


Abstract
Earlier clinical studies reported a high sensitivity of pretargeted immunoscintigraphy using murine or chimeric anticarcinoembryonic antigen (CEA) bispecific antibody (BsMAb) and peptides labeled with 111In or 131I in medullary thyroid carcinoma (MTC). Preclinical studies showed that new-generation humanized recombinant anti-CEA × antihistamine-succinyl-glycine (HSG) trivalent BsMAb TF2 and radiolabeled HSG peptide (IMP288) present good features for PET. This study aimed at optimizing molar doses and pretargeting interval of TF2 and 68Ga-labeled IMP288 for immuno-PET in relapsed MTC patients with calcitonin serum levels greater than 150 pg/mL. Methods: Five cohorts (C1–C5) of 3 patients received variable molar doses of TF2 and approximately 150 MBq of 68Ga-IMP288 after different pretargeting time intervals (C1: 120 nmol TF2, 6 nmol IMP288, 24 h; C2: 120 nmol TF2, 6 nmol IMP288, 30 h; C3: 120 nmol TF2, 6 nmol IMP288, 42 h; C4: 120 nmol TF2, 3 nmol IMP288, 30 h; and C5: 60 nmol TF2, 3 nmol IMP288, 30 h). TF2 and 68Ga-IMP288 pharmacokinetics were monitored. Whole-body PET was recorded 60 and 120 min after 68Ga-IMP288 injection. Tumor maximal SUV (T-SUVmax) and T-SUVmax–to–mediastinum blood-pool (MBP) SUVmean ratios (T/MBP) were determined. Results: In C1, T-SUVmax and T/MBP ranged from 4.09 to 8.93 and 1.39 to 3.72 at 60 min and 5.14 to 11.25 and 2.73 to 5.38 at 120 min, respectively. Because of the high MBP, the delay was increased to 30 h in C2, increasing T-SUVmax and T/MBP. Further increasing the delay to 42 h in C3 decreased T-SUVmax and T/MBP, showing that 30 h was the most favorable delay. In C4, the TF2-to-peptide mole ratio was increased to 40 (delay 30 h), resulting in high T-SUVmax but with higher MBP than in C2. In C5, the molar dose of TF2 was reduced, resulting in lower imaging performance. Pharmacokinetics demonstrated a fast TF2 clearance and a clear relationship between blood activity clearance and the ratio between the molar amount of injected peptide to the molar amount of circulating TF2 at the time of peptide injection. Conclusion: High tumor uptake and contrast can be obtained with pretargeted anti-CEA immuno-PET in relapsed MTC patients, especially using optimized pretargeting parameters: a BsMAb-to-peptide mole ratio of 20 and 30 h pretargeting delay.
Medullary thyroid carcinoma (MTC) is relatively infrequent, accounting for less than 10% of all thyroid cancers (1). After initial surgery, serum calcitonin is still detectable in nearly 20% of patients, suggesting residual disease, and imaging including neck ultrasonography, neck and chest CT, liver contrast-enhanced CT or MRI, and spine and pelvic bone MRI is recommended when serum calcitonin is higher than 150 pg/mL (1,2). With the ability to characterize and quantify cancer molecular processes, 18F-DOPA or 18F-FDG PET/CT also show high performance in relapsed MTC patients and great potential as surrogate biomarkers, useful for early response evaluation and prediction of clinical outcome (3–6).
MTC is characterized by an intense expression of CEA, and previous clinical trials showed the high sensitivity of pretargeted immunoscintigraphy using murine or chimeric anti-CEA bispecific antibody (BsMAb) and pretargeted haptens-peptides labeled with 111In or 131I (5,7,8). These results and the high potential of immuno-PET reported in other solid tumors using different radioimmunoconjugates suggested that pretargeted haptens labeled with PET emitters would allow high-sensitivity and -specificity imaging under good conditions of radiation protection and dosimetry (9,10).
Today, new pretargeting reagents have been designed (11–15). TF2 is an engineered trivalent BsMAb composed of a humanized anti–histamine-succinyl-glycine Fab fragment derived from the murine 679 antibody and 2 humanized anti-CEA Fab fragments derived from the hMN-14 antibody, formed into a 157-kD protein by the dock-and-lock procedure (11). IMP288 is a bivalent histamine-succinyl-glycine hapten that can be labeled with a variety of radionuclides for therapy (90Y and 177Lu), scintigraphy (111In), or PET (124I, 68Ga, and 18F). The clinical implementation of pretargeting requires a first phase to optimize the BsMAb and peptide molar doses and the delay between the 2 injections (14–17). The first clinical results were reported using TF2/177Lu-IMP288 in colorectal carcinoma patients, showing fast tumor uptake and high tumor–to–background activity ratios within a few hours (14). This feature is favorable for labeling with short-lived 68Ga and 18F, as confirmed by animal studies, 68Ga having the advantage of availability via a generator (13).
Thus, a study was designed in relapsed MTC patients to transfer into the clinic TF2/68Ga-IMP288 pretargeting, with a first part to determine the best pretargeting parameters in different cohorts of patients injected with variable TF2 and IMP288 molar doses at variable pretargeting delays and a second part to assess immuno-PET performances. We report here the results of the optimization part of the study.
MATERIALS AND METHODS
Population
Patients 18 y or older with a histologic diagnosis of MTC treated by complete surgery and presenting a calcitonin serum level of 150 pg/mL or more with at least 1 lesion 10 mm or greater on conventional imaging were eligible. In the 4 wk preceding immuno-PET, a staging workup that included a complete history, physical examination, CEA, and calcitonin serum level measurements (with biomarker doubling time determination when possible) was performed. As recommended by the international guidelines, contrast-enhanced CT of the neck, chest, abdomen, and pelvis; bone marrow MRI; and liver MRI were performed (2). 18F-DOPA PET/CT was also performed to obtain an optimal disease staging. The other inclusion criteria were a Karnofsky performance status of 70 or greater or Eastern Cooperative Oncology Group performance status 0–1, minimum life expectancy of 6 mo, creatinine 2.5 or less × normal, and normal serum human antimouse antibody and human antihumanized antibody titers. Women of child-bearing potential were required to have a negative pregnancy test. The exclusion criteria were pregnancy and breast feeding; anticancer treatment within 6 wk before immuno-PET or necessity to start anticancer treatment in the 3 mo after immuno-PET; any serious active disease or comorbid medical condition (according to the investigator’s decision); any history of other cancer during the last 5 y, with the exception of nonmelanoma skin tumors or stage 0 (in situ) cervical carcinoma; and a known hypersensitivity to antibodies or proteins. The trial, sponsored by Nantes University Hospital, was approved by the responsible ethics committee (CPP), registered at ClinicalTrial.gov (NCT01730638), and all patients signed a written informed consent form.
Investigational Products and Labeling
The reagents were prepared suitable for human use by Immunomedics, Inc. A 1.85-GBq (at calibration time) pharmaceutical-grade 68Ga generator (Eckert-Ziegler) was used. 68Ga-IMP288 was obtained with a specific activity of 40–100 MBq/nmol and a radiochemical purity greater than 95%.
TF2 diluted in 250 mL of 0.9% NaCl and 68Ga-IMP288 in 50 mL of 0.9% NaCl were administered by intravenous infusion over 30 min. Patients were premedicated with antihistamine (orally) the day before TF2 infusion and with antihistamine (polaramine) and corticosteroid (hydrocortisone hemisuccinate) (intravenously) 5 min before TF2 infusion. For patients 11 to 16, the same premedication was also administered before peptide infusion.
Study Design
Five pretargeting conditions were examined in 5 cohorts (C1–C5) of 3 patients (Table 1). Safety was assessed by monitoring vital signs, performing physical examination, and monitoring adverse events. For the 3-mo follow-up, the imaging methods (CT, MRI, 18F-DOPA, or 18F-FDG PET/CT) chosen to confirm abnormalities revealed by immuno-PET but not detected by baseline imaging were decided by a panel of experts comprising endocrinologists, radiologists, and nuclear physicians. A lesion detected by immuno-PET was considered related to MTC when confirmed by histology or detected by one other imaging modality and confirmed by the follow-up. Human antihumanized antibody was determined 3 or 6 mo after TF2 infusion using an enzyme-linked immunosorbent assay (ELISA) method (abnormal when ≥ 50 ng/mL).
Scheme of Study Cohorts
PET/CT Imaging
PET/CT was performed using a 4-ring Siemens Biograph mCT system with time-of-flight capability 60 and 120 min after 68Ga-IMP288 injection and reconstructed using a 3-dimensional ordinary Poisson ordered-subset expectation maximization with point-spread function correction and time-of-flight mode (3 iterations, 21 subsets, 2 mm in full width at half maximum gaussian postfiltering, and voxel size of 4 × 4 × 2 mm). Whole-body images were acquired under normal tidal respiration for 2.5 min per bed position. CT was performed using variable mAs, 120 kVp, and a pitch of 1 without contrast enhancement. Images were acquired from the top of the head to mid-thigh (6–8 steps per patient). Tumor SUVmax (T-SUVmax) was determined on the most intense focus in the whole-body scan, confirmed as MTC according to the gold standard. Mediastinum blood-pool SUVmean (MBP-SUVmean) was measured within a small volume of interest manually placed in the right atrium (V = 1–2 cm3). The ratio of T-SUVmax to MBP-SUVmean (T/MBP) was subsequently calculated.
Pharmacokinetics Analysis
Blood samples were collected before TF2 infusion, 5 min before the end of TF2 infusion, 5 min and 1 and 2–4 h after infusion, and 5 min before the 68Ga-IMP288 injection. TF2 concentrations were determined by ELISA. Blood samples were also collected 5 min and 1, 2, and 3–4 h after the 68Ga-IMP288 injection and counted immediately after the end of the blood collection, corrected for radioactive decay, and transformed into molar concentrations.
Pharmacokinetics population modeling was performed using 2-compartment models as described previously (17).
RESULTS
The characteristics of the 16 included patients are presented in Table 2. One of these patients did not receive the full hapten dose and was excluded. Fifteen patients (3 per cohort) were thus analyzed. No patient experienced an anaphylactic reaction during or after TF2 infusion. One patient experienced grade 3 reaction starting immediately after hapten infusion with malaise, bronchospasm, tachycardia, and hypertension requiring hospitalization. Human antihumanized antibody analyzed in 11 patients (at 3 and 6 mo in 9 and only at 3 mo in 2) was abnormal in 2 patients, equal to 52 ng/mL at 3 mo and normalized at 6 mo in one and normal at 3 mo and abnormal at 6 mo (244 ng/mL) in the other.
Patient Characteristics (n = 16)
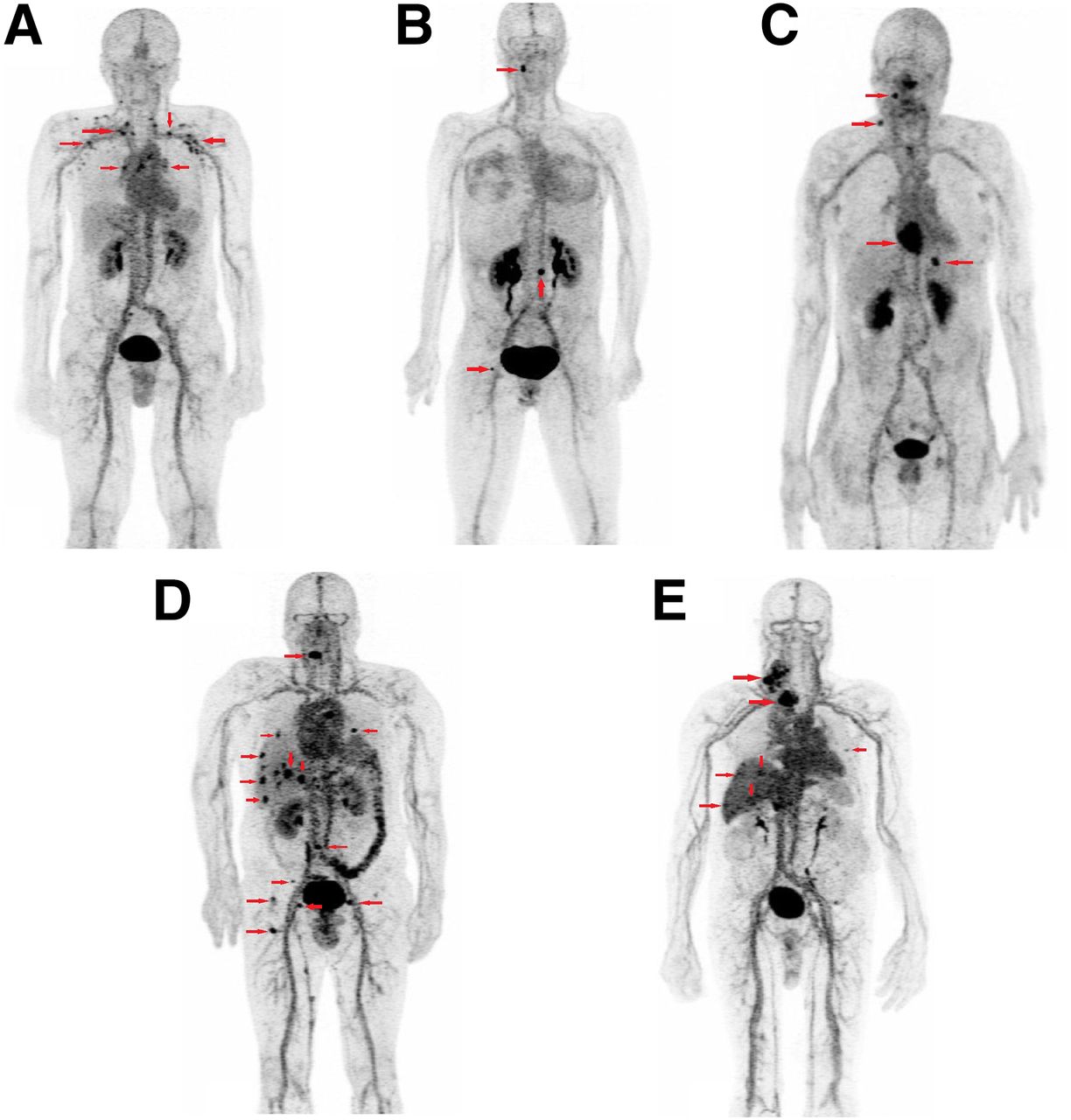
Immuno-PET revealed abnormal foci in all patients, confirmed as MTC in 14 of them (Table 3). In patient 16, immuno-PET detected 1 neck focus not confirmed by conventional imaging or 18F-DOPA PET/CT at the time of the analysis. Figure 1 presents 1 example of immuno-PET in each cohort and Table 4 semiquantitative analysis results. In cohort 1, T-SUVmax ranged from 4.1 to 8.9 at 60 min; tumor uptake and T/MBP increased for the 3 patients between 60 and 120 min. We considered MBP uptake in cohort 1 as too high and lengthened the delay to 30 h in cohort 2, thus increasing T-SUVmax and T/MBP. Only 1 patient showed an increase of tumor uptake and contrast between 60 and 120 min. Because of the improvement between cohort 2 and cohort 1, the delay was further increased to 42 h in cohort 3, decreasing T-SUVmax and contrast. Thus, the 30-h pretargeting delay appeared to be the most favorable. In cohort 4, the pretargeting delay was set back to 30 h, and the TF2/peptide mole ratio was increased to 40 by injection of a lower IMP288 dose (3 nmol). With this schedule, high T-SUVmax was obtained, but with higher MBP-SUVmean than in cohort 2. Tumor uptake and contrast increased in the 3 patients between 60 and 120 min. A reduced TF2 dose was tested in cohort 5, resulting in high tumor uptake in 2 patients but also in relatively high MBP, with increase of tumor uptake and contrast between 60 and 120 min. In contrast, blood activity was low in patient 16.
Number of Confirmed Lesions According to Gold Standard Detected by Immuno-PET, 18F-DOPA PET/CT, and Conventional Imaging for Each Patient
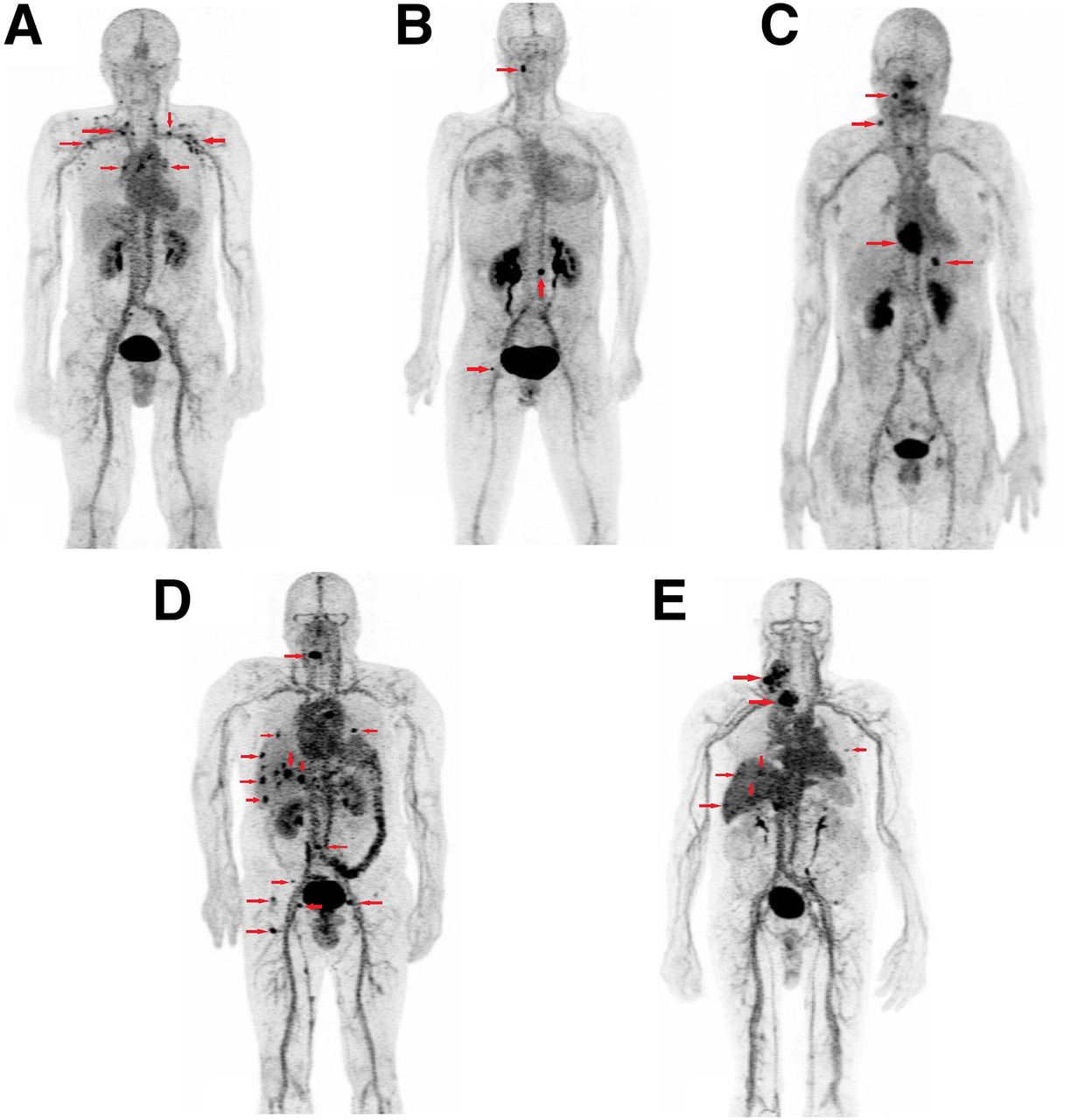
Immuno-PET maximum-intensity-projection images recorded in 1 patient of each cohort. Arrows showed foci considered as pathologic by immuno-PET: supradiaphragmatic nodes in C1 (A) cervical node; lumbar and femoral bones foci in C2 (B); supradiaphragmatic nodes and liver and heart lesions in C3 (C); supradiaphragmatic nodes, lung, liver, and bone foci in C4 (D); and supradiaphragmatic nodes and liver foci in C5 (E).
Semiquantitative Immuno-PET Analysis
TF2 pharmacokinetics were well described by a 2-compartment model according to the population approach (Fig. 2; Supplemental Table 1 [supplemental materials are available at http://jnm.snmjournals.org]), but because of the short sampling time span, limited by the low injected dose and the limited sensitivity of the ELISA assay, the estimation of the T1/2 of the β-phase was not good for 2 patients (3 and 16). TF2 clearance was fast, estimated at 0.6 ± 0.1 L/h, with a T1/2 of the α-phase of 4.1 ± 0.5 h. The T1/2 of the β-phase, after exclusion of the 2 outliers, was 14.3 ± 1.2 h. The interindividual variability was limited and explained in part by body surface differences: the coefficient of variation of the estimations of central compartment volume was reduced from 11.0% to 3.4% if reported by body surface. As a result of the fast clearance, the concentrations of circulating TF2 at the time of hapten injection changed dramatically from 24 to 42 h (Fig. 2).

Pharmacokinetics of bispecific antibody TF2. Patient received infusion of 60 (brown) or 120 nmol (purple) of TF2.
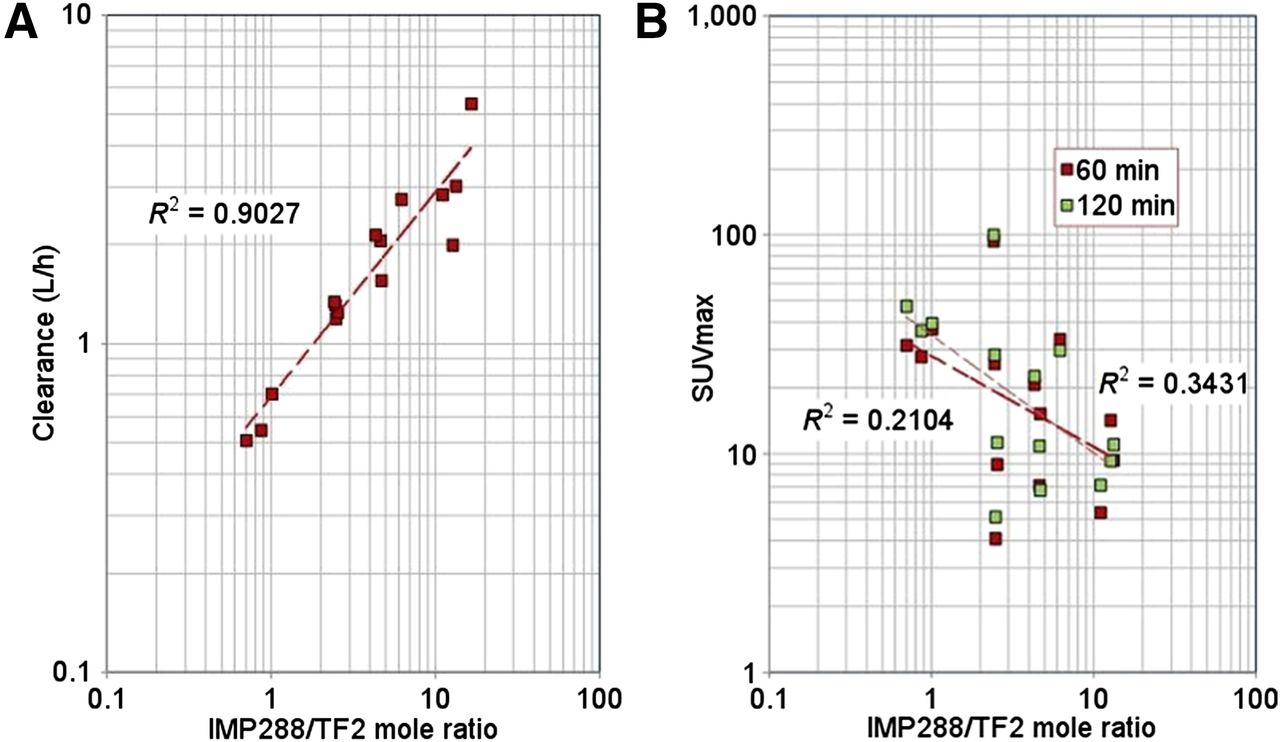
IMP288 pharmacokinetics was also well represented by a 2-compartment model (Fig. 3; Supplemental Table 2). Circulating TF2 is expected to bind the hapten and to reduce its clearance, and the mean cohort clearances seemed to increase with the increase of time delay (C1, 1.2 ± 0.1 L/h; C2, 2.1 ± 0.6 L/h; C3, 2.6 ± 0.5 L/h) for the same molar doses of TF2 (120 nmol) and IMP288 (6 nmol). Similarly, reducing the IMP288 dose to 3 nmol decreased its clearance (C4, 1.0 ± 0.5 L/h). In C5, with a TF2 dose reduced to 60 nmol, patients 14 and 15 showed a relatively slow TF2 clearance (0.46 and 0.36 L/h) and patient 16 a faster clearance (0.7 L/h). As a result, TF2 concentrations were high in patients 14 and 15, explaining the slower IMP288 clearances (0.54 and 0.7 L/h) and the high MBP on immuno-PET, and low for patient 16, explained in part by fast IMP288 clearance (5.4 L/h). Overall, a good correlation (R2 = 0.9) was obtained between IMP288 clearance and the circulating molar amount of TF2 at the time of peptide injection (Fig. 4A). The correlation between this molar ratio and SUVmax was not as good (Fig. 4B).

Pharmacokinetics of 68Ga-IMP288. Results are plotted as semilog plot with population (dashed lines) and individual (solid lines) fitted curves.
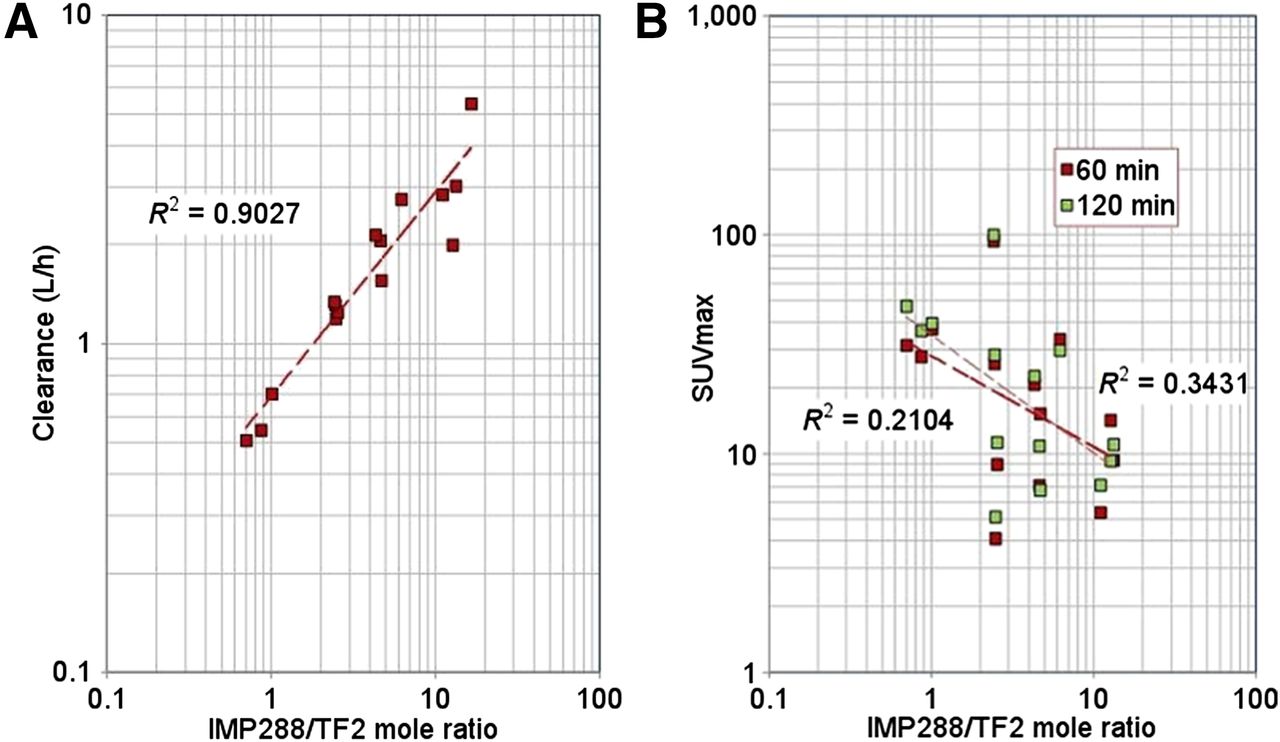
Correlation between IMP288 clearance (A) or SUVmax (B) and IMP228 to TF2 ratio. IMP288 clearance (A), estimated for each patient according to population pharmacokinetics analysis, or SUVmax (B) were plotted (log–log plot) against ratio of number of moles of injected IMP288 to number of moles of TF2 present in circulation at time of IMP288 injection. Correlation coefficients for power function regression (dotted lines) are shown in figure.
DISCUSSION
To our knowledge, this study is the first-in-human demonstration of the feasibility of pretargeted immuno-PET using the trivalent humanized TF2 BsMAb and 68Ga-IMP288 peptide. The previous clinical study assessing TF2 and 177Lu-IMP288 in metastatic colorectal patients showed selective tumor uptake within 1 h of peptide injection and high tumor-to-tissue uptake ratios at 24 h. The best tumor targeting was achieved with a 24-h pretargeting interval, a high TF2 dose (150 mg, 955 nmol), and a low (25 μg, 17.5 nmol) peptide dose (14). Prepretargeting radioimmunotherapy (pRIT) 111In-IMP288 immunoscintigraphy showed good tumor targeting with a better contrast when the IMP288 dose was reduced. In our pRIT study assessing the same compounds in lung cancer patients, similar conclusions were reached with regard to the best pretargeting conditions: a pretargeting delay of 24 h, a TF2 dose of 480 nmol/m2, and an IMP288 dose of 24 nmol/m2 (17). However, the constraints for therapy and imaging are different: for therapy, the injected activity must be high, which sets a minimum for the amount of injected IMP288, and the dose to the tumor must be maximum, not necessarily the tumor-to-organ ratios. The population pharmacokinetics analysis of this immuno-PET study showed a good correlation between IMP288 clearance and the molar ratio of injected IMP288 to circulating TF2 at the time of IMP288 injection. This means that increasing the molar dose of IMP288 or the pretargeting delay will increase IMP288 clearance. Moreover, if the correlation between this molar ratio and SUVmax was not as good as that of IMP288 clearance, the expected trend of lower tumor uptake for higher ratio was observed. Thus, a faster clearance of activity reduces background but also reduces tumor uptake and the optimum that may be achieved.
According to a PET visual and semiquantitative analysis, the 30-h pretargeting delay seemed to be the most favorable. Moreover, even if good imaging performances were observed in cohorts C2 and C4 using 120 nmol of TF2 and a 30-h pretargeting delay, a TF2-to-IMP288 molar ratio of 20 in C2 appeared better than 40 in C4. Indeed, even if tumor uptake appeared to be higher, with the 40-molar ratio, with tumor SUVmax increasing in the 3 patients between 60 and 120 min, the blood activity also seemed higher as shown by concordant semiquantitative PET (higher MBP uptake in C4 than in C2) and pharmacokinetics results (decrease of hapten clearance), because the higher TF2 blood concentration causes a more efficient formation of peptide–BsMAb complexes (14,15). This relatively high blood activity diminishes tumor detectability, as shown in Figure 1. However, the increase of tumor uptake between 60 and 120 min in C4 suggests that a longer half-life PET emitter allowing later PET imaging would be more favorable than 68Ga for a 40-molar dose ratio. If a hapten radiolabeling with 18F could also be envisaged using IMP449, this peptide is not currently available for clinical use. Moreover, 64Cu (half-life of 12.7 h) should be preferred, allowing delayed images up to 48 h after the hapten injection (18,19). Additionally, the reduced peptide dose makes the labeling more difficult, requiring high specific activity, which may not be achieved at the end of the life of the 68Ga generator.
C5 was set to test whether a lower dose (60 nmol) of TF2 could give similar imaging performance. A large pharmacokinetics variability, in agreement with semiquantitative PET observations, was observed in this cohort. Schoffelen et al. also described a considerable variability in IMP288 blood residence times in patients who received the lowest TF2 and IMP288 doses, despite a favorable imaging contrast (14,15). In C5, patients 14 and 15 showed good tumor uptake but also high MBP concordant with slow TF2 and hapten clearances. The image contrast was not optimal and was improved by later PET imaging with increased tumor uptake and T/MBP ratio between 60 and 120 min. By contrast, patient 16 showed fast TF2 and hapten clearances, concordant with the low MBP activity. High blood CEA concentration could accelerate the clearance of anti-CEA immunoglobulin because of antigen–antibody complexes formed in serum (20), but the plasma CEA concentration was low (3 ng/mL) in this patient. The only clinically relevant parameter registered in this patient was a primary polycythemia diagnosed in the weeks after immuno-PET. Thus, the C2 protocol (120 nmol of TF2, 6 nmol of IMP288, and 30-h pretargeting delay) was considered the most favorable for PET imaging and the most reproducible in clinical practice.
This study confirmed the hypothesis previously proposed in our pRIT study that systematic intravenous injection of corticosteroids and antihistamines before TF2 injection may induce transient immunosuppression, limiting immediate and delayed immune effects. No immediate immune effects were reported during or after TF2 infusion, and the immunization rate in our 2 studies (3/19) was lower than previously described by Schoffelen et al. (11/21) using the same compounds (14,15). A grade 3 adverse event was observed immediately after the IMP288 infusion, suggesting an immune reaction to hapten as previously described using di-DTPA-indium hapten (16). Therefore, the protocol was amended, and a premedication with antihistamine and corticosteroid before both TF2 and IMP288 injections was given to all patients. The low immunogenicity observed under these conditions also represents a favorable element for the use of immuno-PET as a theranostic approach, for example, to select patients for pRIT.
Pretargeted immuno-PET detected MTC foci in all patients except one. The sensitivity of the technique will be evaluated in the second part of the study, but these preliminary results already suggest that high tumor contrast can be obtained using this novel whole-body imaging. Our previous studies showed that CEA expression seemed to be almost constant in MTC and that high sensitivity PET imaging using CEA as a target would detect the disease independently of the prognosis, in contrast to 18F-FDG or 18F-DOPA PET/CT (4–6). Moreover, on the basis of the lung cancer pRIT study, we estimate that the induced internal radiation exposure resulting from 68Ga-IMP288 injection is low, with an effective dose obtained using MIRD S factors of 1.9 ± 1.2 mSv equivalent to 18F-FDG, which was estimated to be 2.3 mSv for the same injected activity (21).
An increased interest for immuno-PET is found in the recent literature (9,10), in which targeted therapies using antibodies are experiencing a considerable growth in cancer management. On the basis of immuno-PET, treatment strategies could be tailored for individual patients before the administration of expensive and potentially toxic therapies. Immuno-PET can offer a noninvasive solution to quantitatively assess target expression. For example, anti–human epidermal growth factor receptor 2 (Her2) therapeutic agents are only effective in patients who have Her2-positive breast cancer, and immunoconjugates labeled with 68Ga, 64Cu, or 89Zr could noninvasively identify lesions that are likely to respond to therapy (19,22,23). Pretargeted immuno-PET could be a specific diagnostic tool for tumor detection but also a theranostic/companion approach to select patients to be treated with radioimmunoconjugates or antibody–drug conjugates.
CONCLUSION
This clinical study demonstrated the feasibility of immuno-PET using the anti-CEA humanized trivalent BsMab TF2 and the 68Ga-IMP288 hapten. We determined that 120 nmol of TF2, 6 nmol of peptide, and a 30-h pretargeting delay seemed to be the best parameters for clinical practice. The sensitivity of this novel imaging method in relapsing MTC patients, in comparison with conventional imaging, will be assessed in the second part of the study, but present results already show that high-contrast tumor uptake can be obtained.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by grants from the French DHOS INCA in 2010, the French National Agency for Research, IRON Labex ANR-11-LABX-0018-01, and ArronaxPlus Equipex ANR-11-EQPX-0004. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
TF2 and IMP288 were provided by Immunomedics, Inc., and IBC Pharmaceuticals, Inc.
Footnotes
Published online May 26, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication January 6, 2016.
- Accepted for publication April 7, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pretargeting: A Path Forward for Radioimmunotherapy
- Anti-CEA Pretargeted Immuno-PET Shows Higher Sensitivity Than DOPA PET/CT in Detecting Relapsing Metastatic Medullary Thyroid Carcinoma: Post Hoc Analysis of the iPET-MTC Study
- Current Landscape in Clinical Pretargeted Radioimmunoimaging and Therapy
- Initial Clinical Results of a Novel Immuno-PET Theranostic Probe in Human Epidermal Growth Factor Receptor 2-Negative Breast Cancer
- Pretargeted Imaging and Therapy
- PET Imaging for Endocrine Malignancies: From Woe to Go