


Abstract
The pronouncement of death is a determination of paramount social, legal, and ethical import. The novel construct of “brain death” was introduced 50 years ago, yet there persist gaps in understanding regarding this diagnosis on the part of medical caregivers and families. The tragic, much-publicized case of Jahi McMath typifies potential problems that can be encountered with this diagnosis and serves as an effective point of departure for discussion. This article recapitulates the historical development of brain death and the evolution of scintigraphic examinations as ancillary or confirmatory studies, emphasizing updated clinical and imaging practice guidelines and the current role of scintigraphy. The limitations of clinical and radionuclide studies are then reviewed. Finally, the article examines whether radionuclide examinations might be able to play an expanded role in the determination of brain death by improving accuracy and facilitating effective communication with family members.
The pronouncement of death is a determination of paramount social, legal, and ethical import. A new construct of “brain death” was promulgated by the Ad Hoc Committee of the Harvard Medical School some 50 years ago (1) and has seen international adoption (2–7), though not without a degree of ongoing controversy (8–12).
Physicians who care for severely ill patients require a working grasp of the concept of brain death. Reviews of the current medical literature periodically appear (13–16), and updated guidelines have been issued by professional societies (17–21). Despite these resources, surveys have repeatedly shown that many physicians exhibit a poor understanding of the underlying concepts (22,23) and that even carefully formulated practice guidelines are inconsistently adopted (7,24–26), indicating a persistent gap in knowledge and training (27,28). The topic of brain death has entered into the public’s consciousness, albeit in a distorted manner (29,30); physicians must therefore contend with families’ erroneous notions, which are based, at least in part, on inaccurate or sensational media reports (31).
A tragic contemporary case of brain death that has appeared in the news concerns a girl named Jahi McMath (32). This case highlights relevant issues and typifies potential problems that may arise, thereby serving as an effective nidus for discussion (33–35). Pertinent facts surrounding the McMath case have been summarized from prior publications and news reports.
JAHI MCMATH
Jahi McMath was 13 years old when she presented in late 2013 with symptoms of sleep apnea and underwent extensive resection of obstructing nasopharyngeal lymphatic and soft tissues. After a complicated postoperative course marked by hemorrhage and cardiac arrest, she was placed on a respirator. The hospital determined she was brain-dead and informed the family that her supportive therapy would be discontinued. The family vigorously contested this assertion, insisting that the hospital maintain Jahi on a ventilator on the basis of their belief that she would recover. An independent court-appointed medical expert confirmed that all medical criteria for brain death were met and Jahi was legally dead. At the family’s behest, an Alameda County Superior Court Judge repeatedly ruled that officials at Children’s Hospital Oakland maintain Jahi on a ventilator.
On December 30, 2013, the family appealed the brain death decision, insisting that the hospital continue life support until other arrangements could be made and arguing that applying the Uniform Determination of Death Act was a violation of Jahi’s constitutional religious and privacy rights. The hospital countered that because the brain death standard was fulfilled, it would be unethical to provide further medical care to the deceased. Ultimately, a solution to the impasse was reached by which Jahi’s body would be released by Children’s Hospital to the Alameda County coroner and then by the coroner to Jahi’s mother, all the while supported by artificial ventilation. Jahi was moved to an undisclosed location, where a tracheostomy was performed and a feeding tube inserted. Subsequent news reports (36) indicated that this location was New Jersey, where a patient’s representative may insist that death be legally determined only by the traditional cardiopulmonary definition. Jahi’s mother continues to maintain that Jahi is alive and responsive to verbal commands (37). The family’s attorney has argued that forcing the family to accept brain death would detract from numerous constitutional rights (38).
From a general medical perspective, several questions arise from this ongoing tragic narrative. Is it conceivable that a brain death examination, performed by hospital personnel and a court-appointed expert, could indicate brain death in a patient who—as the family claims—subsequently manifests a degree of brain function? Can a clinical brain death study ever be falsely positive or the findings of brain death be reversed? Can a brain-dead body continue to maintain vital functions, albeit with ventilator support, for several years? From a nuclear medicine perspective, can a scintigraphic examination improve the specificity of determining brain death and thereby reduce the possibility of error? Finally, is there any evidence to suggest that blood flow studies might have a role in illustrating absence of perfusion to an otherwise skeptical family?
This article begins by recapitulating the historical development of brain death (15), reviewing updated practice guidelines, and emphasizing the present role that scintigraphic examinations have in this diagnosis. The limitations of clinical and radionuclide studies will then be presented, followed by speculation on whether radionuclide examinations could play an expanded role.
HISTORICAL DEVELOPMENT OF THE BRAIN DEATH STANDARD
The operative definition of death in any society is based on biologic determinations that are refracted through particular legal, moral, and religious perspectives (8). The predominant definition of death embraced by western societies is absence of circulation and breathing, a cardiopulmonary standard. Before advances in artificial respiration, patients who sustained catastrophic neurologic injury would rapidly progress to cardiopulmonary death. With advances in resuscitation, many such patients could maintain an autonomous heartbeat and never achieve the cardiopulmonary standard, leading to a state of prolonged and irreversible coma even when the brain is devoid of all cerebral and cerebellar function (39). An increased use of resources and the need for organs to transplant have challenged society to revise the definition of death and propelled debate on this topic to the national agenda (40,41).
In 1968, the Ad Hoc Committee of the Harvard Medical School to Examine the Definition of Brain Death introduced a new paradigm of death based on “irreversible coma” with “no discernible central nervous system activity” (1). This concept was codified into U.S. law in the early 1980s by the President’s Commission for the Study of Ethical Problems in Medicine (42), which proposed a Uniform Determination of Death Act (2) that was ultimately written into state laws, albeit with local variations (6). The Act succinctly states that “An individual who has sustained either (1) irreversible cessation of circulatory and respiratory functions, or (2) irreversible cessation of all functions of the entire brain, including the brain stem, is dead. A determination of death must be made in accordance with accepted medical standards.” Factors such as the credentials of the examining practitioners, and the waiting period between repeat examinations, as required, are determined at the discretion of each state. Most notably, the states of New Jersey (43) and New York (44) are unique in allowing for a religious or moral exception to brain death. On the basis of varying legal statutes and regional preferences, the concept of brain death is applied differently in different locales.
Irreversible cessation of all functions in the entire brain, including the brain stem, has been termed the whole-brain standard. Similar or variant formulations of brain death have been adopted throughout the world (5,6); a brain-stem-death standard used in the United Kingdom is defined as irreversible dysfunction of the brain stem alone (4).
Successive clinical guidelines for the determination of brain death were promulgated by the American Academy of Neurology (AAN) (17,45) and the American Academy of Pediatrics (18,46), thereby elaborating on the “accepted medical standards” referred to in the Act (Table 1). Technical guidelines for the performance of scintigraphic studies (20,21,47,48) are summarized in Table 2.
Accepted Medical Standards for Brain Death
Recommended Imaging Techniques for Radionuclide Studies to Support Brain Death
THE EVALUATION OF BRAIN DEATH
The Clinical Examination
Brain death is usually diagnosed by physical examination alone (17). Cardinal elements include coma, absence of brain stem reflexes, and profound apnea (itself a marker for severe disruption of the brain stem), assessed in such a way as to rigorously elicit persistence of a central respiratory drive while avoiding potential hypoxic injury (49,50). The presence of apparently coordinated patient movements is compatible with brain death when mediated through the spinal cord (17,51). The examining physician must be experienced in order to accurately differentiate spine-mediated reflexes from centrally coordinated motion.
Prerequisites to diagnosing brain death by physical examination include a sufficient mechanism of injury, lack of confounding factors (such as drug intoxication or poisoning), and exclusion of complicating medical conditions that interfere with clinical assessment (including facial trauma, pupillary abnormalities, hypothermia, or severe electrolyte, acid–base, or endocrine disturbances). It has been recommended that after the onset of acute brain injury, the physical examination be deferred for several hours in adults (17) or 1–2 d in children (18). In the past, it was recommended that the physical examination be repeated after an appropriate interval, to ensure irreversible cessation of neurologic functions; however, the most recent evidence-based update accepted a single neurologic examination (unless otherwise mandated by local legal statute) in adults (17). In children, the American Academy of Pediatrics currently requires two examinations separated by an age-determined interval (18).
The 2010 AAN evidence-based update (17) failed to find reports of recovery of brain function after brain death by strict application of the 1995 AAN practice parameters. Nevertheless, reports in the medical literature do document neurologic function in patients in whom brain death was previously diagnosed, apparently not according to rigorous criteria (52–54)). In fact, several potential pitfalls have been noted in the clinical determination of brain death (28,55–57). A recent global survey on the determination of brain death demonstrated substantial differences in perceptions and practice worldwide (7). Among the respondents, 53% reported that the formalized brain death protocol in their institution deviated from the AAN criteria. A recent examination of 508 major U.S. hospitals demonstrated wide variability in brain death policies, which were not fully congruent with contemporary practice parameters (26). A chart review of 226 brain-dead organ donors at 68 heterogeneous hospitals in the Midwest United States revealed that documentation was often incomplete, likely reflecting actual variability in practice (58). Adherence to contemporary AAN guidelines was followed strictly in only 45% of patient records and loosely in 37%. Prior studies noted poor documentation of compliance in brain death declarations for adults in British (59) and American (60) hospitals, and similar findings were observed in brain death declarations for children (61,62). Finally, studies have also shown a poor understanding of relevant concepts among many physicians involved in the declaration of brain death (22,23).
Confirmatory and Ancillary Examinations
Role
Confirmatory or ancillary examinations are second-line investigations required only in special situations, primarily to complement the physical examination when components cannot be reliably evaluated (45). These situations include those in which the proximate cause of injury is unknown, a complete examination cannot be performed because of facial trauma or pupillary abnormalities, or the apnea test cannot be completed because of difficulty in maintaining adequate oxygenation. Radionuclide studies can also be used to document absence of blood flow in patients in whom elevated levels of sedatives or neuromuscular blockers are present (18,63). In some jurisdictions, a confirmatory examination can eliminate the requirement for a second examiner or a second examination after a prescribed waiting interval.
Choice of Examination
Confirmatory examinations include those that demonstrate absence of electrical activity (electroencephalography and somatosensory evoked potentials) and those that evaluate blood flow (radionuclide studies, multivessel angiography, and CT or MR angiography). The AAN accepts 3 methods of evaluating blood flow: conventional contrast-enhanced angiography, transcranial Doppler ultrasonography, and 99mTc-exametazime (99mTc-HMPAO) scintigraphy (45), while there is insufficient evidence to determine whether examination methods newer than these can also accurately identify brain death (17). The American Academy of Pediatrics lists 4-vessel angiography and radionuclide cerebral blood flow studies as acceptable methods (18). Specific states may permit additional methods of examination in accordance with accepted medical standards and local regulations (64,65).
Issues of relevance in choosing a confirmatory examination include its availability after hours, its accuracy across multiple operators and interpreters, its ability to be performed at the bedside, and whether it has any potentially deleterious side effects to the patient or organs (especially when the organs are slated for transplantation). An optimal examination should be unaffected by drug effects or metabolic disturbances, relatively standardized, and sufficiently robust to be the sole means of establishing brain death (66). Radionuclide examinations achieve many of these criteria. After-hours staffing and portable cameras may not be supported in typical departments, and a restricted off-hours availability of radiopharmaceuticals, compounded by their short shelf-life, may also limit implementation.
Nonlipophilic Radiopharmaceuticals
The initial scintigraphic blood flow studies used nonlipophilic radiopharmaceuticals, such as 99mTc-diethylenetriaminepentaacetic acid (DTPA) (Fig. 1), 99mTc-glucoheptonate, and 99mTc-TcO4− (Fig. 2), which do not cross the intact blood–brain barrier (67,68). Renal radiopharmaceuticals are favored because of relatively rapid blood clearance, which facilitates repetition of the studies as needed, and a lack of appreciable uptake overlying structures important to diagnosis. On scrutiny of the angiographic phase immediately after injection, visualization of activity within the anterior or middle cerebral arteries indicates cerebral blood flow (Fig. 1), whereas nonvisualization, after an adequate injection, indicates absence of flow (Fig. 2). The venous sinuses may be visualized via scalp vein collaterals even in the setting of brain death (69–71).
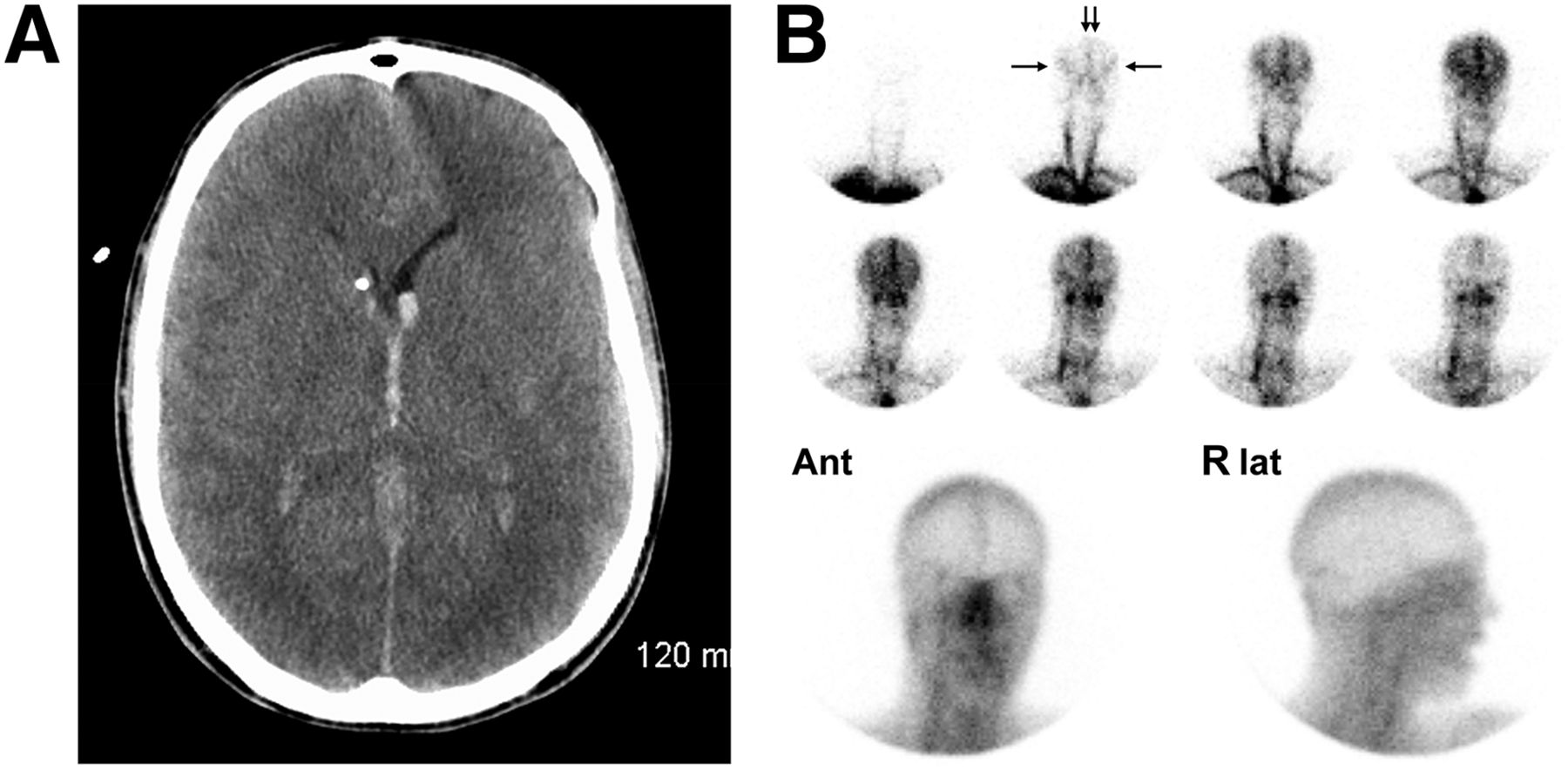
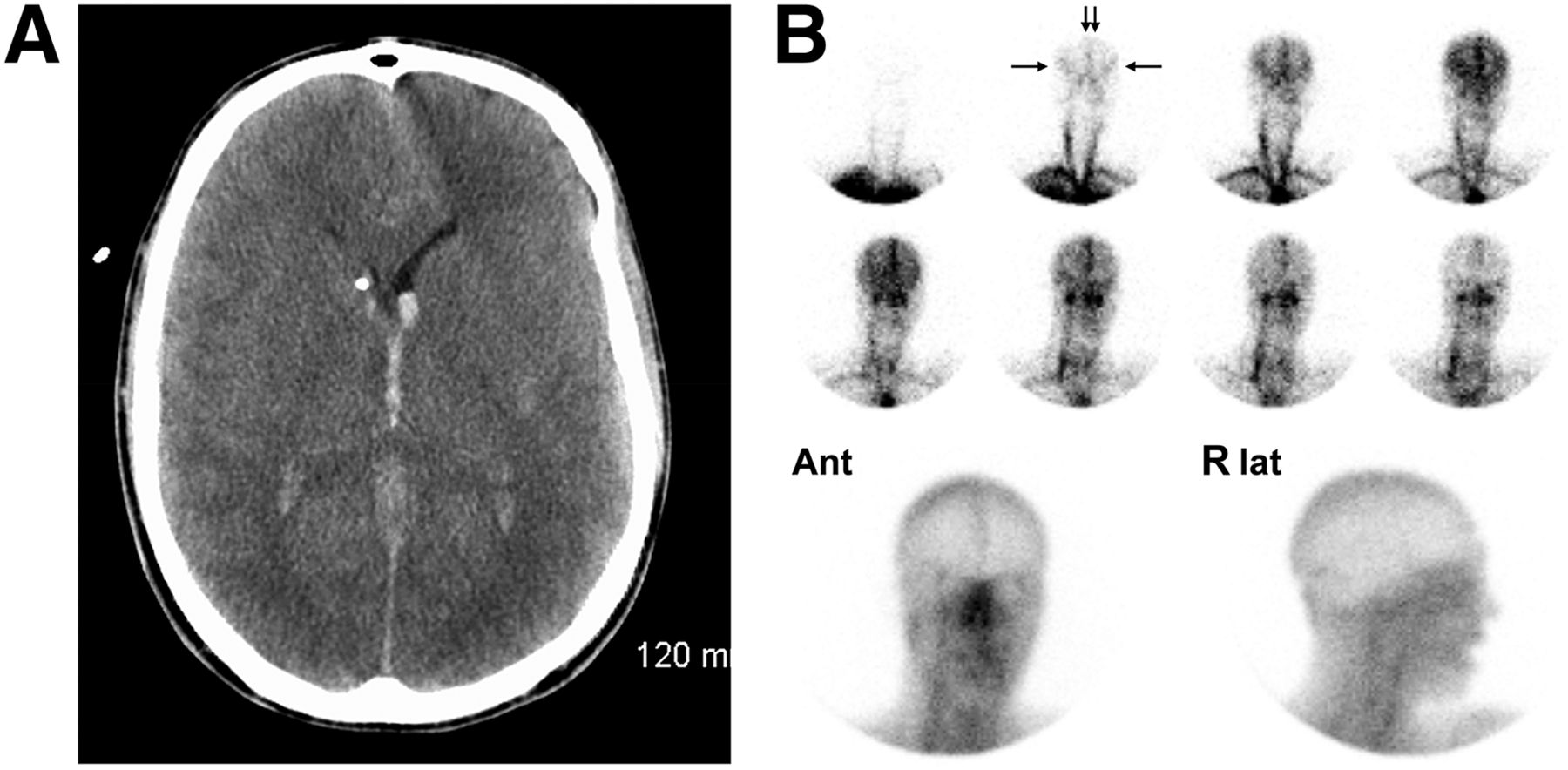
Findings of persistence of blood flow on blood flow study using nonlipophilic radiopharmaceutical in 22-y-old man with ruptured aneurysm of left posterior inferior cerebral artery. (A) CT scan demonstrates intraventricular and subarachnoid hemorrhage. (B) Two-second flow images (top rows) after injection of 905 MBq of 99mTc-DTPA demonstrate excellent visualization of anterior (vertical arrows) and middle (horizontal arrows) cerebral arteries, forming a trident appearance, indicating presence of perfusion, which progresses into visualization of intracranial venous sinuses. On immediate anterior (Ant) and right lateral (R lat) static images (bottom row), radiopharmaceutical does not cross blood–brain barrier; however, activity is noted in venous sinuses.

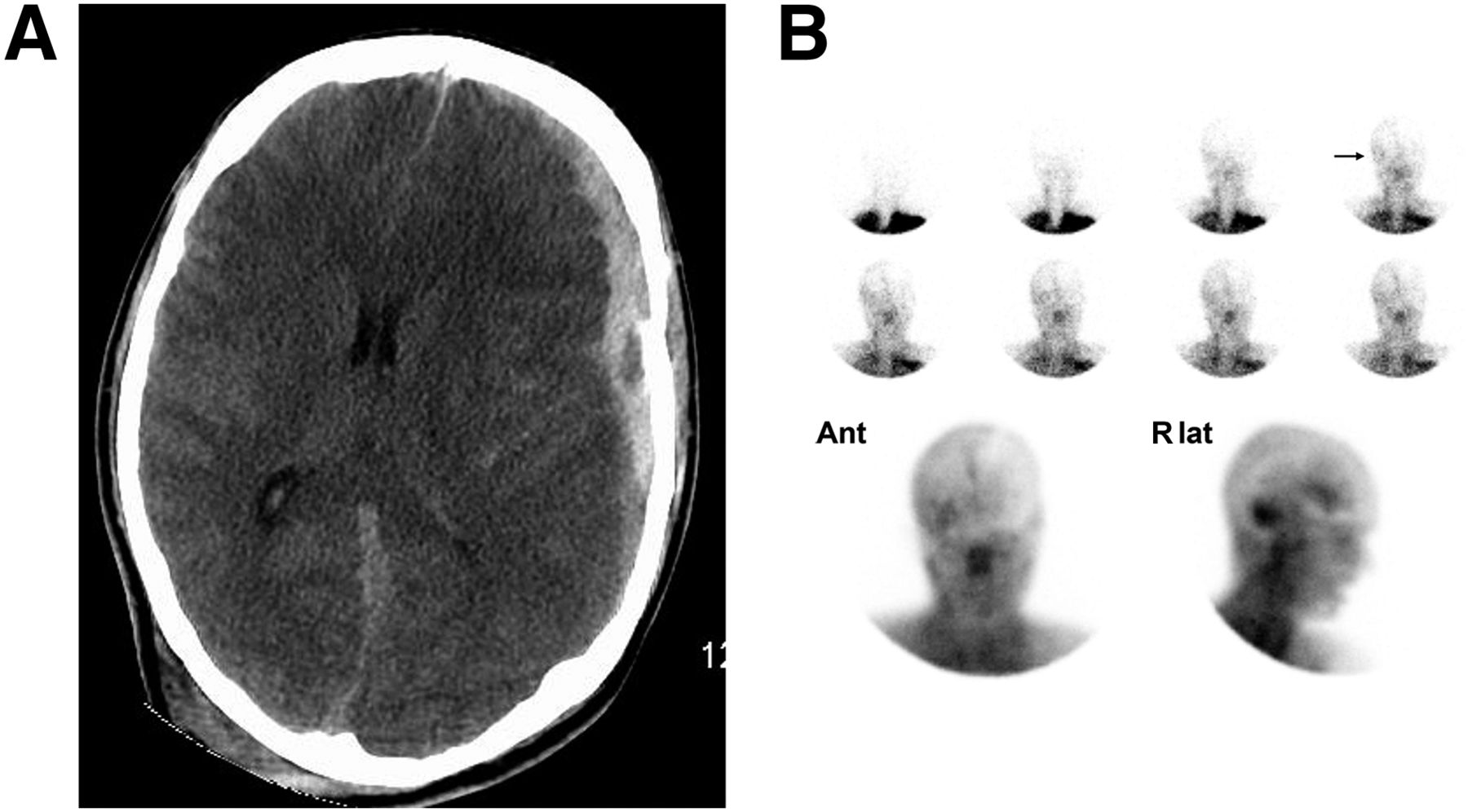
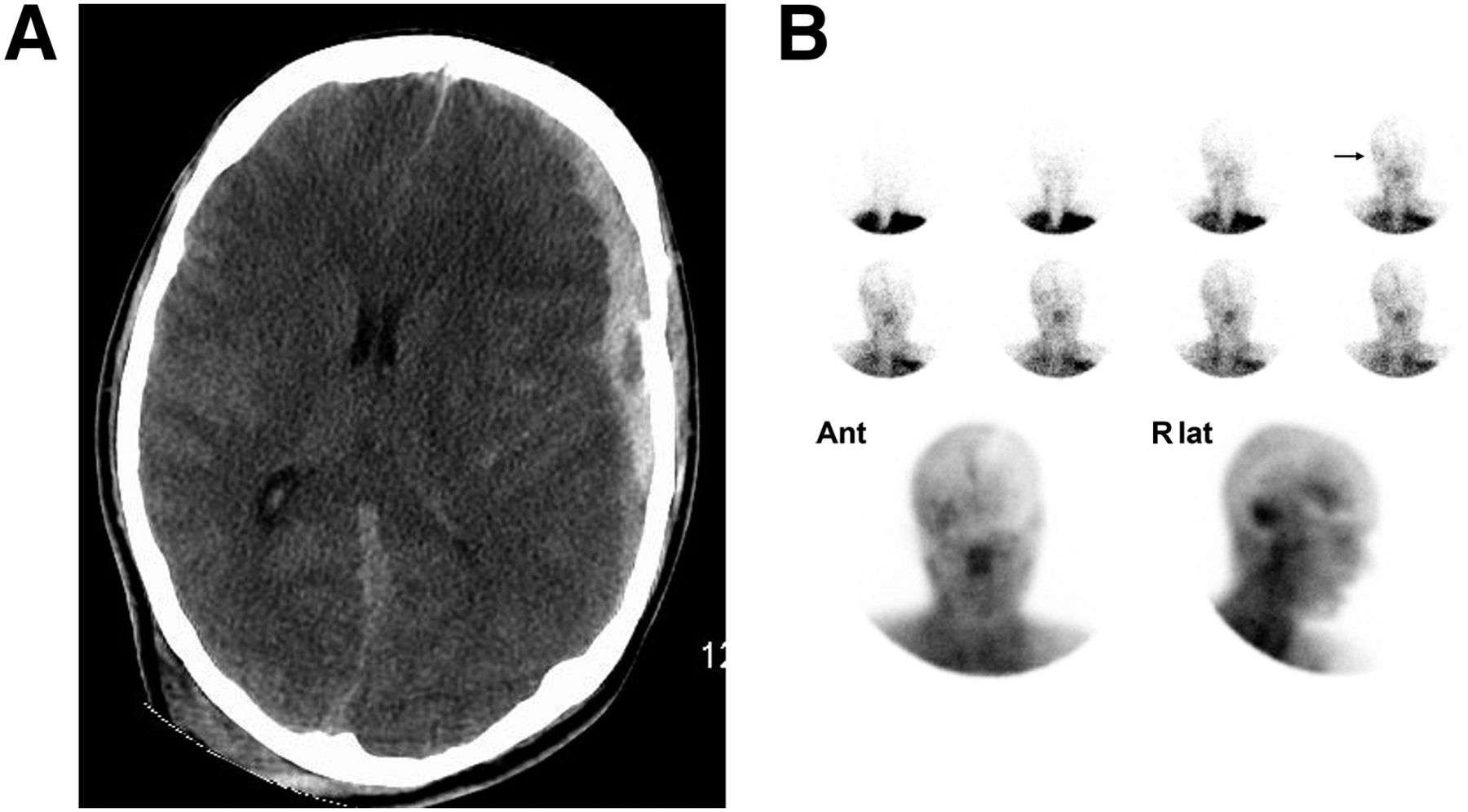
Findings of absence of blood flow on blood flow study using nonlipophilic radiopharmaceutical 99mTcO4− in 28-y-old woman with diffuse cerebral edema due to hypoxic ischemic injury after hanging. (A) CT scan demonstrates diffuse loss of white matter–to–gray matter differentiation in cerebral hemispheres. (B) Two-second flow images (top rows) demonstrate visualization of common carotid arteries in neck (arrows) but no flow into skull. On immediate anterior (Ant) and left lateral (L lat) static images (bottom row), no activity is seen within venous sinuses. 99mTcO4− has localized in salivary glands and thyroid.
Lipophilic Radiopharmaceuticals
Since their introduction in the mid-1980s (72–74), the lipophilic radiopharmaceuticals 99mTc-HMPAO (75–79) and 99mTc-bicisate (Neurolite; Lantheus Medical Imaging) (47,48,80), which cross the blood–brain barrier and become trapped in the brain parenchyma, have been used in the determination of brain death. Parenchymal trapping appears preserved even in the presence of metabolic derangements (78,79). There is a good correlation with 4-vessel contrast angiography (81). Both an early angiographic phase and a subsequent parenchymal phase are imaged; the presence of blood flow on either is incompatible with brain death (Figs. 3 and 4). The initial 99mTc-HMPAO preparations degraded rapidly and needed to be injected within 30 min of reconstitution (82). The subsequently developed stabilized formulations have a longer shelf-life but require injection through a 0.45-μM filter to exclude particulate matter (83); care must be taken to ensure that this filtration does not hinder delivery of an adequate bolus.

Findings of persistence of blood flow on blood flow study using lipophilic radiopharmaceutical in 18-y-old man after motor vehicle accident followed by left-sided craniotomy to evacuate subdural hematoma. (A) CT indicates loss of white matter–to–gray matter differentiation in left posterior cerebral artery territory and right posterior parasagittal cortex territory. There is diffuse cerebral edema and transtentorial herniation with compression of basilar cisterns. (B) Two-second flow images (top rows) demonstrate excellent visualization of anterior (vertical arrows) and middle (horizontal arrows) cerebral arteries, resembling a trident, with retention of activity within brain parenchyma, thereby indicating presence of blood flow. Anterior (Ant) and left lateral (L lat) parenchymal phase images (bottom row) demonstrate somewhat inhomogeneous though extensive brain perfusion.

Findings of absence of blood flow on blood flow study using lipophilic radiopharmaceutical in 33-y-old man after hanging. (A) CT scan demonstrates diffuse cerebral edema with narrowing of lateral ventricles and bilateral infarction of lentiform nuclei. (B) Two-second flow images (top rows) after injection of 799 MBq of 99mTc-HMPAO demonstrate excellent visualization of common carotid arteries (arrows) but absence of flow into calvarium, consistent with brain death. Anterior (Ant) and left lateral (L lat) parenchymal phase images (bottom row) demonstrate complete lack of perfusion within boney skull (light-bulb or hollow-skull sign), including absence of posterior fossa and superior sagittal sinus. More technically demanding SPECT imaging is generally not performed in these critically ill patients.
The static parenchymal phase is the more sensitive, and therefore crucial, component because of its ability to adequately evaluate the posterior fossa (Fig. 5); dynamic blood flow studies, typically performed in an anterior projection, are unable to do so (79,84). In clinical studies, perfusion has been observed more often on delayed imaging than on the dynamic angiographic phase (77,78,85,86). de la Riva has illustrated cases in which flow was absent on the angiographic phase but cerebellar perfusion was clearly present on static parenchymal images (79). In addition, sensitivity is greater on the parenchymal phase, as higher-count static images offer statistical discrimination superior to that of short-duration dynamic images. Static imaging is also less dependent on bolus technique and timing of injection; imaging can be repeated, including tomographic imaging if clinically feasible (87–89). Dynamic flow images retain residual value in excluding the uncommon possibility that absence of visualization on parenchymal images is due to a failed 99mTc-HMPAO preparation (20,78,90).
Findings of blood flow confined primarily to posterior fossa on blood flow study using lipophilic radiopharmaceutical in 24-y-old man who fell down flight of stairs and suffered multiple fractures of skull base. (A) CT scan demonstrates presence of bilateral subarachnoid and moderate left subdural hemorrhages, along with mass effect, including transtentorial herniation and compression of left lateral ventricle. (B) Two-second flow images (top rows) after injection of 99mTc-HMPAO demonstrate vague visualization of arterial flow to right lower calvarium (arrow) with appearance of superior sagittal sinus. Anterior (Ant) and right lateral (R lat) static images (bottom row) demonstrate relatively intense perfusion of right cerebellum with suggestion of probable visualization of periventricular activity.
The brain stem is not reliably visualized on planar imaging, though it may be so on tomographic imaging. SPECT has occasionally been used to assess brain death (87–89), but technical demands represent a challenge in a respirator-dependent patient.
Choice of Nonlipophilic Versus Lipophilic Radiopharmaceuticals
Many believe that studies using lipophilic radiopharmaceuticals (incorporating both parenchymal and angiographic phases) are superior to studies using nonlipophilic radiopharmaceuticals (which include only an angiographic phase). On direct comparison of 99mTc-DTPA and 99mTc-HMPAO imaging, there was complete agreement between the two methods in 14 patients with brain death and 12 patients with persistent flow (91). 99mTc-HMPAO was considered more technically forgiving, though expensive. The Society of Nuclear Medicine and Molecular Imaging (SNMMI) Procedure Guideline for Brain Death Scintigraphy (20,48) lists the relative accuracies of lipophilic and nonlipophilic agents as being among the issues that require further clarification. The revised guidelines (20) note that although the lipophilic radiopharmaceuticals are “increasing in popularity” “there is no clear evidence that they are more accurate than nonspecific agents.” They are preferred by some institutions because they are less dependent on a bolus, and delayed images are usually definitive for the presence of blood flow. Furthermore, the lipophilic agents evaluate regional brain tissue perfusion and hence brain viability, whereas nonlipophilic radiopharmaceuticals provide information only on low-resolution vascular flow (20). AAN (45) and Canadian guidelines (64) reference only lipophilic radiopharmaceuticals; the Belgian Society for Nuclear Medicine (92) lists 99mTc-HMPAO and 99mTc-ethyl cysteinate dimer (ECD), favoring the first because it is more validated; and the current joint ACR–SPR Practice Parameter (21) lists 99mTc-ECD and 99mTc-HMPAO equally and includes nonlipophilic radiopharmaceuticals such as 99mTc-DTPA as an alternative option. Consensus appears to favor lipophilic radiopharmaceuticals whenever available.
Limitations of Clinical and Imaging Examinations
At one time it was thought that clinical brain death correlated with a pathologic entity of total brain necrosis (“respirator brain”), but this correlation has not been substantiated in more recent pathologic examinations (93). It was also believed that patients could not be maintained for prolonged periods after clinical brain death (42,94). Long-term survival is actually possible, especially in patients who are younger or have primarily neurologic and not multisystem etiologies of brain death (95).
Two definitions of brain death have been established in the AAN guidelines (17): a purely clinical diagnosis, and a diagnosis that uses confirmatory examinations to complement deficiencies in the physical examination. These definitions are not congruent, with internal inconsistencies that can ultimately lead to contradictory conclusions (15). Reports in the literature persist of patients in whom the physical examination unequivocally demonstrated brain death, yet specific confirmatory tests indicated the presence of blood flow, electrical activity, or other phenomena (15,53,81,96). Although erroneous performance of either the physical examination or the confirmatory test is a possible cause of conflicting findings, Wijdicks believes that the clinical entity of brain death can coexist with preserved blood flow on ancillary examinations and should not deter a physician from declaring patients dead after complete and properly conducted physical examinations and apnea testing (57,97). How to adjudicate situations in which the neurologic and ancillary examinations are discordant is currently unresolved, and a conservative approach should be in order (15).
Although elevation of intracranial pressure causes global hypoperfusion of the brain (98) and effectively eliminates small areas of perfused tissue that could prevent a confirmatory diagnosis of brain death, case reports indicate that in the context of clinical brain death, blood flow may persist under the exceptional circumstance that the skull is no longer a closed space (as in patients with open fontanelles, cerebrospinal fluid shunts, ventricular drains, or skull defects (89,99)) or if insufficient time has elapsed after the brain injury (100–102). In the latter situation, studies repeated after an adequate interval (e.g., 12 h) generally show reversion to complete absence of blood flow. To avoid discrepant cases, it has been suggested that blood flow studies be delayed for at least 6 h after the clinical finding of brain death (17,18,101).
The hot-nose sign—a prominent central region seen overlying the face on flow and blood pool studies—has frequently been described in the context of brain death (103). A report has suggested that the hyperemic region is actually more posterior, in the region of the brain stem and cervical spinal cord (104), though this hypothesis is hard to reconcile with profound brain stem dysfunction. The hot-nose sign is neither specific nor sensitive for brain death and therefore is unreliable (105).
Potential Expanded Role for Radionuclide Blood Flow Studies
In light of the variation in hospital brain death protocols and their application, as well as the apparent difficulties in performing the clinical examination and the periodic reluctance of families to embrace the brain-death standard, could there be an increased role for radionuclide perfusion examinations in helping to support the diagnosis of brain death (89,106)? Radiographic testing before retrieval of organs from donors who meet clinical brain death criteria might provide conclusive evidence of permanent and irreversible loss of brain function (107), and more-routine use of ancillary brain blood flow analyses might reduce errors (53). A diametrically opposed viewpoint is espoused by Wijdicks, who has suggested that a comprehensive clinical examination, when performed by skilled examiners, should trump any conflicting ancillary examinations (57,97).
Ancillary studies may also be helpful for social reasons, allowing family members to better comprehend the diagnosis of brain death (18). Presentation of visual, objective support for the diagnosis of brain death provides family members with a psychologic benefit that helps them with the decision to withdraw care (108). Offering families the opportunity to review images from a radionuclide blood flow study may be an effective method of demonstrating brain death (109). Although several authors have begun to measure the efficacy of radionuclide studies in determining brain death, more work is needed to evaluate the effect of brain death on elapsed time until certification of death and the rate of organ donation (63,108,110).
THE MCMATH CASE IN RETROSPECT
In closing, we return to the tragic McMath case. It seems reasonable to accept that there have been no cases of a false-positive determination of brain death when the neurologic examination and apnea test have been properly performed; however, errors in the performance of brain death protocols are described in actual practice. In the McMath case, it is likely that the neurologic examination was carefully performed and rechecked by the outside court-appointed expert. Confirmatory examinations, such as radionuclide perfusion studies, have been suggested as a means of detecting and eliminating these errors (though it is not known whether ancillary examinations were performed in the McMath case). Patient movement due to spinally mediated reflexes may occur, mimicking centrally directed motion. Brain-dead patients, especially when young and adequately cared for, can maintain homeostasis for years. There may be a role for blood flow studies in illustrating absence of perfusion to otherwise skeptical families, a concept that has not been rigorously examined.
Acknowledgments
The author would like to acknowledge contributions by Drs. Sadri Bazarjani, Joseph Sommerfeldt, and Matthieu Pelletier-Galarneau in critically reviewing the manuscript and Alexandra Davis, BA, MLIS, in providing research assistance.
Footnotes
Published online Aug. 11, 2016.
Learning Objectives: On successful completion of this activity, participants should be able to (1) relate the diagnostic protocols and recommendations regarding the clinical diagnosis of brain death; (2) list the relative advantages and disadvantages of lipophilic and nonlipophilic blood flow radiopharmaceuticals for brain blood flow studies; and (3) consider how the nuclear medicine blood flow study could assist the clinician in making the difficult diagnosis of brain death.
Financial Disclosure: The author of this article has indicated no relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through October 2019.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- 1.↵
- 2.↵
- 3.
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.
- 10.
- 11.
- 12.↵
- 13.↵
- 14.
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.
- 71.↵
- 72.↵
- 73.
- 74.↵
- 75.↵
- 76.
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- Received for publication May 23, 2016.
- Accepted for publication August 8, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}