supposed to play an important role in development of disease manifestations and is a target for antiangiogenic therapy with the monoclonal antibody bevacizumab. We aimed to assess whether VHL manifestations can be visualized with 89Zr-bevacizumab PET and to explore whether 89Zr-bevacizumab PET can differentiate progressive from nonprogressive lesions. Methods: VHL patients with at least 1 measurable hemangioblastoma were eligible. 89Zr-bevacizumab (37 MBq) was administered intravenously 4 d before the scan. Maximum standardized uptake values were calculated. PET scans were fused with routine MRI of the central nervous system and abdominal MRI or CT. Progressive lesions were defined as new lesions, lesions that became symptomatic, and lesions ≥ 10 mm that increased ≥ 10% and ≥ 4 mm on repeated anatomic imaging within 12 mo. Results: Twenty-two patients were enrolled. At baseline, anatomic imaging showed 311 lesions. 89Zr-bevacizumab PET visualized 59 VHL manifestations, 0–17 per patient. The median of maximum standardized uptake values was 8.5 (range, 1.3–35.8). The detection rate for lesions ≥ 10 mm was 30.8%. Seven additional hotspots without substrate on baseline anatomic imaging were found; 2 were also detected with anatomic imaging during follow-up. Nine of 25 progressive lesions were visible on PET and 27 of 175 nonprogressive lesions, corresponding to a positive predictive value of 25% and a negative predictive value of 90%. SUVmax was similar in progressive and nonprogressive lesions (median, 4.8; range, 0.9–8.9 vs. median, 6.7; range, 1.3–35.8, P = 0.14). Conclusion: VHL manifestations can be visualized with 89Zr-bevacizumab PET with a striking heterogeneity in tracer accumulation. 89Zr-bevacizumab uptake does not predict progression within 12 mo. In one third of the lesions, the drug target VEGF is available and accessible. 89Zr-bevacizumab PET might offer a tool to select VHL patients for anti-VEGF therapy.
- von Hippel-Lindau disease
- hemangioblastoma
- positron emission tomography
- vascular endothelial growth factor
- bevacizumab
von Hippel–Lindau (VHL) disease is an autosomal-dominant inherited tumor syndrome caused by an inactivating germline mutation in the VHL gene, located on chromosome 3p25. The estimated prevalence is 2–3 per 100,000 (1,2). Inactivation or loss of the wild-type VHL allele results in disease manifestations. Lack of functional VHL protein induces intracellular accumulation of the transcription factor hypoxia-inducible factor 1α, activating cellular survival strategies for hypoxic circumstances by angiogenesis via proangiogenic growth factors including vascular endothelial growth factor A (VEGF-A). The main VHL disease manifestations are hemangioblastomas, retinal angiomas, renal cell carcinomas, pancreatic neuroendocrine tumors, pheochromocytomas, middle ear endolymphatic sac tumors, and cysts in the kidneys, pancreas, epididymis, and broad ligament. VHL mutation carriers often develop multiple disease manifestations that can severely affect quality of life. Moreover, patients with VHL disease have a shorter life expectancy (3).
Guidelines for screening and surveillance of existing lesions advise frequent imaging, ocular examination, and blood and urine examination (4,5). There is no validated tool that predicts the progression of disease manifestations. Hemangioblastomas are often dormant for years but can suddenly start growing; 72% grow in a saltatory pattern (6,7). Hemangioblastoma growth is associated with location in the brain stem and cerebellum, male sex, and a cystic component (6). Local concentrations of growth factor VEGF-A may provide predictive information on biologic behavior of VHL-associated lesions. Early identification of progressive lesions allows timely local treatment. Furthermore, different drugs are available to target the VEGF-A pathway at the growth factor level as well as at the receptor level. We developed the PET tracer 89Zr-bevacizumab that binds VEGF-A and enables noninvasive whole-body imaging and quantification. In patients with sporadic metastatic renal cell carcinoma, 89Zr-bevacizumab PET visualized tumor lesions including brain metastases, illustrating that the radioactive tracer can cross the blood–brain barrier (8).
The aim of the present feasibility study was to assess whether VHL-associated lesions can be visualized with 89Zr-bevacizumab PET and whether 89Zr-bevacizumab PET can differentiate progressive from nonprogressive lesions.
MATERIALS AND METHODS
Patients
Patients were recruited from the University Medical Centers in Groningen and Utrecht. Eligibility criteria included genetically proven VHL disease or clinically proven VHL disease (4), age ≥ 18 y, participation in a surveillance program, and at least 1 measurable lesion located in the central nervous system (CNS). Pregnant patients were excluded. Treatment for VHL disease manifestations was recorded up to 12 mo after 89Zr-bevacizumab PET imaging. The study was approved by the institutional review board (http://www.clinicaltrials.gov NCT00970970). All patients gave written informed consent.
89Zr-Bevacizumab PET
PET scans were obtained at the University Medical Center Groningen. Conjugation and labeling of bevacizumab (25 mg/mL; Roche) with 89Zr was performed as described (9). Whole-body PET images were acquired on a Biograph mCT (PET/CT 64 slices; Siemens) scanner from the upper legs to head in 6–8 bed positions of 5-min acquisition time each. Administration of 37 MBq of 89Zr provides a resolution of approximately 10 mm on PET and reconstruction settings used. The first 3 patients underwent PET scans at 1 h, 2 d, and 4 d after intravenous administration of 89Zr-bevacizumab (37 MBq, protein dose of 5 mg). The optimal scan timing with the highest lesion-to-background ratio was day 4. The next patients underwent PET scanning 4 d after 89Zr-bevacizumab administration.
Standard Screening and Surveillance
Patients underwent MRI of the CNS within 6 wk before 89Zr-bevacizumab PET and abdominal CT or MRI within 3 mo before or after 89Zr-bevacizumab PET. Follow-up anatomic imaging was performed within 12 mo of initial surveillance. MR images were acquired with a 1.5-T scanner in T1- and T2-weighted sequences, with and without intravenous administration of a gadolinium-containing contrast agent. The reconstruction interval varied between 1 and 5 mm for CNS and between 1.5 and 5 mm for abdominal imaging. CT scans were acquired with a multidetector scanner, before and after intravenous administration of an iodine-containing contrast agent, with a maximum slice thickness of 5.0 mm. CNS and abdominal imaging were centrally reviewed by 2 radiologists. Morphologic aspect (cystic, solid, mixed) and maximal lesion diameters were recorded.
Imaging Analysis
The 89Zr-bevacizumab PET scans were fused with baseline MRI or CT scans using SyngoMMWP VE50A software (Siemens AG) to verify substrate for hot spots. Tracer uptake was quantified by calculating SUVmean and SUVmax for PET-positive VHL-associated lesions and healthy organs with AMIDE Medical Image Data Examiner software (version 0.9.1; Stanford University) by drawing 3-dimensional regions of interest (10). Quantification of 89Zr-bevacizumab distribution revealed a strong correlation between SUVmax and SUVmean for normal organs (r = 0.99, P < 0.01) and VHL disease manifestations (r = 0.97, P < 0.01, Supplemental Fig. 1 [supplemental materials are available at http://jnm.snmjournals.org]). SUVmax is less operator dependent and therefore reported. Given the resolution of 89Zr-bevacizumab PET, we did a subanalysis of lesions ≥ 10 mm.
For all lesions visualized on baseline CT/MRI except simple renal and pancreatic cysts, progression was recorded and compared with 89Zr-bevacizumab PET. Because a definition for progression of VHL manifestations and information on variability of measurements on repeated imaging are lacking, we took a conservative approach based on variability of lung tumor CT measurements (11). We considered lesions with a longest diameter of ≥ 10 mm that increased ≥ 10% and an absolute growth of ≥ 4 mm progressive, as well as new lesions visualized on the follow-up scan and lesions that became symptomatic.
Plasma VEGF-A
Before each 89Zr-bevacizumab administration, a blood sample was obtained by peripheral vena puncture, using a tourniquet. Blood was collected in sterile 10-mL ethylenediaminetetraacetic acid tubes. Within 30 min of collection, ethylenediaminetetraacetic acid blood was centrifuged at 120g for 30 min at 4°C. After collection of 0.25 mL of platelet-rich plasma, the leftover was centrifuged again at 2,500g for 10 min at room temperature to obtain platelet-poor plasma. Plasma sample aliquots were stored at −80°C. VEGF-A was determined in platelet-poor plasma in duplicate using the Quantikine enzyme-linked immunosorbent assay kit (R&D Systems) according to the manufacturer’s instructions. The mean of the duplicates was used for calculations. Plasma VEGF-A was compared with 89Zr-bevacizumab PET results.
Statistical Analysis
The primary endpoint was the detection rate of 89Zr-bevacizumab PET for VHL disease manifestations. Spearman rank correlations served to calculate correlations. For comparison of unpaired data the Mann–Whitney test was used, and for paired data the Wilcoxon signed-rank test was used. Differences in PET positivity rate between progressive and nonprogressive lesions were tested using the Fisher exact test. A P value of less than 0.05 was considered statistically significant. Analyses were performed with SPSS (version 20; IBM) and GraphPad Prism (version 5.00; GraphPad Prism Inc.).
RESULTS
Patient Characteristics
Between November 2009 and April 2012, 13 male and 9 female patients were included (median age, 42 y; range, 23–66 y) (patient characteristics are shown in Table 1).
Patient Characteristics
Routine Anatomic Imaging
Three hundred eleven VHL disease manifestations other than simple renal and pancreatic cysts were identified on baseline MRI and CT, with a median of 7 per patient (range, 1–102) (Tables 2 and 3). In total, 139 lesions were ≥ 10 mm. Furthermore, 130 simple cysts ≥ 5 mm were detected in the kidneys (range, 0–46 per patient) and 126 in the pancreas (range, 0–30).
VHL Disease Manifestations on Routine Imaging and on 89Zr-Bevacizumab PET Per Patient
VHL Disease Manifestations* on Routine Imaging and on 89Zr-Bevacizumab PET Per Organ
89Zr-Bevacizumab PET
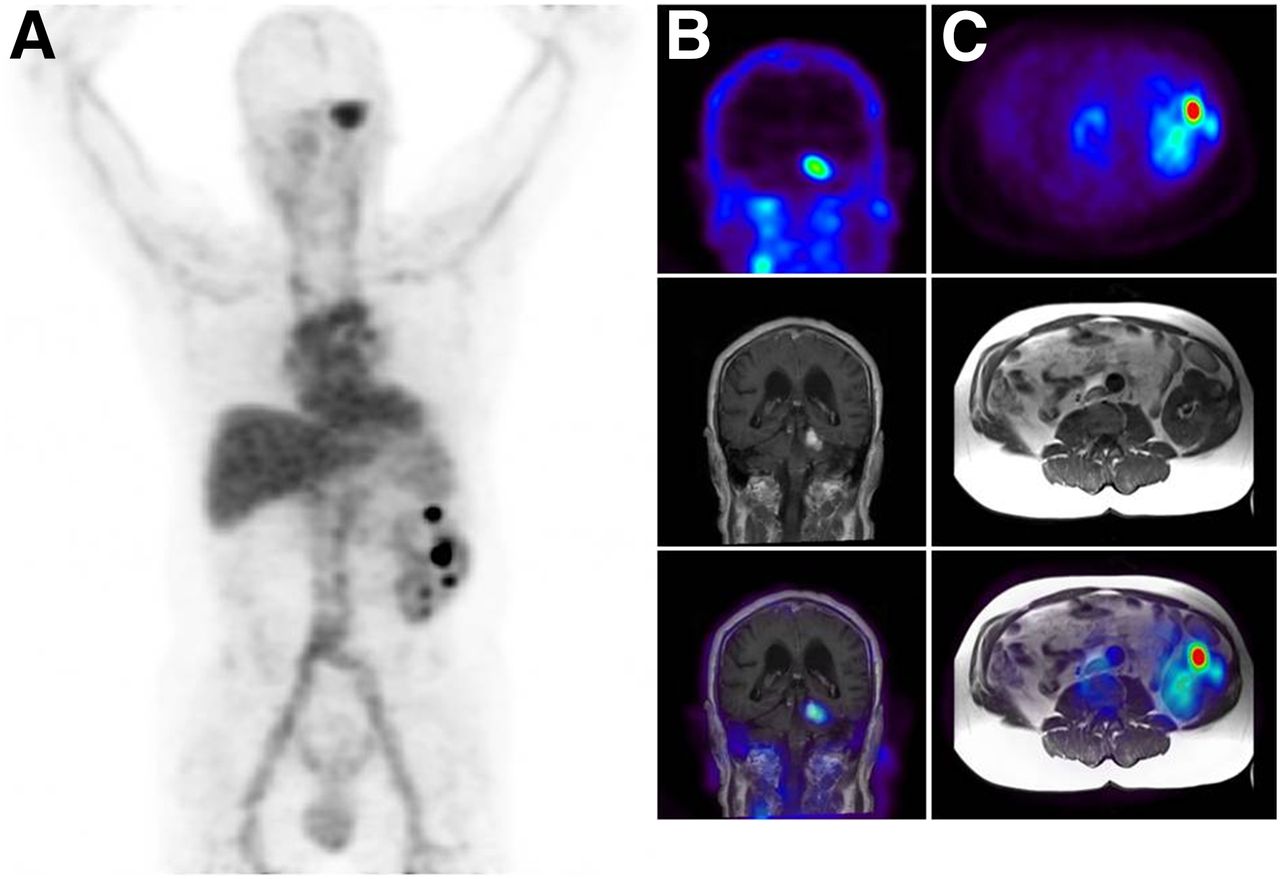
89Zr-bevacizumab PET visualized 59 VHL disease manifestations, 0–17 per patient (median, 1) (Fig. 1; Tables 2 and 3). Fifty of these 59 PET-positive VHL lesions had a solid, 6 a cystic, and 2 a mixed appearance on anatomic imaging, and 1 lesion could not be classified. No 89Zr-bevacizumab accumulation in simple renal and pancreatic cysts was demonstrated; 33 simple renal cysts appeared as cold spots.
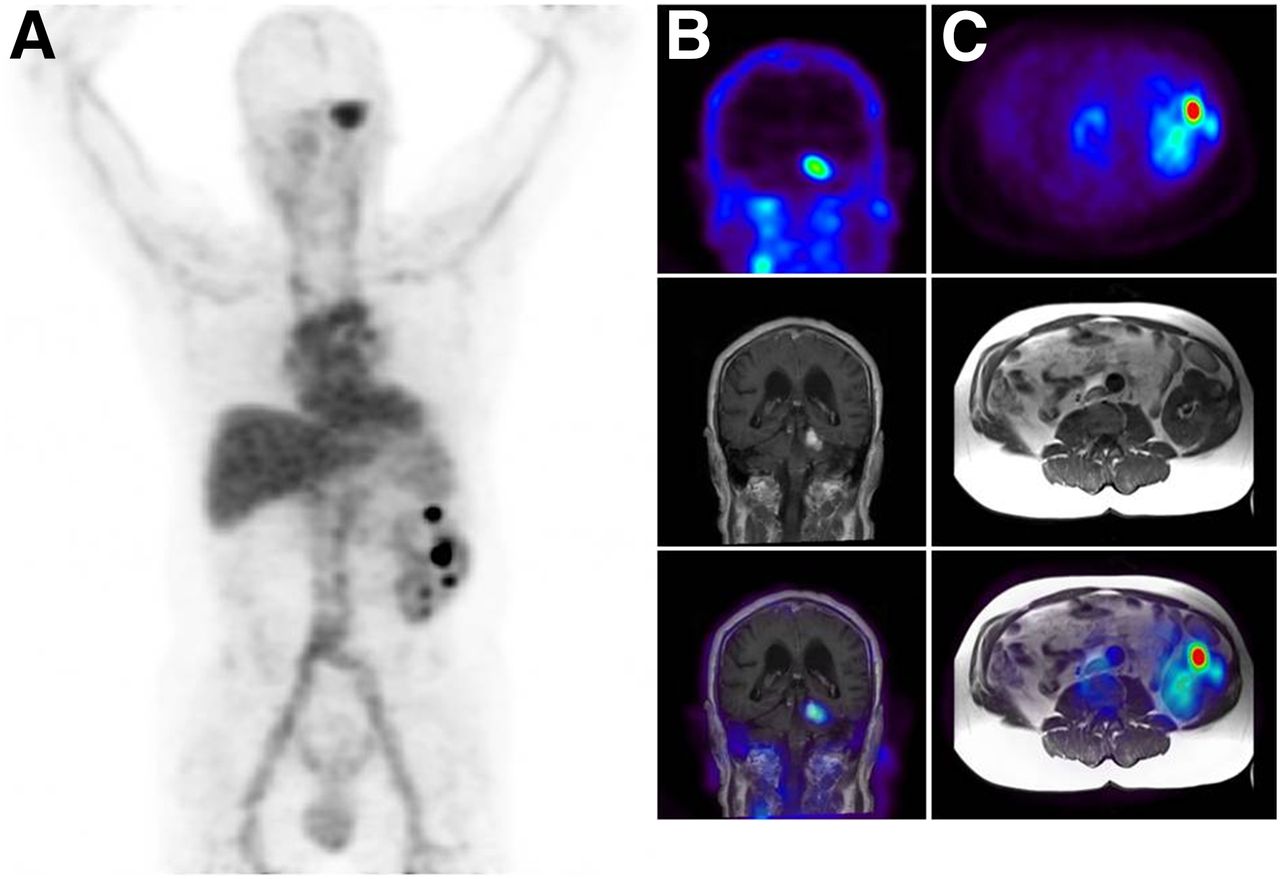
(A) 89Zr-bevacizumab PET scan (maximum-intensity projection) of patient 4, demonstrating normal antibody distribution with tracer uptake in blood pool and liver as well as uptake in a hemangioblastoma in cerebellum (SUVmax, 8.3) and in 6 solid kidney lesions (SUVmax, 6.6–27.6). (B) Hemangioblastoma visualized on coronal 89Zr-bevacizumab PET, MR, and fusion images (top, middle, and bottom, respectively). (C) Kidney lesion visualized on transversal 89Zr-bevacizumab PET, MR, and fusion images (top, middle, and bottom, respectively).
The PET scan demonstrated 7 additional hot spots in 5 different organs without substrate on anatomic imaging. Two lesions (cerebellum, adrenal gland) were detected during follow-up on anatomic imaging.
Overall, 44 of 139 VHL disease manifestations ≥ 10 mm (30.8%) were identified on 89Zr-bevacizumab PET. The detection rate of hemangioblastomas ≥ 10 mm was 16 of 29 (55%). Figure 2 shows SUVmax and the proportion of PET-positive lesions ≥ 10 mm for the different germline mutations.
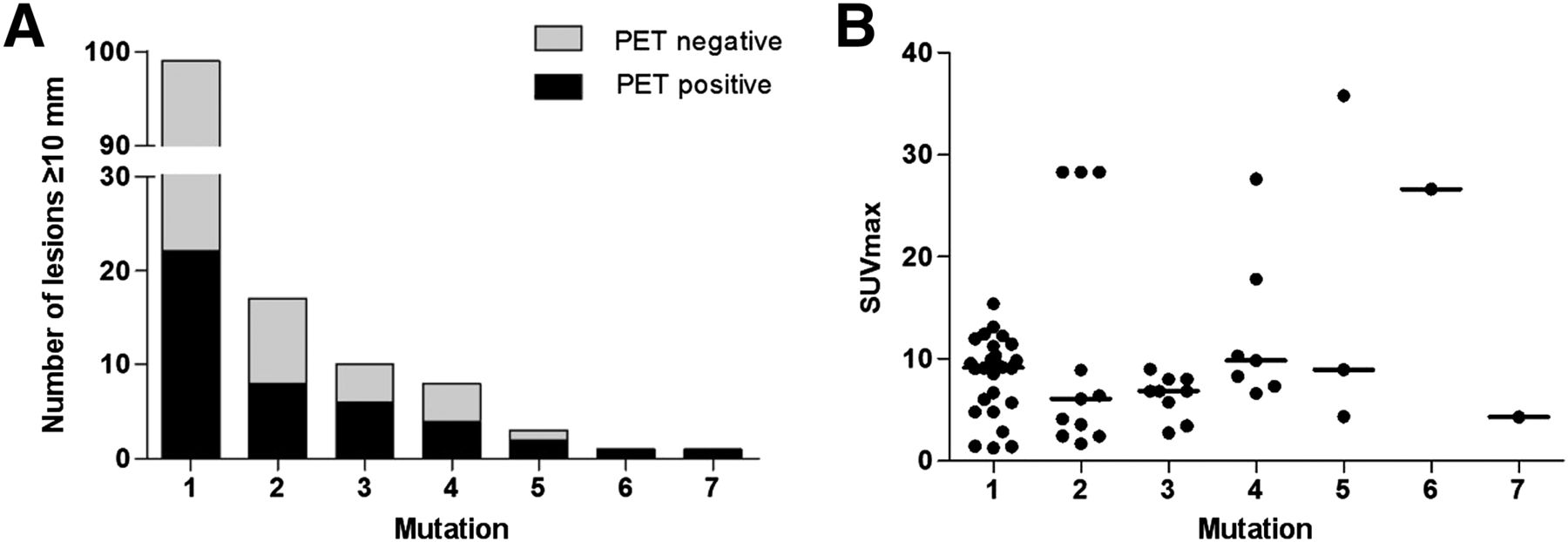
Number of PET-positive VHL disease manifestations ≥ 10 mm according to germline mutation (A) and SUVmax (B): 1 = c.-89-?_c.297+?del, 2 = c.500G > A, 3 = c.490C > T, 4 = c.509T > A, 5 = c.340 + 1G > A, 6 = c.241C > T, 7 = IVS1-59del46.
Normal-organ distribution of 89Zr-bevacizumab was similar as described earlier (Fig. 3A) (8,12). Median SUVmax of VHL disease manifestations was 8.5 (range, 1.3–35.8), with higher tracer uptake in kidney lesions (n = 12; median SUVmax, 22.2; range, 6.6–35.8) than in CNS lesions (n = 24; median SUVmax, 4.5; range, 1.3–8.9; P < 0.0001; Fig. 3B). However, because of the low normal-organ background in the CNS, the lesion-to-background ratio (median, 8.6; range, 1.9–25.3) was excellent for hemangioblastomas and even higher than for kidney lesions (median, 5.0; range, 2.0–11.5; P = 0.049).

Quantification (median with range) of 89Zr-bevacizumab distribution in 22 patients with VHL disease in normal organs and 59 disease manifestations (A) and in VHL disease manifestations according to localization (B).
Progressive Lesions
Repeated abdominal imaging was available in 19 patients at a median of 349 d after baseline (range, 196–642 d); repeated CNS imaging was available in 20 patients at a median of 319 d after baseline (range, 90–540 d). Out of 200 evaluable lesions, 25 were progressive (21 hemangioblastomas and 4 renal cell carcinomas).
89Zr-bevacizumab PET visualized 9 of 25 (36%) progressive lesions and 27 of 175 nonprogressive lesions (15%), resulting in a positive predictive value of 0.25 (95% confidence interval, 0.11–0.39) and a negative predictive value of 0.90 (95% confidence interval, 0.86–0.95). The detection rate of 89Zr-bevacizumab PET was significantly higher for progressive lesions than nonprogressive lesions (P = 0.022). However, progressive and nonprogressive lesions had a similar SUVmax (median, 4.8; range, 0.9–8.9, vs. median, 6.7; range, 1.3–35.8; P = 0.14). When this analysis was limited to hemangioblastomas, again a significantly higher PET detection rate for progressive (9/21 [43%]) than nonprogressive hemangioblastomas (15/148 [10%]) was found (P = 0.001). To explore whether the difference in detection rate could be explained by a difference in size between progressive and nonprogressive lesions, we further limited the analysis to hemangioblastomas ≥ 10 mm and found no difference in detection rate (P = 0.71).
Treatment
In the first year of follow-up, 8 patients were actively treated for VHL disease manifestations, and in 6 surveillance was intensified (Supplemental Table 1). Two patients received bevacizumab treatment. These patients are described in more detail in the supplemental data.
Plasma VEGF-A
Baseline plasma VEGF-A levels were available for all and follow-up levels for 14 of 22 patients. Median plasma VEGF-A was 23.9 pg/mL (range, undetectable–123.0) at baseline and 32.1 pg/mL (range, undetectable–259.7) at follow-up. No correlation was found between baseline plasma VEGF-A and the total number of VHL disease manifestations, the number of PET-positive lesions, SUVmax, or mean SUVmax. Furthermore, baseline and delta plasma VEGF-A did not differ between patients with progressive lesions and patients without progressive lesions.
DISCUSSION
To our knowledge, this is the first study demonstrating that VHL disease manifestations can be visualized with 89Zr-bevacizumab PET. The detection rate for lesions ≥ 10 mm was 30.8%. Despite the monogenetic pathogenesis, profound heterogeneity in tracer uptake by the lesions between and within patients was demonstrated, reflected by the finding of PET-positive and -negative lesions and by the range of SUVmax. 89Zr-bevacizumab PET did not identify lesions that progressed within the next year, nor did plasma VEGF-A levels.
Abundant VEGF expression has been demonstrated by in situ hybridization and immunohistochemistry in a variety of VHL-associated lesions (13–18). In contrast, VEGF messenger RNA was not detectable in normal brain (16) and was 3–13 times lower in normal kidney than in renal cell carcinoma (13). This corresponds with our imaging data that show virtually no 89Zr-bevacizumab accumulation in normal brain, intermediate uptake in normal kidney, and high uptake compared with normal surrounding tissue in one third of disease manifestations. The lesion detection rate was lower than in previous studies with 89Zr-bevacizumab PET in breast cancer and sporadic renal cell carcinoma patients but higher than in patients with neuroendocrine tumors (8,9,12). This may well represent different biology in relation to VEGF-A between these neoplasms. In the present study, there were 3 of 11 pancreatic lesions, which are probably neuroendocrine tumors, PET-positive. In addition, in a single patient only 16 of 80 liver metastases of a pancreatic neuroendocrine tumor were visible on PET. This is in line with our previous study in neuroendocrine tumor patients and highly influences the overall detection rate in the current study. Of the CNS lesions, 16 of 29 (55%) were PET-positive, which—although they are likely nonmalignant—closely resembles the detection rate we found for metastatic renal cell carcinoma. Interestingly, median SUVmax was numerically the highest in the current study, followed by the study in renal cell carcinoma, which is also characterized by loss of VHL and high VEGF-A expression. Median SUVmax was lowest in the primary breast cancer study (9), underscoring that these type of PET scans are more of value for characterization of lesions than in general for detection of lesions.
Accumulation of a radiolabeled antibody not only is determined by expression of the target, but also can be affected by perfusion and permeability of blood vessels, tumor interstitial pressure, and anatomic location (19). A small MRI study showed hyperperfusion and edema in hemangioblastomas, suggesting that vascular characteristics are not a likely cause of limited or no 89Zr-bevacizumab accumulation (20). CT in 66 sporadic clear cell renal cancer patients demonstrated lower blood flow, blood volume, and permeability surface area in primary tumors compared with normal renal cortex but with large SD, indicating heterogeneity (21). These perfusion parameters were correlated with microvessel density but not with VEGF staining. Future studies combining perfusion imaging with 89Zr-bevacizumab PET would enable determination of the role of vascular characteristics on antibody distribution.
In the present study, we did not perform biopsies to correlate imaging results with tissue VEGF-A concentration. However, in 9 melanoma patients and 23 breast cancer patients, radiolabeled bevacizumab uptake in the tumor correlated with tumor VEGF-A measurement by immunohistochemistry and enzyme-linked immunosorbent assay, respectively (9,22).
Heterogeneity in VEGF-A concentration in VHL manifestations between and within patients might be explained by different germline and second-hit mutations, resulting in variable preservation of the ability to degrade hypoxia-inducible factor 1α (23). The numbers of lesions in this study are too small to draw conclusions, but the results do not suggest important differences in the rate of PET-positive lesions or in SUVmax for different germline mutations.
In addition to being hypoxia-inducible-factor-dependent, VHL protein also has hypoxia-inducible-factor-independent functions such as stabilization of microtubules, regulation of apoptosis, regulation of extracellular matrix assembly, maintenance of primary cilium (23), and control of fibroblast growth factor receptor signaling (24). Loss of hypoxia-inducible-factor-independent functions probably contributes to the development of disease manifestations, including angiogenesis. In-depth genomic analysis of 4 synchronous renal cell carcinomas in a patient with VHL disease demonstrated different additional mutations per tumor (25). Therefore, intrapatient heterogeneity in 89Zr-bevacizumab uptake might reflect genomic heterogeneity. Whether additional mutations and mutational heterogeneity are prevalent in hemangioblastomas in VHL disease is unknown. However, sporadic hemangioblastomas are characterized by a low somatic mutation rate with exception of the VHL gene (26).
We found no difference in 89Zr-bevacizumab accumulation between progressive and nonprogressive disease manifestations ≥ 10 mm. This contrasts with a small study in 3 VHL patients in which the highest VEGF messenger RNA level was found in the patient with the most active disease (27). Moreover, in 50 patients with sporadic clear cell renal cell carcinoma who underwent nephrectomy, cytoplasmic VEGF expression correlated with tumor progression and grade (28).
Simple cysts in kidneys and pancreatic glands did not take up 89Zr-bevacizumab. Higher VEGF concentrations were detected in the fluid of 2 renal cysts than in serum of 1 VHL patient (29). Cyst formation may, however, be more dependent on loss of maintenance of the primary cilium than on activation of the VEGF pathway (30).
We did not find a relation between plasma VEGF-A levels and 89Zr-bevacizumab PET imaging results. Also the number of lesions and presence of symptomatic or growing lesions were not related with plasma VEGF-A. This is in line with earlier data (29) and may be explained by different VEGF-A splice variants in the circulation compared with the microenvironment of disease manifestations. The small variants, consisting of 121 and 165 amino acids (VEGF121 and VEGF165), are freely diffusible whereas the large variants VEGF189 and VEGF206 are bound to the extracellular matrix (31). Imaging with 89Zr-bevacizumab, binding to all splice variants potentially better reflects biology of disease manifestations than circulating VEGF-A.
VHL patients receive local treatment for symptomatic disease manifestations and lesions that pose a threat to functioning or have metastatic potential. There is no evidence-based systemic therapy available, but case reports and small studies have been reported for antiangiogenic treatment with bevacizumab (32–34), thalidomide (35,36), and the tyrosine kinase inhibitors semaxanib (37–41) and pazopanib (42). Study results for vatalanib and for bevacizumab are awaited (www.clinicaltrials.gov identifiers NTC00052013 and NTC01015300). Antiangiogenic therapy has resulted in improvement of symptoms and disease stabilization but rarely induces volume responses in hemangioblastomas. We treated 2 patients with bevacizumab plus interferon-α after participation in this study. One patient, who received bevacizumab plus interferon-α for metastatic renal cell carcinoma and hardly showed 89Zr-bevacizumab accumulation in the tumor, did not respond and died of rapidly progressive disease after 2 mo. The other patient was treated for multiple progressive unresectable hemangioblastomas with intense uptake on the 89Zr-bevacizumab PET scan. She experienced prolonged symptomatic improvement and a decrease in hemangioblastoma size. These cases suggest that 89Zr-bevacizumab PET might offer a tool to select patients for anti-VEGF therapy, but this needs further evaluation in future studies.
CONCLUSION
89Zr-bevacizumab PET can visualize different VHL disease manifestations but does not predict the behavior of a lesion. Striking heterogeneity between and within patients was found, reflecting different biology. Future studies are needed to assess whether 89Zr-bevacizumab PET can predict sensitivity to antiangiogenic treatment.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study was supported by a grant of the American VHL Family Alliance. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We are grateful to Dr. Ronald van Rheenen for his help with the supplemental videos.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication September 30, 2015.
- Accepted for publication January 15, 2016.





{kind=link}
{kind=link}
{kind=link}