


Abstract
The purpose of this study was to compare the diagnostic accuracy of whole-body unenhanced PET/MR with that of PET/CT in determining the stage of non–small cell lung cancer. Methods: This study was approved by the institutional review board and by national government authorities. Forty-two consecutive patients referred for the initial staging of non–small cell lung cancer underwent whole-body imaging with a sequential trimodality PET/CT/MR system. PET/MR and PET/CT datasets were evaluated separately, and a TNM stage was assigned on the basis of the image analysis. Nodal stations in the chest were identified according to the mapping system of the American Thoracic Society. The standard of reference was histopathology for the tumor stage in 20 subjects, for the nodal stage in 22 patients, and for extrathoracic metastases in 5 subjects. All other lesions were confirmed by at least 1 different imaging method. A Wilcoxon signed-ranks test was used for comparing PET/MR with PET/CT. Results: PET/MR did not provide additional information compared with PET/CT. The diagnostic accuracy of both imaging modalities was equal (T staging, P = 0.177; N staging, P = 0.114; M staging, P = 0.465), however, with advantages for PET/CT by trend. In the subgroup with histopathologic confirmation of T and N stages, the situation was similar (T staging, P = 0.705; N staging, P = 0.334). Conclusion: This study indicates that PET/MR using a fast MR protocol does not improve the diagnostic accuracy of the staging of non–small cell lung cancer.
Since 2003, PET/CT using 18F-FDG as tracer has emerged as the most important cross-sectional imaging modality for whole-body staging of patients with non–small cell lung cancer (NSCLC) (1). Today, 18F-FDG PET/CT assumes a prominent role in the presurgical evaluation for metastatic disease and is considered by various international guidelines (2,3). Unlike the whole-body approach of PET/CT, MR imaging in lung cancer staging today is reserved to selected regionalized indications, for which PET/CT provides limited information, because of the inferior soft-tissue contrast of CT or the high physiologic background activity of PET. Such specific questions include the presence of mediastinal infiltration by a lung tumor and the presence of metastatic disease to the brain and liver. In 2011, the first clinical PET/MR scanner was installed (4). PET/MR imaging might be superior to PET/CT in the detection of mediastinal invasion and extrathoracic malignancy, but it is yet unknown if the shortcomings of MR in lung imaging, such as visibility of small nodules, can be compensated for by the addition of PET. Several groups have suggested whole-body PET/MR protocols for lung cancer patients, all of which contain at least 1 pulse sequence specifically tailored to the chest, and most of them with exceptionally long MR acquisition times (5–9). Ohno et al. showed that coregistered PET and whole-body MR is superior to PET/CT for the staging of lung cancer patients, partly contradicting previous results for whole-body MR only (8,10–12). Fraioli et al. demonstrated that PET/MR is accurate in the assessment of NSCLC resectability, detecting the correct T stage and N stage in 74% of patients (6). Another study by Heusch et al. showed that PET/MR and PET/CT was 100% accurate in the T staging in a small cohort of 16 NSCLC patients, clearly exceeding previous results of larger studies with PET/CT (9). An assessment of the M stage was not part of this study.
Because relevant comparative information is missing, we prospectively compared the accuracy of PET/CT with that of time-matched PET/MR in the pretherapeutic TNM staging of NSCLC.
MATERIALS AND METHODS
This study was approved by the institutional review board. All patients provided signed informed consent before the examinations.
Fifty-two consecutive patients (36 men, 16 women; median age, 65 y) with biopsy-proven or suspected NSCLC were enrolled between May 2012 and November 2014 at the University Hospital of Zurich. Thereof, 8 subjects have been reported previously in another study with different goals (tumor delineation and image artifacts) (5). All subjects in this study underwent conventional staging, including a review of their medical history, physical examination, blood tests, bronchoscopy, biopsy of the primary tumor, and a contrast-enhanced CT of the chest and upper abdomen. All subjects also underwent imaging with a trimodality PET/CT/MR system. Ten patients were excluded from the study because final histopathology revealed lesions other than NSCLC (small cell lung cancer [4 subjects]; inflammatory lesions [3 subjects]; carcinoid, lymphoma, and hamartoma [1 subject each]). Finally, 42 subjects (29 men, 13 women; median age, 65 y; range, 35–89 y) remained.
Imaging Techniques
The trimodality PET/CT/MR system consists of a full-ring time-of-flight 64-slice PET/CT scanner (Discovery PET/CT 690 VCT; GE Healthcare) and a 3-T MR scanner (Discovery MR 750w; GE Healthcare), connected by a shuttle system (5,13,14). Patients fasted at least 4 h before being injected with 350 MBq of 18F-FDG. The total uptake time was 60 min. After 40 min, patients were transferred into the MR machine. All MR images were acquired during these 20 min. Then patients were transferred to the PET/CT machine, where acquisition started subsequently. Details are given in the supplemental materials (available at http://jnm.snmjournals.org).
PET/CT
PET and unenhanced CT datasets were acquired from vertex to mid thighs. PET data were acquired during shallow breathing. CT data were acquired during breathing baseline for PET attenuation correction and diagnostic purposes. Detailed scan parameters are given in Supplemental Table 1 and were published previously (5).
MR
The MR protocol consisted of 3 pulse sequences: an axial whole-body T1-weighted 3-dimensional dual-echo fast spoiled gradient-echo sequence (liver-accelerated volume acquisition [LAVA]-Flex; GE Healthcare), a coronal whole-body short TI inversion recovery sequence without breath-hold, and a T2-weighted sequence with motion correction (periodically rotated overlapping parallel lines with enhanced reconstruction [Propeller]; GE Healthcare) covering the lung, acquired axially during free breathing, using respiratory triggering (15). The total MR acquisition took approximately 16 min. The rationale for this rather short MR protocol was to keep the MR acquisition time equal to the PET acquisition time, so that this protocol could be implemented into a fully integrated PET/MR without impact on the total acquisition time compared with PET/CT.
Technical details are given in Supplemental Table 2 and were published previously (5).
Surgery and Nonsurgical Therapy
Subsequent thoracic surgery with curative intent was performed in 20 subjects and included mediastinal lymphadenectomy. Details are given in the supplemental materials.
Image Analysis
Anonymized image datasets were assessed in random order by 2 independent review boards of dually trained radiologists/nuclear medicine physicians with 7–12 y of experience in both MR and PET/CT interpretation. Interpreters were masked to all patient data other than the suspicion of NSCLC. Each board consisted of 2 interpreters. Review board A first analyzed PET-only datasets in random order and without access to CT images, then PET/CT datasets in random order. Review board B analyzed first PET-only datasets without access to MR images, then PET/MR datasets. The PET-only analysis was done because it presents the least common denominator of both boards and thus allows for a comparison of their agreement. After each single PET, PET/CT, and PET/MR analysis, a TNM stage (seventh edition) was assigned based on intraboard consensus decision (16). If 2 stages (T, N, or M) could not be clearly differentiated, both stages were noted and deemed equivocal.
Standard of Reference
Histopathology of the primary tumor was available in all subjects. Surgical specimens served as the standard of reference for the T stage and N stage in 20 subjects. Two patients who were deemed no-surgery candidates underwent biopsy of mediastinal and hilar lymph nodes guided by endobronchial ultrasound. Here, histopathology of biopsy specimens served as the standard of reference for the N stage. The T stage and N stage of the remaining 22 and 20 subjects, respectively, was confirmed by at least 1 different imaging method (contrast-enhanced CT, 22 subjects; contrast-enhanced MR, 5 subjects). Five patients underwent histopathologic confirmation of distant metastasis, 4 by surgery and 1 by biopsy. All other lesions were confirmed by at least 1 different cross-sectional imaging modality and follow-up, including imaging until death or for a mean period of 568 d. Interpreters who defined the TNM stage if histopathology was unavailable were not members of the aforementioned review boards.
Statistical Analysis
On the basis of the standard of reference, scores ranging from 0 to 2 were assigned to the findings of the review board readings. A score of 2 indicates a correct assignment of a T, N, or M stage. A score of 1 also indicates a correct assignment, but because of equivocal findings, 2 stages had been noted by the board. And a score of 0 indicates an incorrect finding, no matter if findings were deemed equivocal or not. We counted subjects with a score of 0 and subdivided them into overestimated and underestimated individuals.
The interobserver agreement between both review boards concerning the designation of T, N, and M stages with PET-only datasets was assessed using κ statistics. Agreement was defined as moderate (0.41–0.60), substantial (0.61–0.80), or almost perfect (>0.80) (17). Differences between the T, N, and M stages assigned with either PET/CT (board A) or PET/MR (board B) were compared using a Wilcoxon signed-ranks test for matched pairs.
On the basis of the TNM stages assigned by PET/CT (board A) and PET/MR (board B), the potential resectability of the NSCLC was defined. Potential resectability was characterized as the prevalence of 3 conditions: a T stage of less than 4, an N stage of less than 3, and an M stage of 0 (18). A score of 1 was assigned if resectability was given, a score of 0 if resectability was not given. If an equivocal finding turned the scale, then a score of 0.5 was assigned. According to the standard of reference, the area under the receiver-operating-characteristic curve, fitted for sensitivity and specificity, and the 95% confidence intervals were calculated.
A P value of less than 0.05 was deemed statistically significant. All statistical analyses used SPSS Statistics 19.0.1 (IBM).
RESULTS
Histopathologic results of study subjects and TNM staging according to the standard of reference are given in the supplemental materials.
Interobserver Agreement
For the assessment of the variability of staging between the 2 review boards, we calculated the κ of their PET ratings. The κ was 0.49 for the T stage, 0.60 for the N stage, and 0.53 for the M stage. There was no significant difference in the accuracy of their PET findings (P = 0.380 for T stage, P = 0.862 for N stage, and P = 0.351 for M stage).
Diagnostic Accuracy
Compared with PET/CT, PET/MR provided 7 items of additional information in 5 of 42 patients (9%). On the other hand, PET/CT provided 18 items of additional information in 15 of 42 patients (36%).
These items represented the exact location of nodal metastases in 6 patients by PET/CT, whereas PET/MR made a contribution over PET/CT only in 1 subject. PET/CT correctly estimated tumor size (3 subjects), detected main bronchus involvement (2 subjects) (Supplemental Fig. 1), and correctly discriminated pleural dissemination from ipsilateral intrapulmonary nodules (1 subject). PET/MR correctly estimated tumor size in 1 subject for whom PET/CT was incorrect and detected the absence of chest wall infiltration in another subject. Compared with PET/MR, distant metastases were exactly located by PET/CT in 6 subjects, whereas PET/MR correctly located them in 4 subjects. However, no statistically significant improvement of the staging was found, neither for the whole cohort nor for the subgroup with histopathology as reference standard for T staging and N staging (Table 1). The diagnostic accuracy for the TNM staging by PET/MR and PET/CT is given in Table 2.
Comparison of Diagnostic Accuracy of PET/MR and PET/CT
Diagnostic Accuracy of Imaging Methods
T Staging
Of the 34 subjects correctly classified by PET/CT, 29 were also classified correctly by PET/MR, whereas 3 were rated as correct but equivocal and 2 were classified incorrectly. The lower performance of PET/MR was due to missed main bronchus involvement (2 subjects), misjudgment about size (2 subjects), and misinterpretation of pleural dissemination as lung metastases. Additional information is provided in the supplemental materials.
Overall, PET/MR underestimated 3 subjects (7%) and overestimated 2 subjects (5%), whereas PET/CT underestimated 3 subjects (7%) and overestimated 1 subject (2%).
N Staging
Of the 37 subjects with a correct nodal stage by means of PET/CT, 32 were classified correctly by PET/MR, whereas 1 subject was rated as correct but equivocal, and in 4 the results were classified as incorrect. The single subject who was classified as correct but equivocal by PET/CT was classified incorrectly by PET/MR. Of the 4 subjects whose results were classified as incorrect by PET/CT, 3 were also classified as incorrect by PET/MR, whereas 1 was classified correctly. Additional information is provided in the supplemental materials.
Altogether, PET/MR underestimated the nodal stage in 5 subjects (12%), whereas PET/CT underestimated only 1 subject (2%). Overestimation was done by both modalities in 3 subjects (7%), 2 of which were identical.
M Staging
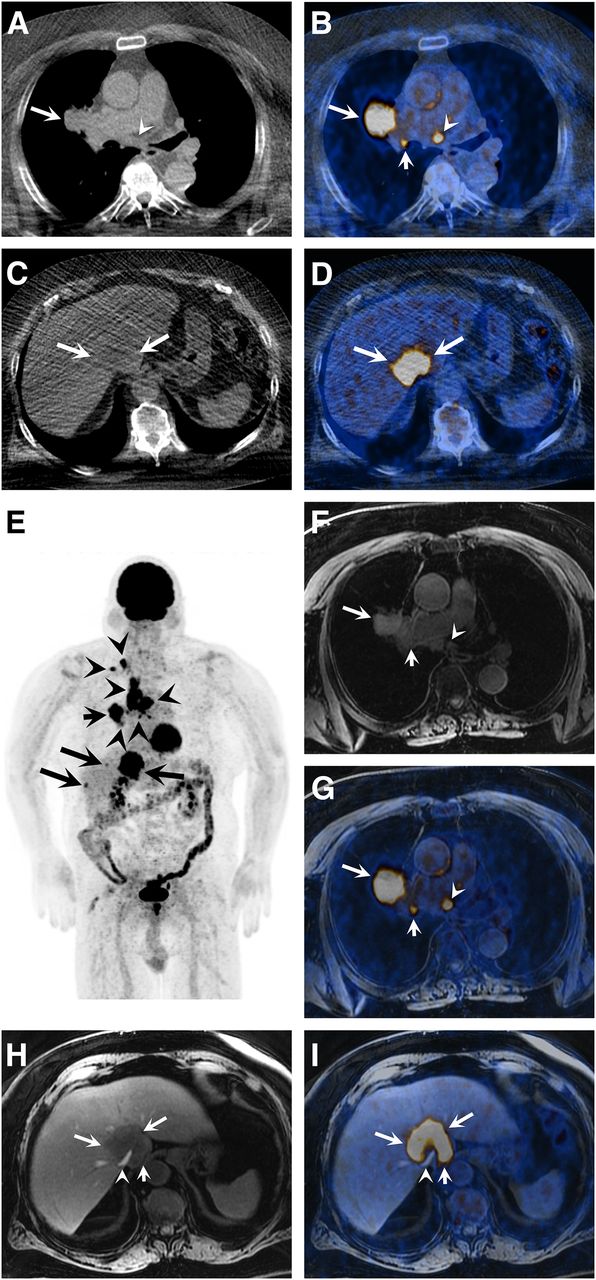
In 12 of 42 subjects (29%), distant metastases were present, corresponding to an M1a stage in 2 subjects and an M1b stage in 10 (Fig. 1). Of the 11 subjects with distant metastases identified correctly by PET/CT, PET/MR correctly rated 9 subjects, whereas 1 subjected was classified as correct but equivocal and 1 as incorrect. The single subject who was classified as correct but equivocal by PET/CT was classified correctly by PET/MR. Additional information is provided in the supplemental materials.

A 64-y-old man with lung cancer in right upper lobe, stage T2a N3 M1b. Axial CT image (A) shows mass (arrow) in right upper lobe close to hilum. Prominent subcarinal lymph node (arrowhead) is seen. Axial coregistered PET/CT image (B) confirms highly 18F-FDG–avid tumor (arrow) and presence of subcarinal nodal metastases (arrowhead) and right hilar metastases (short arrow). Axial CT image (C) at level of gastroesophageal junction shows slightly hypodense liver lesion (arrows) in region of intrahepatic segment of inferior vena cava, being hardly appreciated. Axial coregistered PET/CT image (D) reveals intense 18F-FDG uptake of lesion (arrows), compatible with metastasis. Coronal PET maximum-intensity-projection image (E) confirms nodal metastases in right hilum, mediastinum, and right supraclavicular region (arrowheads) as well as multiple liver metastases. Primary tumor (short arrow) is seen as well. Axial LAVA (water-only) image (repetition time, 4.3 ms; echo time, 1.3 ms; flip angle, 12°) (F) and coregistered PET/LAVA image (G) show primary tumor (arrow) in right upper lobe, nodal metastases in right hilum (short arrow), and subcarinal region (arrowhead). Axial LAVA (water-only) image (repetition time, 4.3 ms; echo time, 1.3 ms; flip angle, 12°) (H) and coregistered PET/LAVA image (I) show liver metastasis (arrows) with more anatomic detail. Intrahepatic segment of inferior vena cava (arrowhead) is compressed but not infiltrated. Fat plane between liver and right crus of diaphragm (short arrow) is preserved.
Overall, PET/MR missed a sclerotic bone metastasis in 1 patient (2%) and overrated 4 patients (10%) with regard to distant metastatic disease. PET/CT did not miss distant metastatic spread and overrated 2 patients (7%) only.
Potential Resectability
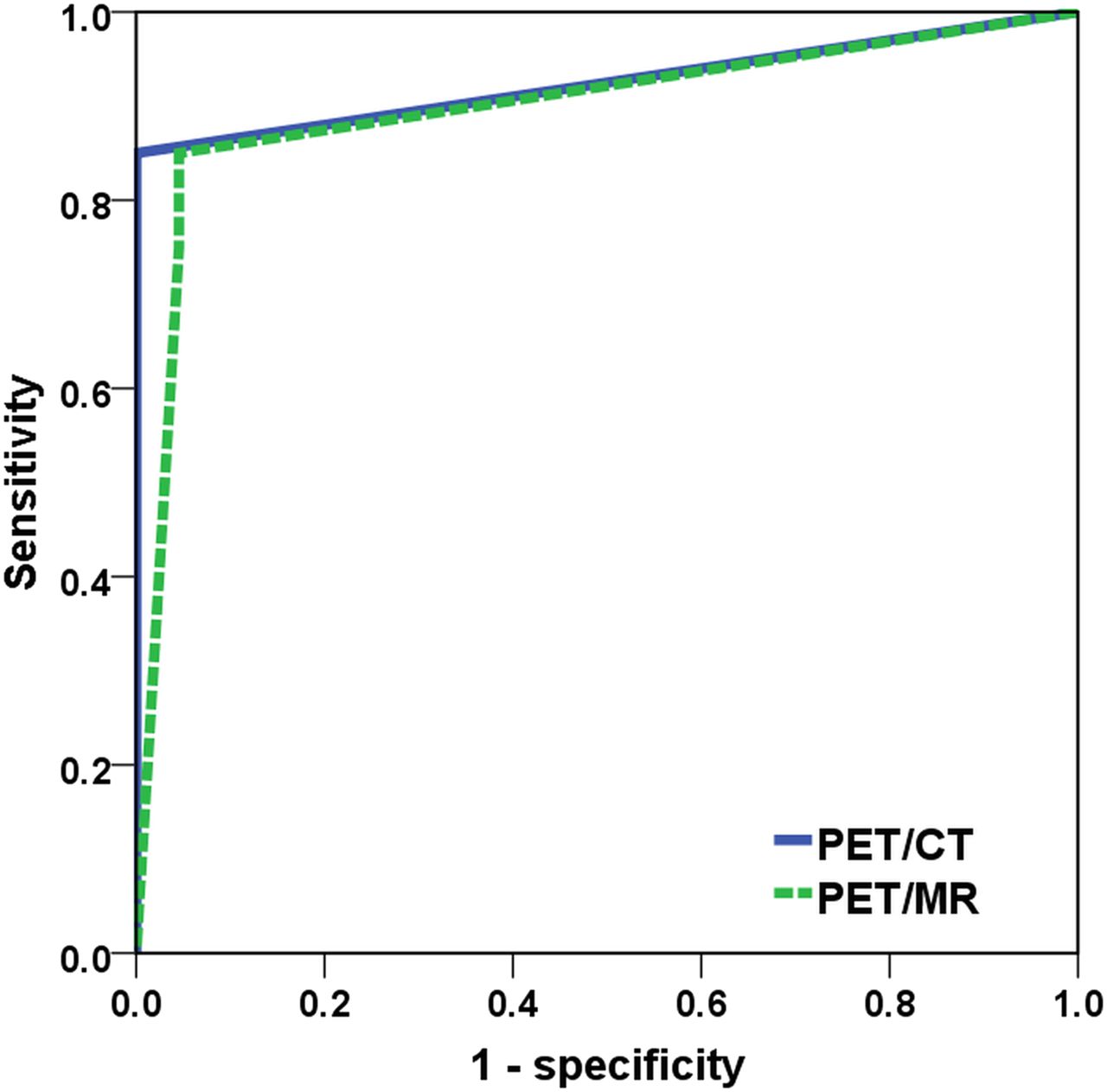
For the assessment of potential tumor resectability, the area under the receiver-operating-characteristic curve was calculated for PET/CT and PET/MR (Fig. 2). The receiver-operating-characteristic analysis revealed no difference between PET/CT and PET/MR.
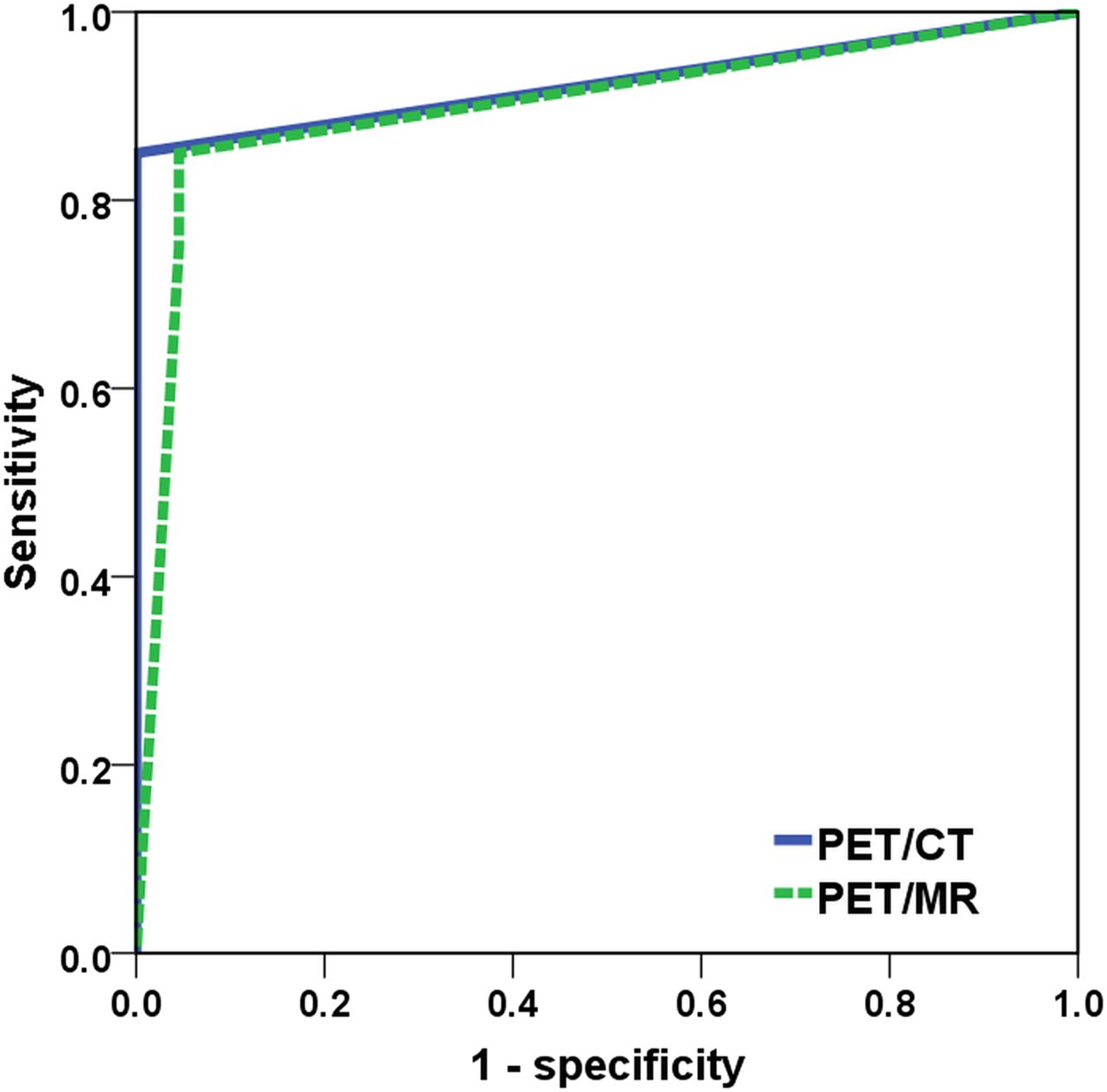
Graph illustrates receiver-operating-characteristic curves for potential resectability of tumors with PET/MR and PET/CT. Potential resectability of tumor was defined as T stage below 4, N stage below 3, and M stage of 0 (PET/MR: area under the curve, 0.90; 95% confidence interval, 0.79–1.00 [P = 0.000]; PET/CT: area under the curve, 0.93; 95% confidence interval, 0.83–1.00 [P = 0.000]).
DISCUSSION
This prospective study in NSCLC patients compared the staging capabilities of whole-body unenhanced PET/MR and PET/CT using similar acquisition times. We found that both modalities were equally accurate in the TNM staging, however, with some advantages for PET/CT. There appears to be a tendency toward more misclassification of local nodal and distant metastatic disease with PET/MR compared with PET/CT.
In addition to the unquestionable benefit of lower radiation exposure, mostly irrelevant in NSCLC patients, PET/MR is expected to be more accurate than PET/CT in the evaluation of mediastinal and chest wall infiltration by a lung tumor (6). PET/MR can also be conjectured to be better in detecting metastases in organs with a high physiologic 18F-FDG background activity, such as the brain and the liver, in which small metastatic lesions might go undetected with PET/CT.
Several groups have suggested whole-body PET/MR protocols for lung cancer patients, all of those containing at least 1 pulse sequence specifically tailored to the chest (5–9). However, most of these protocols are time-consuming, taking between 40 and 90 min for MR acquisition, far exceeding the acquisition time of PET and PET/CT.
In clinical practice, such lengthy examinations are problematic with regards to patient compliance and throughput. PET/MR examination times matching those of PET/CT are desired to consider PET/MR a valuable alternative to PET/CT (5,9).
Resectability and T Staging
Above all, the T stage of a tumor determinates its resectability (19,20). The ability to differentiate between stages T3 and T4 is critical for any cross-sectional imaging modality, because T4 tumors are widely considered not resectable. The detection of infiltrative growth into the mediastinum and chest wall is facilitated by T2-weighted images without fat suppression and T1-weighted contrast-enhanced sequences (19). MR is particularly helpful for assessing tumor growth into pulmonary veins and infiltration of the superior and inferior vena cava (19). Although MR to date is mainly used in cases of unclear findings of mediastinal and chest wall infiltration with CT or PET/CT, hybrid PET/MR needs to provide morphologic images of the lung parenchyma itself to address other T stage–defining factors, such as pulmonary nodules (5,21).
Fraioli et al. specifically addressed the resectability of primary tumors with PET/MR (6). They reported a high accuracy of PET/MR: although they made no direct comparison with PET/CT, they found a valid agreement between both modalities. In a small cohort of 16 patients, Heusch et al. reported correct T staging by both PET/CT and PET/MR in all subjects (9). They also found an excellent agreement of the SUV and size of tumors with both modalities. In our study, there was also no significant difference in the accuracy of T staging with either method, despite a trend toward more correct and less equivocal results with PET/CT. This was mainly due to misinterpretation of tumor size and missed main bronchus involvement by PET/MR.
N Staging
The sensitivity and specificity of PET/CT for the identification of mediastinal metastases was approximately 77% and 86%, respectively (2). Despite suggestions of using short TI inversion recovery or T2-weighted black-blood imaging for the assessment of small mediastinal nodes, MR has not gained widespread clinical acceptance for N staging of lung cancer (10,12,20,22). For PET/MR, Fraioli et al. reported good accordance of PET/MR and PET/CT but did not provide data on the accuracy of PET/MR in comparison with PET/CT (6). Heusch et al. found that PET/MR and PET/CT performed comparably in the N staging of 22 patients (9). Their study used histopathology as a reference standard; however, distant metastases were not addressed.
In most comparative studies, the lesion-to-background uptake varies between PET/MR and PET/CT because examinations are performed sequentially on 2 different machines. This may particularly alter the visual perception of nodal disease (23), which is not an issue with the trimodality system used in our study. With 79% of patients staged correctly by PET/MR, our results correspond to those of Fraioli et al. and Heusch et al., although we used a more comprehensive MR approach (6,9). Like them, we found no significant difference in the N staging with both methods, despite a trend of more correct staging with PET/CT. Using contrast enhancement might turn the tide in favor of PET/MR but would have to be compared with contrast-enhanced PET/CT.
M Staging
PET/CT misses lesions that are small or located in organs with high background 18F-FDG activity, such as the brain and liver, or might be falsely positive in the adrenal glands, which display variable physiologic 18F-FDG uptake (24–26). Hence, regionalized MR is recommended depending on the patient’s symptoms and stage of disease (2,3,18,27,28). Even without specific organ protocols, PET/MR supposedly has a higher yield of distant metastases in asymptomatic patients than PET/CT, not only because of better anatomic detail but also because of tissue decomposition properties of Dixon-type pulse sequences that are a prerequisite for MR-based attenuation correction in the body (10).
Beiderwellen et al. found an equal performance of PET/MR and PET/CT in 48 bone lesions in oncologic patients (29). In NSCLC patients, PET/MR detected slightly more bone and liver metastases than PET/CT, albeit without statistical significance (6). Our study also found no difference between both modalities, with accuracies comparable to the results of Fraioli et al. (6). All liver and adrenal gland metastases in our cohort were detected by both modalities, whereas none of our patients had brain metastases. Complementing a whole-body PET/MR in NSCLC with a contrast-enhanced short brain MR protocol of less than 15 min after the PET/MR should be able to deal with the issue of brain metastases readily. Therefore, development of rule-out protocols also encompassing the brain with MR in PET/MR may lead to a NSCLC 1-stop-shop examination without need of supplementation by an additional brain MR in many patients, as currently is the case in PET/CT. Additional discussion is provided in the supplemental materials.
A first limitation of our study is that—for ethical reasons—the primary tumor and local lymph nodes were not resected in all patients. However, histopathology was available in all primary tumors, and results of the subgroup with surgical confirmation of T stage and N stage were not different from the whole cohort. Second, our study was performed without contrast agents, so our results should be interpreted with caution when comparing them with studies using contrast-enhanced examinations. Nonetheless, contrast agents are not consistently used in PET/CT. Third, because our goal was to provide a time-effective PET/MR protocol, we refrained from using specific pulse sequences for selected organs. Further studies are needed to address the potential benefits of MR pulse sequences tailored to the liver and brain within a PET/MR protocol. Fourth, with CT-based attenuation correction available using the trimodality approach, we did not use an MR-based attenuation correction for PET/MR. However, this drawback affects mostly therapy monitoring, for which comparing accurate SUVs is desired.
CONCLUSION
Our results indicate that PET/MR and PET/CT have similar diagnostic accuracy for the staging of NSCLC. We found a tendency toward more misinterpretation of nodal metastases and distant metastases disease with PET/MR compared with PET/CT. Without the addition of dedicated brain and possibly liver MR pulse sequences as part of a PET/MR protocol, PET/CT will likely remain the preferred hybrid imaging modality for the staging of patients with NSCLC.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study received financial support by an institutional grant from GE Healthcare. Only non-GE employees had control of inclusion of data and information that might present a conflict of interest for those authors who are employees of GE Healthcare. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 15, 2015.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 9, 2015.
- Accepted for publication October 6, 2015.





{kind=link}
{kind=link}