


Abstract
This study evaluated the impact of 68Ga-DOTATOC PET/CT in detecting recurrence or metastases in differentiated thyroid carcinoma (DTC) patients with elevated serum thyroglobulin and both negative radioiodine imaging and negative 18F-FDG PET/CT. Methods: 68Ga-DOTATOC PET/CT (CT without contrast, low-dose) was performed on average 6 wk after negative 18F-FDG PET/CT (CT contrast-enhanced, full-dose) in 15 consecutive radioiodine-negative DTC patients with elevated and rising thyroglobulin. Visual assessment of 68Ga-DOTATOC PET/CT images used a 4-point scale for classification of lesions (0, no pathologic findings; 1, benign; 2, equivocal; 3, malignant). PET findings were correlated with the histologic subtype of tumor, levels of serum thyroglobulin, and morphologic findings on full-dose CT and neck ultrasound. Histology or clinical and imaging follow-up served as a reference standard. Analysis was performed on a patient and lesion basis. Results: 68Ga-DOTATOC PET/CT was true-positive in 5 patients (10 tumor lesions) and was false-positive in 1 patient. The rate of positive 68Ga-DOTATOC PET/CT was significantly higher in poorly differentiated/oxyphilic carcinomas (4/4 patients) than in papillary (1/5) or follicular (0/6) tumors. Thyroglobulin levels tended to be higher in patients with tumor localization on 68Ga-DOTATOC PET/CT, but differences were not significant. In 2 of 5 patients with true-positive findings on 68Ga-DOTATOC PET/CT, CT alone but not ultrasound identified 2 of 10 tumor lesions, but in both patients 68Ga-DOTATOC-PET/CT revealed further tumor lesions not detected on CT alone. Conclusion: 68Ga-DOTATOC PET/CT should be considered in the case of negative 18F-FDG PET/CT in radioiodine-negative DTC patients with elevated and rising thyroglobulin. Imaging with 68Ga-DOTATOC appears promising especially in poorly differentiated and oxyphilic subtypes of DTC.
Differentiated thyroid carcinomas (DTCs) have generally excellent prognosis after initial surgery and radioiodine treatment. However, tumor recurrence is quite common, with a relapse rate of up to 20% (1). Even in the case of relapse or metastasis, iodine-accumulating tumors can be effectively treated with radioiodine. But once DTCs lose the capability to concentrate (radio)iodine, they can be challenging to treat (2). The recently established molecularly targeted therapy for patients with locally advanced or metastatic radioiodine-refractory tumors was shown to extend progression-free survival, but patients failed to achieve complete remission (3). Currently, there are no curative systemic treatment options for metastatic radioiodine-refractory tumors. As long as these tumors are locally limited, they can be removed surgically or at least controlled by external radiation. Consequently, long-term local tumor control or even cure is achievable, provided that the tumor can be localized early enough. 18F-FDG PET/CT is an established tool for detection of recurrent DTCs in patients presenting with elevated and rising thyroglobulin levels after radioiodine ablation and negative radioiodine scans (1,4). However, 18F-FDG PET/CT fails to localize the tumor in some of these patients.
DTCs were shown to express somatostatin receptors (SSTRs) (5–10). As a result, several imaging studies using radiolabeled SSTR analogs such as 111In-pentetreotide or 99mTc-depreotide were performed in DTC to date (11–19). However, the patient populations investigated in these studies were heterogeneous and only few studies have investigated the impact of SSTR scintigraphy in DTC patients with elevated thyroglobulin, indicating disease recurrence, and negative radioiodine imaging (11–13,16,19). Controversial results were reported about SSTR scintigraphy compared with 18F-FDG PET/CT in iodine-positive and iodine-negative DTC (12,14,16). PET has several advantages over planar scintigraphy or even SPECT such as better spatial resolution allowing for the detection of smaller lesions. In recent years, SSTR-binding PET tracers such as 68Ga-DOTATOC were established in clinical routine. To our knowledge, only 3 studies have compared the diagnostic performance of 68Ga-labeled SSTR analogs (DOTATOC, DOTANOC, DOTALAN PET/CT) with 18F-FDG PET/CT in the staging of iodine-negative DTC so far (20–22). Padhy et al. reported their initial experience of 68Ga-DOTATATE PET/CT in identifying non–iodine-avid/non-18F-FDG–avid disease in patients with DTC (23). However, studies focusing on the usefulness of 68Ga-labeled SSTR-binding PET tracers in DTC patients with elevated thyroglobulin and both negative radioiodine imaging and negative 18F-FDG PET/CT have not yet been reported.
The aim of this study was to evaluate the impact of 68Ga-DOTATOC PET/CT in detecting recurrence or metastases in radioiodine-negative DTC patients with elevated serum thyroglobulin and negative 18F-FDG PET/CT.
MATERIALS AND METHODS
Patients
This retrospective study included 15 consecutive DTC patients with negative radioiodine and 18F-FDG imaging as well as elevated and rising serum thyroglobulin levels (7 women and 8 men; mean age at the time of initial surgery, 57 y; age range, 19–76 y). Tumor histology was papillary thyroid carcinoma in 5 patients, follicular thyroid carcinoma in 6 patients, poorly differentiated carcinoma in 3 patients, and oxyphilic (Hürthle cell) thyroid carcinoma in 1 patient. Most patients presented initially with locally advanced tumor stage (T3 or T4 according to the Union Internationale contre le cancer, seventh edition 2010; 11 patients) or lymph node metastases (5 patients). After total thyroidectomy, all patients were treated with at least 1 radioiodine therapy (median cumulative activity, 8 GBq of 131I; range, 3–11 GBq) 1–19 y (median, 7 y) ago. In addition to radioiodine therapy, 1 patient underwent resurgery and external radiation therapy. Follow-up care routinely included high-resolution ultrasound of the neck (iU22; Philips) and determination of the tumor marker serum thyroglobulin (SELco Tg; Medipan) under thyroid-stimulating hormone (TSH) suppressive treatment with L-thyroxine or under TSH stimulation. Thyroglobulin recovery testing was performed for detecting interference in serum thyroglobulin measurement. Additionally, interfering thyroglobulin antibodies (Anti-TG; Siemens) were determined.
All patients presented with elevated and rising thyroglobulin levels during follow-up. Consecutive whole-body radioiodine imaging (131I-whole-body scan in 8 patients and 124I-PET/CT in 7 patients) under endogenous TSH stimulation (TSH > 30 mU/L) was assessed as negative in all patients by 2 experienced nuclear medicine physicians in consensual diagnosis. All patients followed a low-iodine diet for 4 wk before radioiodine imaging, and measurement of iodine urinary concentration excluded iodine excess.
Patient characteristics and the corresponding results of 68Ga-DOTATOC PET/CT are summarized in Table 1.
Patient Characteristics and Results of 68Ga-DOTATOC PET/CT
The study has been approved by the local ethics committee, and all patients signed an informed consent form.
18F-FDG PET/CT Imaging
18F-FDG PET/CT (CT contrast-enhanced, in full-dose technique) was performed for detection of iodine-refractory thyroid carcinoma at a median 3 mo after radioiodine imaging. PET/CT images were obtained using a Biograph mCT PET/CT scanner (Siemens Healthcare). Before tracer administration, a fasting period of at least 4 h and blood glucose levels lower than 150 mg/dL were assured. After intravenous administration of 250–350 MBq (median, 325 MBq) of 18F-FDG, PET data were acquired 57–70 min (median, 60 min) after injection by scanning from the upper thigh to the head using 6–8 bed positions for 2 min each. The PET data were reconstructed using a 3-dimensional attenuation-weighted ordered-subsets expectation maximization algorithm with 4 iterations and 8 subsets, a 4-mm postreconstruction gaussian filter, and attenuation image segmentation. Diagnostic CT was performed after administration of oral and intravenous contrast medium. Attenuation correction of the PET data was based on the acquired whole-body CT dataset. CT acquisition parameters were as follows: 100 kV; automatic mA adjustment (maximum, 210 mAs); slice thickness, 5 mm; increment, 5 mm; pitch, 1. 18F-FDG PET/CT studies were evaluated by 2 independent, experienced nuclear medicine physicians and a radiologist in consensual diagnosis. Lesions were considered malignant if focal 18F-FDG uptake was noted. 18F-FDG imaging was assessed as negative in all patients. CT revealed 2 pathologic findings without 18F-FDG accumulation assessed as not clearly benign or malignant.
68Ga-DOTATOC PET/CT Imaging
Because no tumor site was detected on radioiodine and on 18F-FDG imaging, all patients underwent a 68Ga-DOTATOC PET/CT scan. The mean interval between 18F-FDG PET/CT and 68Ga-DOTATOC PET/CT scanning was 6 wk (range, 1–12 wk). 68Ga-DOTATOC was synthesized in-house as previously described (24). No patients received treatment with somatostatin analogs. PET data were acquired 28–40 min (median, 30 min) after intravenous administration of 60–100 (median, 78) MBq of 68Ga-DOTATOC from the upper thigh to the head using 6–8 bed positions for 2 min each. Scans were acquired using a Biograph mCT (Siemens Healthcare) scanner. CT data were used for attenuation correction. The PET data were reconstructed using a 3-dimensional attenuation-weighted ordered-subsets expectation maximization algorithm with 4 iterations and 8 subsets, a 4-mm postreconstruction gaussian filter, and attenuation image segmentation. To minimize radiation exposure, CT was performed without contrast in low-dose technique with 15 mAs; 100 kV; slice width, 5 mm; increment, 5 mm; and pitch, 0.85, and served only for attenuation correction of the PET data and anatomic orientation.
68Ga-DOTATOC PET/CT Data Analysis and Statistics
68Ga-DOTATOC PET studies were retrospectively evaluated by 2 independent, experienced nuclear medicine physicians in consensual diagnosis. Visual assessment of PET images used a 4-point scale for classification of lesions (0, no pathologic findings; 1, benign; 2, equivocal; 3 = malignant). Lesions were considered malignant if marked, focal 68Ga-DOTATOC uptake above background was noted in a location incompatible with physiologic tracer uptake. If mild uptake near background level was observed, lesions were assessed as benign. Lesions were assessed as equivocal if assignment as benign or malignant was uncertain. We also measured the SUVmax of lesions, but because there is no generally accepted SUVmax threshold to define malignancy, we did not use a fixed threshold for differentiating between benign and malignant findings. Analysis was performed on a patient and lesion basis. Findings were verified by histology or clinical follow-up, including different imaging modalities.
Results of the 68Ga-DOTATOC PET/CT were correlated with initial tumor histology (papillary, follicular, and less differentiated oxyphilic/poorly differentiated carcinomas) and levels of serum thyroglobulin under TSH-suppressive therapy at the time of 68Ga-DOTATOC PET/CT.
The PET lesions were compared with the full-dose CT of the 18F-FDG PET/CT and were rated as without morphologic correlate or with morphologic correlate. Lesions with morphologic correlate were further classified as inconspicuous, not clearly benign or malignant, or highly suspicious of malignancy on CT alone to define whether a 68Ga-DOTATOC–positive lesion was recognized as malignant on CT alone.
Additionally, high-resolution ultrasound of the neck (iU22; Philips) was performed for detection of local recurrence or suspected lymph nodes. Findings were compared with the results of 68Ga-DOTATOC PET/CT.
Statistical analysis was performed using the Prism 5 software package (GraphPad Software). Thyroglobulin values were compared between patients with positive and negative 68Ga-DOTATOC PET/CT and between histologic subtypes using the nonparametric Mann–Whitney test or Kruskal–Wallis test followed by Dunn multiple comparison test. To exclude bias due to tumor progress over time, thyroglobulin levels at the time of radioiodine imaging were compared with those at 68Ga-DOTATOC PET/CT using a paired t test. Patient-based analysis of positive findings on 68Ga-DOTATOC PET/CT in dependence of histology was performed using the Fisher exact test. In all analyses, a P value of less than 0.05 was considered to indicate statistical significance.
RESULTS
68Ga-DOTATOC PET/CT
68Ga-DOTATOC PET/CT was negative for malignant lesions in 9 patients: PET was completely negative in 6 of 15 patients. In 2 of 15 patients, only benign lesions were detected. Findings were rated as equivocal in 1 of 15 patients. In all of these 9 patients, the absence of detectable malignant lesions was confirmed during follow-up (median follow-up, 22 mo; range, 16–40 mo).
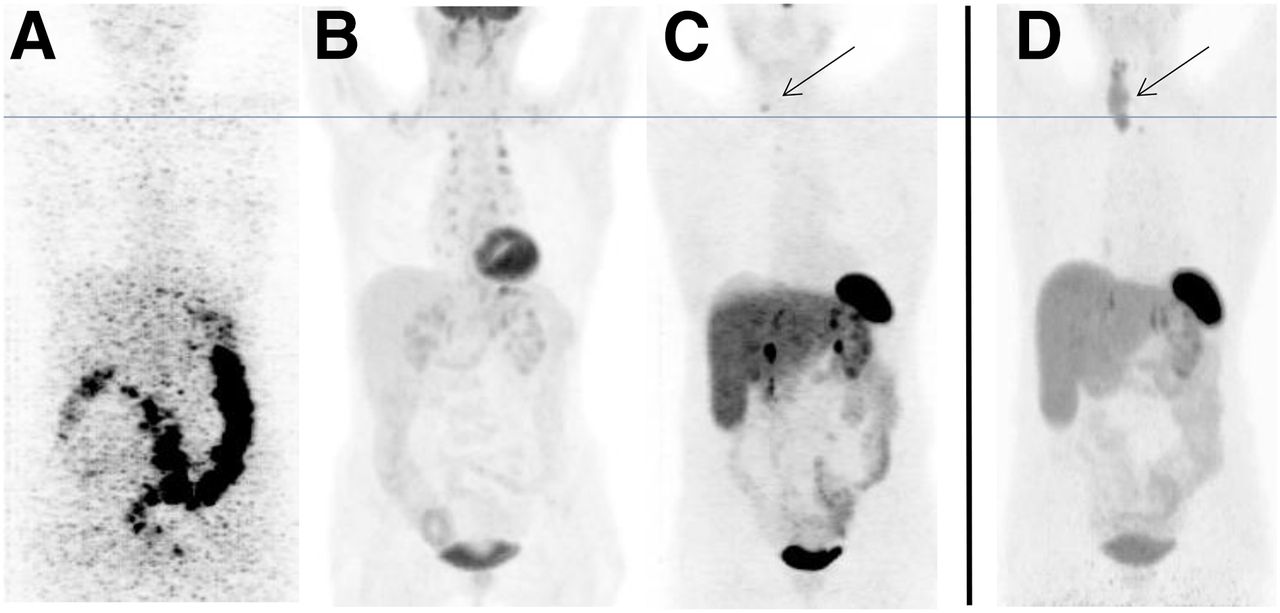
In 6 of 15 patients, at least 1 lesion was considered as malignant (mean SUVmax, 4.8; range, 3.0–10.1). An example is given in Figure 1. Assessment was verified as true-positive in 3 of 6 patients by histologic confirmation, in 1 patient by fine-needle aspiration biopsy before external radiation therapy, and in 1 patient by progressive disease during follow-up. In 1 of 6 patients, focal uptake in a mesenteric lymph node assessed as suspected as neuroendocrine tumor turned out to be false-positive because it showed no tracer accumulation on follow-up 68Ga-DOTATOC PET/CT. Therefore, 68Ga-DOTATOC PET/CT allowed the localization of tumor sites in 5 of 15 (33%) patients with elevated thyroglobulin and negative radioiodine and 18F-FDG imaging. In these patients, 10 malignant lesions were detected by 68Ga-DOTATOC PET/CT. In detail, 7 cervical (including 3 in the cervicothoracic region), 1 axillary, and 2 mediastinal tumor sites (local relapse or lymph node metastases) were identified.

Patient 8 (according to Table 1) with oxyphilic thyroid carcinoma who presented with elevated thyroglobulin (32 ng/mL). Tumor relapse was not detected on either 124I-PET/CT (A) or ultrasound or on 18F-FDG PET/CT (B), whereas 68Ga-DOTATOC PET/CT revealed a small tumor lesion on right side of neck (C, arrow). Patient refused surgery at time of 68Ga-DOTATOC PET/CT. (D) Progressive, but still locally limited disease was diagnosed 15 mo later (arrow).
Tumor Histology and Thyroglobulin Level: Correlation with Detection Rate on 68Ga-DOTATOC PET/CT
When the different histologic tumor subtypes were considered, the tumor detection rate on 68Ga-DOTATOC PET/CT was 1 of 5 for patients with papillary carcinoma, 0 of 6 for follicular tumors, and 4 of 4 for the group of poorly differentiated and oxyphilic carcinomas. Statistical analysis revealed significance between poorly differentiated/oxyphilic and papillary carcinomas (P < 0.05) and between poorly differentiated/oxyphilic and follicular carcinomas (P < 0.01), whereas difference between papillary and follicular carcinomas was not significant (P = 0.45).
All patients presented with elevated and rising thyroglobulin levels under TSH suppression (11 patients) or under TSH stimulation (4 patients). Recovery testing was within the normal reference range in all patients. One patient was excluded from thyroglobulin analysis because he presented, in addition to elevated and rising thyroglobulin levels, with increasing thyroglobulin antibodies during follow-up.
We found no significant differences (P = 0.40) between unstimulated thyroglobulin levels at the time of radioiodine imaging (median, 14 ng/mL) and 68Ga-DOTATOC PET/CT (median, 16 ng/mL), thus excluding bias due to tumor progress between radioiodine imaging and SSTR imaging.
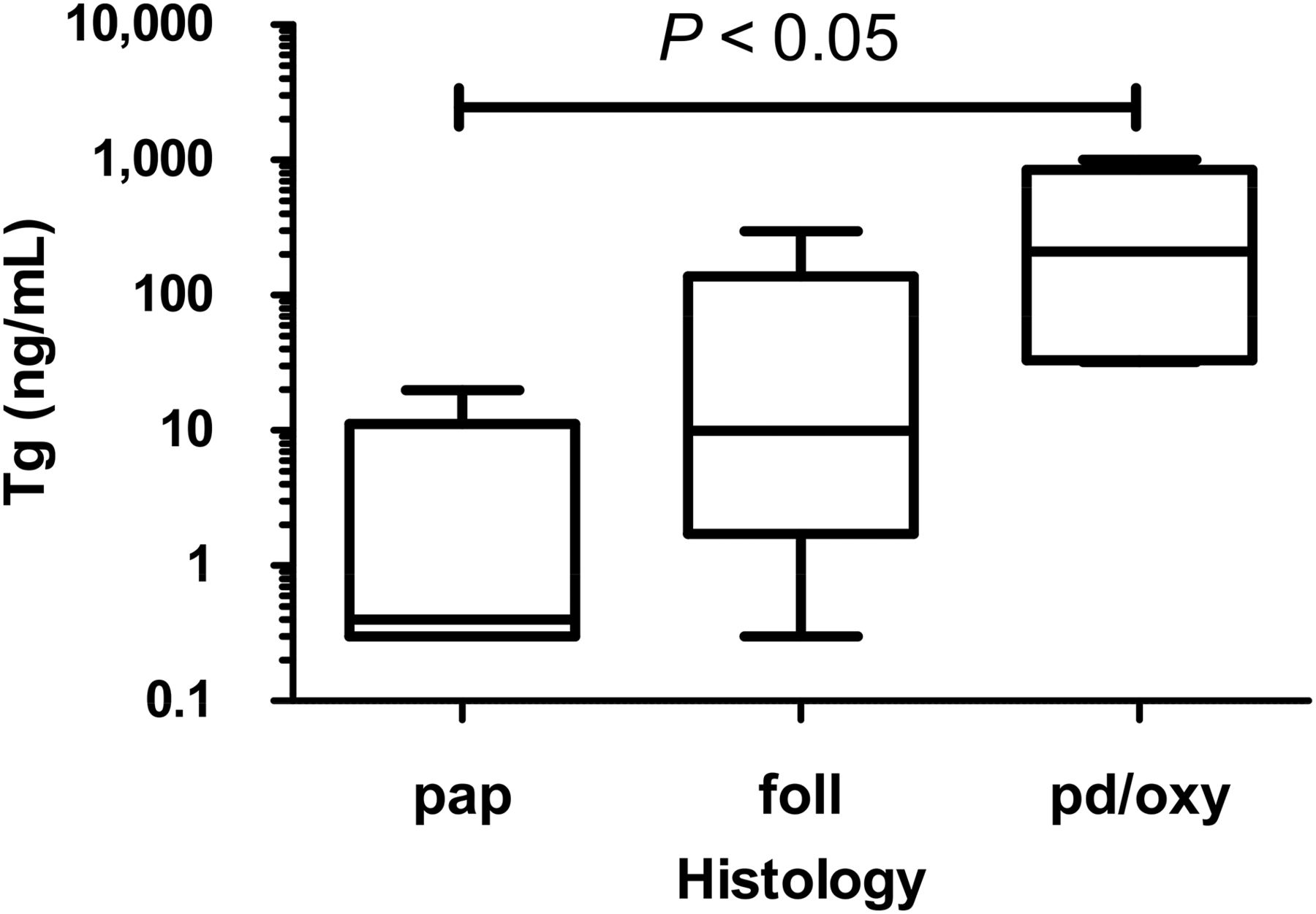
At the time of 68Ga-DOTATOC PET/CT, unstimulated thyroglobulin levels were significantly higher in the group of poorly differentiated/oxyphilic carcinomas (median, 211 ng/mL; range, 32–1,000 ng/mL) than in papillary carcinomas (median, 0.4 ng/mL; range, 0.3–19.9 ng/mL), whereas we found no significant differences between poorly differentiated/oxyphilic and follicular carcinomas (median, 16 ng/mL; range, 0.3–299 ng/mL) or between papillary and follicular carcinomas (Fig. 2).
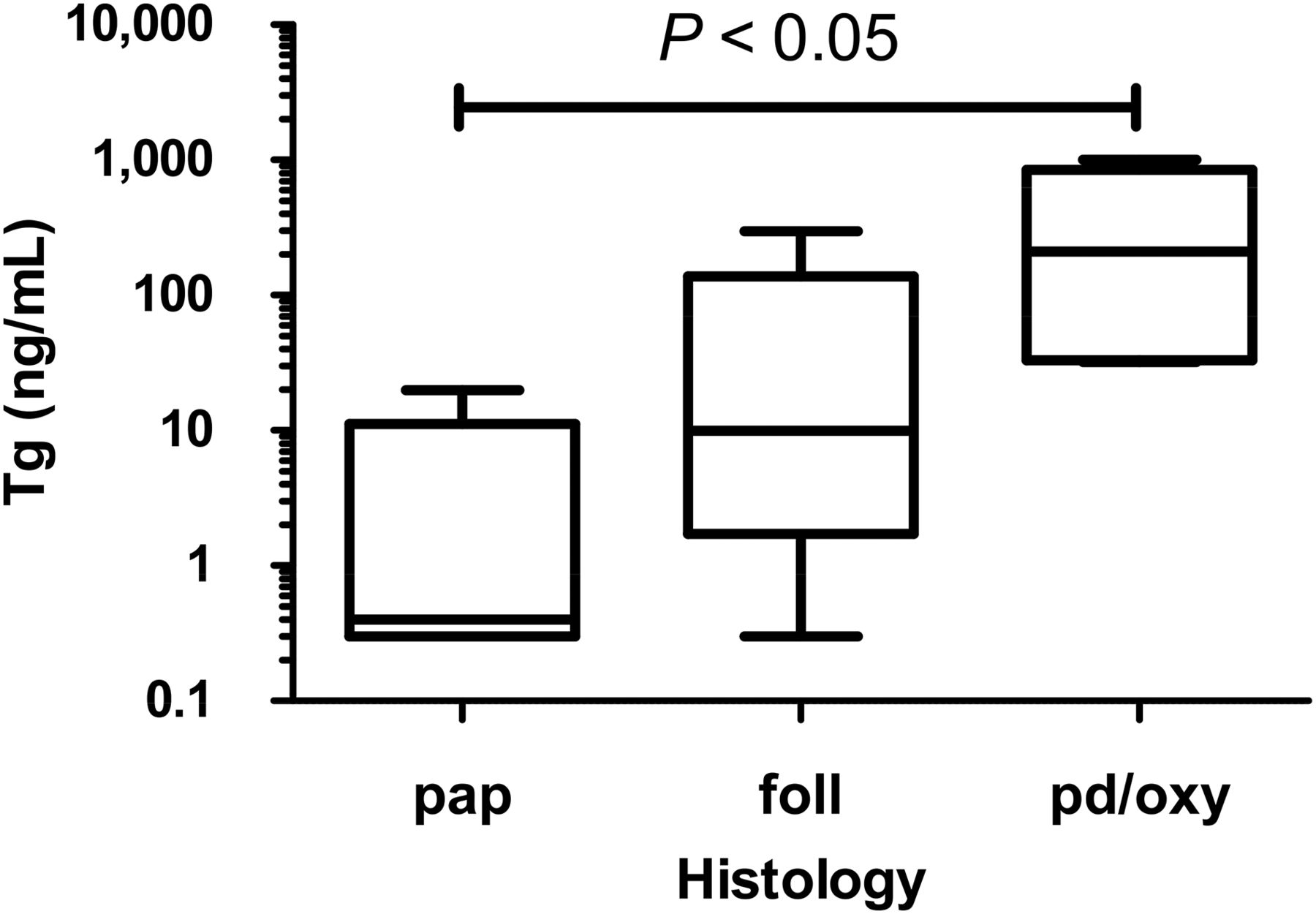
Serum thyroglobulin (Tg) levels in different subtypes of DTC. Statistical significance was found between poorly differentiated/oxyphilic and papillary carcinomas. Box plot illustrates 25th and 75th percentile (box), median (middle bar in box), and range (whiskers). foll = follicular carcinoma; pap = papillary carcinoma; pd/ox = poorly differentiated/oxyphilic carcinoma.
Thyroglobulin levels under TSH-suppressive therapy tended to be higher in patients with positive 68Ga-DOTATOC PET/CT (median, 36 ng/mL; range, 0.3–1,000 ng/mL) than in patients with negative 68Ga-DOTATOC PET/CT (median, 3 ng/mL; range, 0.3–299 ng/mL), but differences were not significant (P = 0.16) (Fig. 3).

Thyroglobulin (Tg) levels in patients with positive and negative findings on 68Ga-DOTATOC PET/CT. Box plot illustrates 25th and 75th percentile (box), median (middle bar in the box), and range (whiskers). ns = not significant.
Pathologic Findings on CT and Ultrasound of the Neck
On full-dose CT, 8 of the 10 tumor lesions detected on 68Ga-DOTATOC PET/CT showed a morphologic correlate. But only 2 of these 8 CT lesions could be categorized as pathologic on CT alone. In detail, the 2 SSTR-positive lesions with pathologic finding on CT presented as local relapse with little contrast enhancement in the thyroid bed (lesion 1) and as mediastinal lymph node that slightly exceeded size criteria but showed no contrast enhancement and could not be clearly differentiated from benign reactive lymphadenopathy (lesion 2). Both lesions were assessed as not clearly malignant, but needs to be closely monitored. Considering the remaining 6 PET-positive lesions with correlate but no pathologic findings on CT, we found 4 SSTR-positive lymph nodes that did not exceed the size criteria to suspect malignancy and 2 lesions in the thyroid bed that could not be differentiated from postoperative changes on CT alone.
The 2 SSTR-positive lesions with pathologic finding on CT were found in 2 patients who presented with at least one further 68Ga-DOTATOC–positive tumor lesion that would not have been characterized as malignant on CT alone. From the other 3 patients with SSTR-positive tumor sites, 1 patient did not show any morphologic correlate on CT. To summarize, in all 5 patients with tumor detection on 68Ga-DOTATOC PET/CT, at least 1 tumor site would not have been identified on CT alone. Moreover, we did not find any suspected lesions on CT that were 68Ga-DOTATOC–negative.
Ultrasound of the neck did not categorize any of the 10 68Ga-DOTATOC–positive lesions as malignant. The enlarged lymph node found on CT could not be detected by ultrasound because of its mediastinal location. The local relapse with contrast enhancement on CT was assessed as postoperative change by ultrasound. The remaining tumor sites identified on 68Ga-DOTATOC imaging were classified as benign reactive lymph nodes or could not be detected.
DISCUSSION
This study demonstrates the capability of 68Ga-DOTATOC-PET/CT to localize tumor relapse or metastases in DTC patients who were unsuccessfully restaged before. Thus, we could localize tumor lesions in 5 of 15 patients who had negative findings on ultrasound, radioiodine imaging, and 18F-FDG PET/CT. Considering the ineffective preceding imaging effort, a detection rate of 33% is substantially high and emphasizes the diagnostic value of 68Ga-DOTATOC PET/CT in iodine- and 18F-FDG–negative DTC with elevated and rising thyroglobulin.
Compared with SSTR PET/CT, 18F-FDG PET/CT was reported to be more sensitive in detecting tumor lesions in previous studies. Yet, in accordance with our results some lesions were detected only with SSTR PET/CT (20–22). Differences in lesion detection between 18F-FDG and SSTR PET/CT may be the result of different DTC subtypes being studied.
Binding of SSTR analogs and as a result tumor detection rates on SSTR imaging appear to differ between histologic subtypes of DTC. In our study, 68Ga-DOTATOC PET/CT identified tumor relapse in all patients with poorly differentiated tumors (3 patients) and oxyphilic carcinoma (1 patient). Whereas SSTR scintigraphy was reported to be a promising tool in oxyphilic carcinoma in several studies before (6,9,12,19,25), reports about SSTR imaging in poorly differentiated thyroid carcinomas are rare (14,26). Although almost all oxyphilic and poorly differentiated tumors were shown to express SSTR in these studies, 18F-FDG PET/CT was superior to SSTR scintigraphy in most cases. Studies having performed more sensitive SSTR PET reported about 2 of 4 SSTR-positive oxyphilic carcinomas (22) or included only papillary and follicular carcinomas (20,21). In the latter 2 DTC subtypes, variable proportions of SSTR-positive tumors were described before. However, even compared with studies that performed less-sensitive scintigraphy (12,14,15,25,26), the rate of SSTR-positive findings on 68Ga-DOTATOC PET/CT was considerably low in patients with papillary (tumor localized in 1/5 patients) and follicular (no tumor localized in 6 patients) tumors in our cohort. This discrepancy between our and previous studies may be due to different patient or tumor characteristics; for example, other studies also included iodine-positive DTC.
Because follicular cells of the thyroid express SSTR, one would expect tumors of follicular origin to express SSTR. Loss of SSTR expression may indicate a lower grade of differentiation as observed in other tumor entities. Yet, it remains unclear whether SSTR expression in DTC is associated with tumor behavior and in consequence patient outcome. Reporting SSTR expression in both iodine-positive and -negative DTC as well as in 18F-FDG–positive and –negative DTC, previous studies revealed no correlation between SSTR expression and differentiation degree of DTC. These observations speak against a flip-flop phenomenon between SSTR expression and iodine accumulation or 18F-FDG uptake as suggested by Feine et al. and Rodrigues et al. (17,27), respectively.
Higher thyroglobulin levels are supposed to enhance detectability of tumors on SSTR imaging. Thyroglobulin levels tended to be higher in patients with positive findings on 68Ga-DOTATOC PET/CT than in those with negative findings, but differences were not significant. However, results were different with regard to DTC subtypes: thyroglobulin levels were significantly higher in the group of poorly differentiated/oxyphilic carcinomas than in papillary tumors. Yet, differences in thyroglobulin levels were not significant between poorly differentiated/oxyphilic carcinomas and follicular carcinomas. Consequently, factors other than the tumor burden affect the detectability on SSTR imaging.
Nonetheless, according to American Thyroid Association guidelines 18F-FDG PET may be performed if the thyroglobulin level is greater than 10 ng/mL. This cutoff value might not be applicable to SSTR PET because the lowest thyroglobulin value in a patient with confirmed tumor localization on 68Ga-DOTATOC PET/CT was 0.3 ng/mL. Furthermore, we found a wide range of overlapping thyroglobulin values between patients with positive and negative findings on 68Ga-DOTATOC PET/CT.
Early detection of tumor relapse on 68Ga-DOTATOC PET/CT and as a result early therapy may prevent the tumor to progress from locally limited to widespread metastatic disease and thus improve patient outcome. In our cohort, 3 of the 5 patients with positive findings on 68Ga-DOTATOC PET/CT presented with tumor lesions that all could be removed surgically, in 1 patient local tumor control was obtained by external radiation therapy, and in 1 patient mediastinal tumor rendered local therapy impossible. 68Ga-DOTATOC PET/CT may be useful also in patients with distant metastases for evaluation of peptide receptor radionuclide therapy, thus offering a systemic treatment option with considerably mild adverse effects in the case of SSTR-expressing tumors. However, in the patient with mediastinal tumor peptide receptor radionuclide therapy was not performed because of relatively low tumor uptake.
Whereas several studies have shown that 18F-FDG PET/CT is superior to morphologic imaging such as CT in iodine-negative DTC (28–30), studies about that issue have not yet been reported for SSTR PET/CT in DTC. In gastroenteropancreatic neuroendocrine tumors, higher sensitivity of SSTR PET/CT than CT alone was reported (31). Consistently, CT identified only 2 of 10 SSTR-positive tumor lesions in 2 patients in our study, but in both patients 68Ga-DOTATOC PET revealed further tumor sites not detected on CT. Our results confirm the advantage of functional imaging especially in small lymph node metastases and in differentiating local tumor relapse from postoperative changes. However, for achieving better anatomic correlation we recommend performing full-dose CT in PET/CT particularly if surgery is intended.
There are some limitations of this study: first, the sample size was relatively small because of strict inclusion criteria. Thus, our study included only patients who were unsuccessfully restaged before. In addition, our study was retrospective in nature. Finally, although the detection of tumor relapse on 68Ga-DOTATOC PET/CT offered a therapy option, the relevance for patient outcome remains unclear and requires long-term follow-up in usually slowly progressive DTC.
To sum up, 68Ga-DOTATOC PET/CT could localize the tumor relapse in 5 of 15 DTC patients and offered a treatment option in 4 of 15 patients.
CONCLUSION
68Ga-DOTATOC PET/CT is a promising tool in DTC patients with elevated thyroglobulin and negative radioiodine imaging and should be considered especially in poorly differentiated and oxyphilic subtypes of DTC if 18F-FDG PET/CT fails to localize the tumor relapse.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 31, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 29, 2015.
- Accepted for publication February 29, 2016.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- SNMMI Procedure Standard/EANM Practice Guideline for Nuclear Medicine Evaluation and Therapy of Differentiated Thyroid Cancer: Abbreviated Version
- Appropriate Use Criteria for Nuclear Medicine in the Evaluation and Treatment of Differentiated Thyroid Cancer
- Current Treatment Strategies in Metastasized Differentiated Thyroid Cancer
- A New Theranostic Paradigm for Advanced Thyroid Cancer