


Abstract
Cerenkov luminescence imaging (CLI) can provide high-resolution images of 18F-FDG–avid tumors but requires prolonged acquisition times because of low photon sensitivity. In this study, we proposed a new modality, termed β-radioluminescence imaging (β-RLI), which incorporates a scintillator with a γ-rejection strategy for imaging β particles. We performed a comparative evaluation of β-RLI with CLI in both in vitro and in vivo systems. Methods: Using in vitro phantoms, we characterized the photon sensitivity and resolution of CLI and β-RLI. We also conducted a series of in vivo experiments with xenograft mouse models using both amelanotic (A375, UMSCC1-Luc) and melanotic (B16F10-Luc) cell lines. The B16F10 and UMSCC1 cell lines were transfected with the luciferase gene (Luc). CLI was acquired over 300 s, and β-RLI was acquired using two 10-s acquisitions. We correlated 18F-FDG activities, as assessed by PET, with tumor radiances for both β-RLI and CLI. We also compared tumor signal-to-background ratios (SBRs) between these modalities for amelanotic and melanotic tumors. Results: For in vitro experiments, the photon sensitivity for β-RLI was 560-fold greater than that for CLI. However, the spatial resolution for β-RLI (4.4 mm) was inferior to that of CLI (1.0 mm). For in vivo experiments, correlations between 18F-FDG activity and tumor radiance were 0.52 (P < 0.01) for β-RLI, 0.81 (P = 0.01) for amelanotic lesions with CLI, and −0.08 (negative contrast; P = 0.80) for melanotic lesions with CLI. Nine of 13 melanotic lesions had an SBR less than 1 for CLI, despite an SBR greater than 1 among all lesions for β-RLI. Conclusion: β-RLI can produce functional images of both amelanotic and melanotic tumors in a shorter time frame than CLI. Further engineering developments are needed to realize the full clinical potential of this modality.
Cerenkov luminescence imaging (CLI) is an optical radionuclide imaging technique that can produce high-resolution (1–2 mm) functional images of 18F (1–3). Because CLI signals demonstrate a strong linear relationship with PET activity (3), this technology can be used for measuring tumor burden after chemotherapy administration (4,5) and surgical resection (6,7). Many radiotracers including 18F-FDG are already approved by the Federal Drug Administration. As a result, CLI has immediate translational potential, and studies have already been reported in human patients (8–10).
However, CLI is limited by its relatively low photon sensitivity. Investigators have estimated that a 0.635-MeV positron from 18F can produce only 20 photons with wavelengths between 250 and 600 nm (1). As a result, prolonged acquisition times on the order of 3–5 min in a darkened environment are required (3,7,9). These stringent acquisition conditions may be difficult to satisfy in certain clinical settings, including the operating room.
One potential strategy for improving photon sensitivity is to use a scintillator, which can convert β particles and γ rays from 18F into optical light. Scintillators can produce between 1,000 and more than 100,000 photons per MeV, depending on the material used (11). Scintillators have been incorporated into handheld radioactive probes and cameras for radio-guided surgical applications (12–16).
In recent years, non-Cerenkov optical radionuclide imaging techniques, termed radioluminescence imaging (RLI), have been evaluated (17). In particular, investigators have performed in vitro and in vivo imaging of the pure γ emitter 99mTc by placing bismuth germanate oxide scintillator crystals between the radioactive source and the camera within a commercial small-animal imaging system. The system resolution was 1.3 mm, and a collimator was present (18). Non–scintillator-based RLI experiments for 99mTc (19) and an α emitter (20) have also been reported. In our group, 1 investigator performed RLI of 18F-FDG-uptake in single cells by imaging a radioactive cell monolayer in direct contact with a scintillator using microscopy (21). Another investigator designed a fiber-optic system for imaging 18F-FDG from ex vivo atherosclerotic plaques that were covered by a scintillator (22).
In this study, we proposed a new method for imaging β particles from 18F using a scintillator. This method, termed β-radioluminescence imaging (β-RLI), incorporates RLI with a γ-rejection strategy adapted from β probes (12). We hypothesized that β-RLI may provide enhanced photon sensitivity, compared with CLI. Furthermore, β-RLI may produce images of intact 18F-FDG–avid tumors in a shorter time frame than that required with CLI. The purpose of this study was to perform a comparative evaluation of β-RLI with CLI in both in vitro and in vivo settings.
MATERIALS AND METHODS
Materials
18F-FDG was produced from the radiochemistry facility (Stanford, CA). Two melanoma cell lines, melanotic B16F10 and amelanotic A375, were obtained from the American Type Culture Collection. The head and neck UMSCC1 cell line was obtained from the University of Michigan. The B16F10 and UMSCC1 cell lines were transfected with the pGL4.10[luc2] vector from Promega, using the jetPRIME transfection reagent (Polyplus) to create B16F10-Luc and UMSCC1-Luc cell lines.
Optimal Imaging Modalities
All images were acquired using an IVIS system (200 or Spectrum) with medium binning and a 10- to 13-cm imaging field of view. Essential acquisition parameters for all imaging modalities are listed in Table 1. A schematic for β-RLI is shown in Figure 1.
Components Required for Acquiring CLI, RLI, and Block-RLI

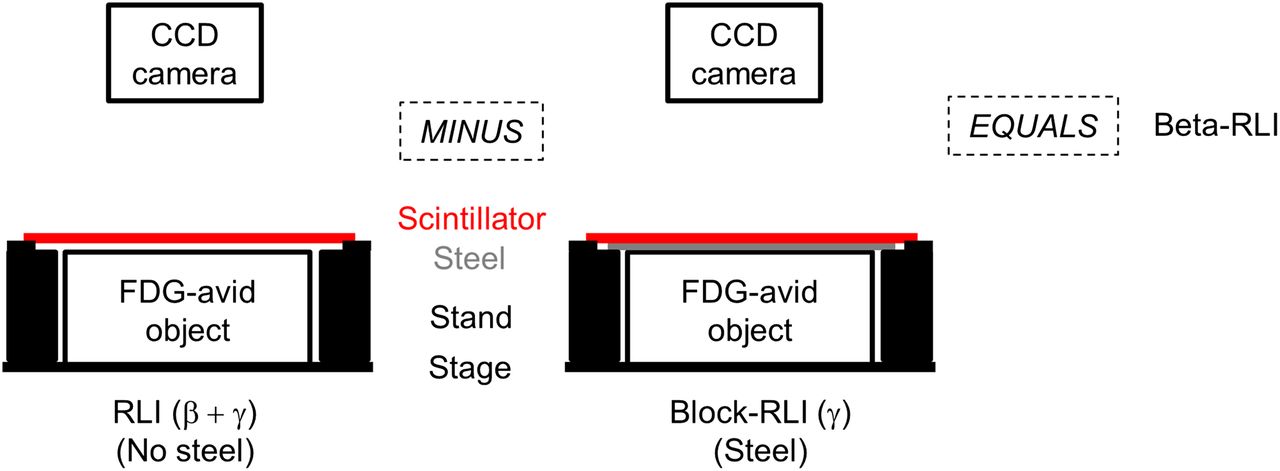
β-RLI acquisition schematic. β-RLI was acquired by obtaining difference between RLI (containing both β particles and γ rays ) and block-RLI (containing mostly γ rays). Schematic is not drawn to scale. Scintillator thickness and stainless steel thickness were less than 1 and 1 mm, respectively. CCD = charge-coupled device; RLI = radioluminescence image.
Optical imaging modalities are described as follows. For CLI, no material was placed between the camera and the object of interest. For RLI, a scintillator was positioned approximately 1 mm above the object but below the camera. Optical signals from both β particles and γ rays were collected. Eq. 1For block-RLI, a 1-mm-thick stainless steel slab (Evansville Sheet Metal Works) was placed between the scintillator and the object. Stainless steel was used because of its ability to block almost all β particles with energies less than 1.5 MeV (12). The optical signal captured by the camera can be expressed as:
Eq. 1For block-RLI, a 1-mm-thick stainless steel slab (Evansville Sheet Metal Works) was placed between the scintillator and the object. Stainless steel was used because of its ability to block almost all β particles with energies less than 1.5 MeV (12). The optical signal captured by the camera can be expressed as: Eq. 2where α1 and α2 are the percentage β and γ transmissions through stainless steel. For this study, estimates of α1 and α2 were 0.03 and 0.91, respectively (supplemental data; supplemental materials are available at http://jnm.snmjournals.org). For β-RLI (with γ rejection), this image was calculated as the difference between the RLI and block-RLI, which was multiplied by 1/α2 to eliminate the γ component.
Eq. 2where α1 and α2 are the percentage β and γ transmissions through stainless steel. For this study, estimates of α1 and α2 were 0.03 and 0.91, respectively (supplemental data; supplemental materials are available at http://jnm.snmjournals.org). For β-RLI (with γ rejection), this image was calculated as the difference between the RLI and block-RLI, which was multiplied by 1/α2 to eliminate the γ component. Eq. 3All RLI and block-RLI were acquired using a radioisotopic screen (Bruker Biosciences Corp.), although other scintillators were also evaluated (supplemental data).
Eq. 3All RLI and block-RLI were acquired using a radioisotopic screen (Bruker Biosciences Corp.), although other scintillators were also evaluated (supplemental data).
Optical Image Processing
Median filtration (3-pixel width) was applied to CLI, RLI, and block-RLI. RLI and block-RLI also underwent additional gaussian smoothing (σ = 2 mm) to reduce noise. Bias correction, flattening field correction, and cosmic ray correction (median filtration of pixel values more than 10 SDs from the image mean) were also applied. All processing was performed using software written in Python 3.2.3 (Python Software Foundation).
In Vitro
Signal Uniformity
The outer shell of the Micro Deluxe Phantom (Data Spectrum Corp.) was filled with 20 mL of 1% agarose (Sigma-Aldrich Chemical Co.) to create a uniform base. A 30-mL solution of 5.1 MBq (137.5 μCi) of 18F-FDG (254 kBq/mL or 6.9 μCi/mL) was prepared. RLI, block-RLI, β-RLI, and CLI were obtained. Profiles across images were extracted. An additional experiment evaluating signal uniformity over a nonuniform background was also conducted (supplemental data).
Resolution
A 0.5-mm internal diameter capillary tube (VitroCom) was filled with 18F-FDG (370 kBq/mL or 10 μCi/mL). β-RLI and CLI were acquired with the scintillator placed directly against the capillary tube. Small binning was used. Profiles were drawn perpendicular to the capillary tube, and full-width half maximum (FWHM) values were extracted.
Object–Scintillator Distance Dependencies for β-RLI
A 0.5-mm-diameter capillary tube was filled with 259 kBq/mL (7 μCi/mL) of 18F-FDG and positioned on a stack of ten 1-mm-thick acrylic slabs. Serial β-RLI was acquired at distances between the capillary tube and scintillator of 1–10 mm. FWHM values and maximum signal ratios (maximal signal at specified distance/maximal signal at 1-mm distance for air) from profiles drawn perpendicular to the capillary tube were acquired for these air distances. To evaluate depth dependency, maximum signal ratios were also acquired for a capillary tube placed under 1–3-mm of acrylic.
Photon Sensitivity Analysis
Serial 10-fold dilutions of 18F-FDG droplets (370 kBq [10 μCi] to 0.037 kBq [0.001 μCi]) dissolved in 50 μL of Matrigel (BD Biosciences) were prepared on microscope cover glasses (Fisher Scientific) in triplicate. Final concentrations ranged from 7.4 MBq/mL (200 μCi/mL) to 0.74 kBq/mL (0.02 μCi/mL). CLI and β-RLI were acquired. The average intensities of regions of interests (ROIs) over the droplets were plotted against 18F-FDG activities. The slopes of the linear regression curves represented the photon sensitivities for each modality. A similar analysis involving serial dilutions of 18F-FDG–avid B16F10 cells is described in the supplemental data.
In Vivo
Tumor Model
All animal studies were conducted in accordance with the institutional Administrative Panel on Laboratory Animal Care. B16F10-Luc, A375, and UMSCC1-Luc cells were cultured in Dulbecco modified Eagle medium supplemented with 10% fetal bovine serum and 1% penicillin-streptomycin (Invitrogen Life Technologies) at 37°C. Approximately 1.0E6 cells suspended in phosphate-buffered saline were inoculated into the right flank of female athymic nude mice (Charles River Laboratories) at 6–8 wk old. Mice were imaged after 9–10 d for B16F10-Luc and A375 cells and after 5–6 wk for UMSCC1-Luc cells.
PET Imaging
PET images were acquired using a microPET/CT scanner (Inveon; Siemens Medical Solutions USA, Inc.). Tumor-bearing animals were injected with 11.1–14.8 MBq (300–400 μCi) of 18F-FDG dissolved in 150 μL of phosphate-buffered saline via the tail vein. After 30–60 min, mice were anesthetized with 2% isoflurane (Aerrane’ Baxter), positioned prone, and imaged. PET images were reconstructed using the ordered-subsets expectation maximum algorithm with attenuation correction if CT data were available. Tumor activities were quantified using commercial software.
Optical Imaging
Acquisition times were 300 s for CLI and 10 s for both RLI and block-RLI. For CLI, 1–3 mice were imaged at the same time. For β-RLI, 1 mouse was imaged each time. BLI was acquired over 60 s at 10 min after intraperitoneal injection of D-Luciferin (150 mg/kg).
For the melanotic B16F10-Luc (n = 14) cell line, after tumor exposure (skin excision), β-RLI and CLI were acquired. Given negative tumor contrast with CLI, BLI was performed and mice were sacrificed. After confirming that photons from BLI did not pass through the scintillator (data not shown), β-RLI was performed after partial and full resections for 5 and 10 mice, respectively. After full resection, BLI was acquired for evaluating the presence of residual disease. CLI was not performed after partial and full resections because of the presence of D-Luciferin.
For the amelanotic A375 (n = 5) cell line, β-RLI and CLI were acquired after tumor exposure, partial resection, and full resection. Mice were not repositioned between β-RLI and CLI. Mice were sacrificed after initial imaging of the exposed tumors.
For the amelanotic UMSCC1-Luc (n = 13) cell line, after tumor exposure, β-RLI and CLI were acquired for 13 and 4 mice, respectively. Mice were then sacrificed.
Tumor Signal-to-Background Ratio (SBR)
Tumor ROIs were delineated with white light and functional (CLI, RLI, β-RLI, and BLI) images using ITK-SNAP 3.0 software (ITK-SNAP) (23). Background ROIs were drawn around the tumor ROI using a circular tool with a diameter of 4–6 mm. However, regions covering intact skin were excluded. Tumor SBRs were then computed.
Statistical Analysis
The following analyses were conducted: Pearson correlation coefficients between 18F-FDG PET activity (scaled to the time of optical imaging) and tumor radiance after tumor exposure were calculated for β-RLI, CLI for amelanotic tumors, and CLI for melanotic tumors.
Pearson correlation coefficients for SBRs from CLI versus β-RLI were calculated for amelanotic and melanotic tumors. A comparative analysis for SBR values from β-RLI versus RLI was also conducted (supplemental data).
One-sided t tests were conducted to determine whether tumor SBR declines between successive stages of serial resection were statistically significant. Tests were used for CLI and β-RLI of A375 tumors (n = 5) and for β-RLI of B16F10-Luc tumors (n = 5).
Among the grossly resected B16F10-Luc tumors with residual disease, as visualized with BLI, the median SBR and the percentage of cases with an SBR greater than 1.2 were tabulated.
RESULTS
In Vitro Experiments
Figure 2 shows RLI, block-RLI, β-RLI, and CLI of the cylinder with 18F-FDG. As exhibited in the profiles, the elevated background in RLI was suppressed in β-RLI. However, the resulting β-RLI was not nearly as uniform as CLI. In another experiment, β-RLI was effective in suppressing γ rays from a nonuniform background (supplemental data).

Signal uniformity across cylindric phantom filled with 5.1 MBq (137.5 μCi) of 18F-FDG. (A) Optical images (RLI, block-RLI, β-RLI, CLI). Intensity values for profile analysis were extracted from purple lines across phantom. (B) Intensity profiles.
As shown in Figure 3A, maximum signal ratios degraded as the air distance between the scintillator and the capillary tube increased. Furthermore, marked declines in maximum signal ratios were observed at 1- to 3-mm depths below the acrylic slabs. With respect to resolution, the FWHM values of profiles perpendicular to the 0.5-mm capillary source were 1.0 mm for CLI and 4.4 mm for β-RLI when the scintillator was placed against the capillary tube. Figure 3B shows that the β-RLI resolution decreased as the distance between the scintillator and the capillary tube increased. Figure 3C depicts intensity values for serial 18F-FDG dilutions. Photon sensitivity values for β-RLI and CLI were 391.8 p/s/cm2/sr/Bq (37.3 counts per second [cps]/kBq) and 0.7 p/s/cm2/sr/Bq (0.07 cps/kBq), respectively. β-RLI was 560 times more sensitive than CLI based on this experiment. β-RLI also exhibited greater photon sensitivity in imaging B16F10 cells (supplemental data).

Resolution and photon sensitivity analyses. (A) Effect of distance (air and acrylic) between 0.5-mm-diameter capillary tube and scintillator on maximal signal ratio (maximal signal at specified distance/maximal signal at 1-mm distance for air). (B) Effect of air distance on FWHM resolution. (C) Radiance values of β-RLI and CLI for serial 18F-FDG dilutions.
In Vivo Studies
Tumor Exposure
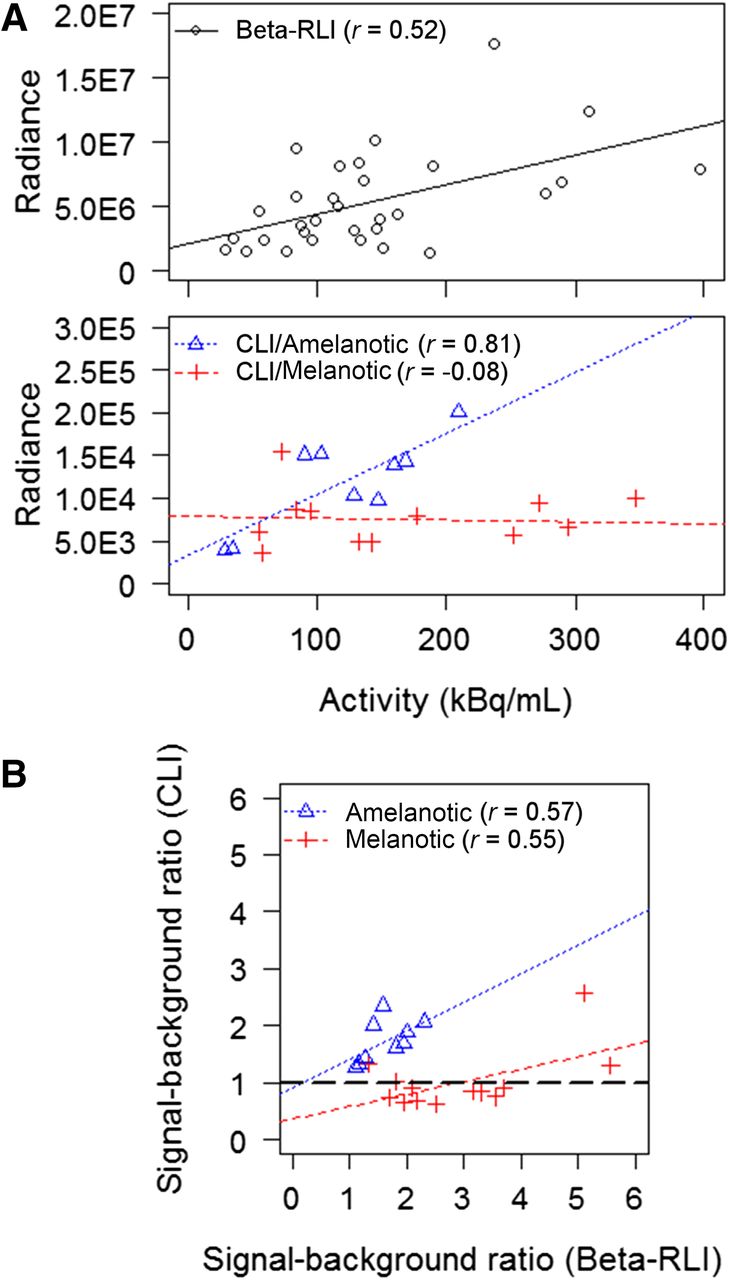
Figure 4A shows the relationship between preresection tumor radiance and 18F-FDG activity (kBq/mL) for β-RLI, CLI for amelanotic lesions, and CLI for melanotic lesions. The correlation coefficients between radiance and 18F-FDG activity were 0.52 (P < 0.01) for β-RLI, 0.81 (P = 0.01) for amelanotic lesions with CLI and −0.08 (P = 0.80) for melanotic lesions with CLI. Figure 4B shows the relationships between SBR values between CLI and β-RLI. Correlation coefficients were 0.57 (P = 0.11) for amelanotic lesions and 0.55 (P = 0.55) for melanotic lesions. For CLI, 9 of 13 melanotic lesions had an SBR less than 1, despite an SBR greater than 1 among all lesions for β-RLI. SBR values for RLI (without γ rejection) were significantly lower than those for β-RLI (supplemental data).
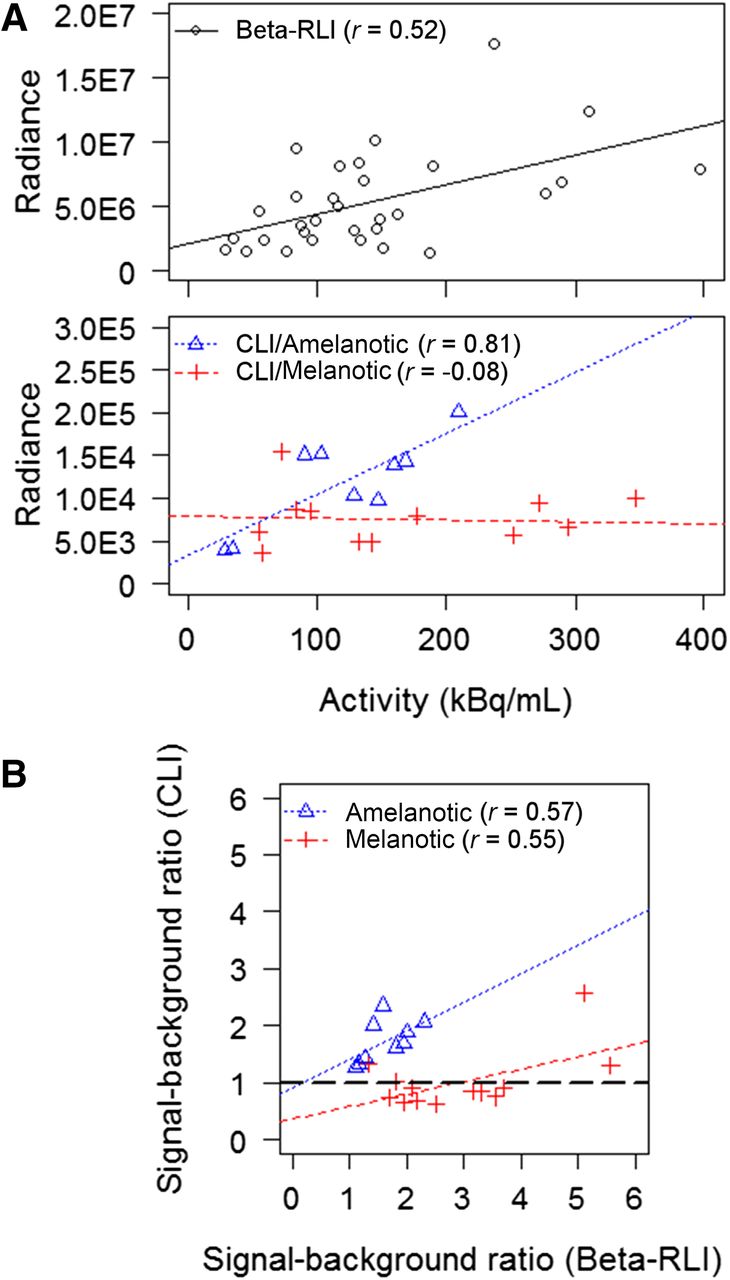
(A) Radiance vs. 18F-FDG activity (kBq/mL) for β-RLI among all tumors, CLI for amelanotic (A375 and UMSCC1-Luc) tumors, and CLI for melanotic (B16F10-Luc) tumors. Radiance has units (p/s/cm2/sr). (B) SBRs between CLI and β-RLI for amelanotic and melanotic tumors.
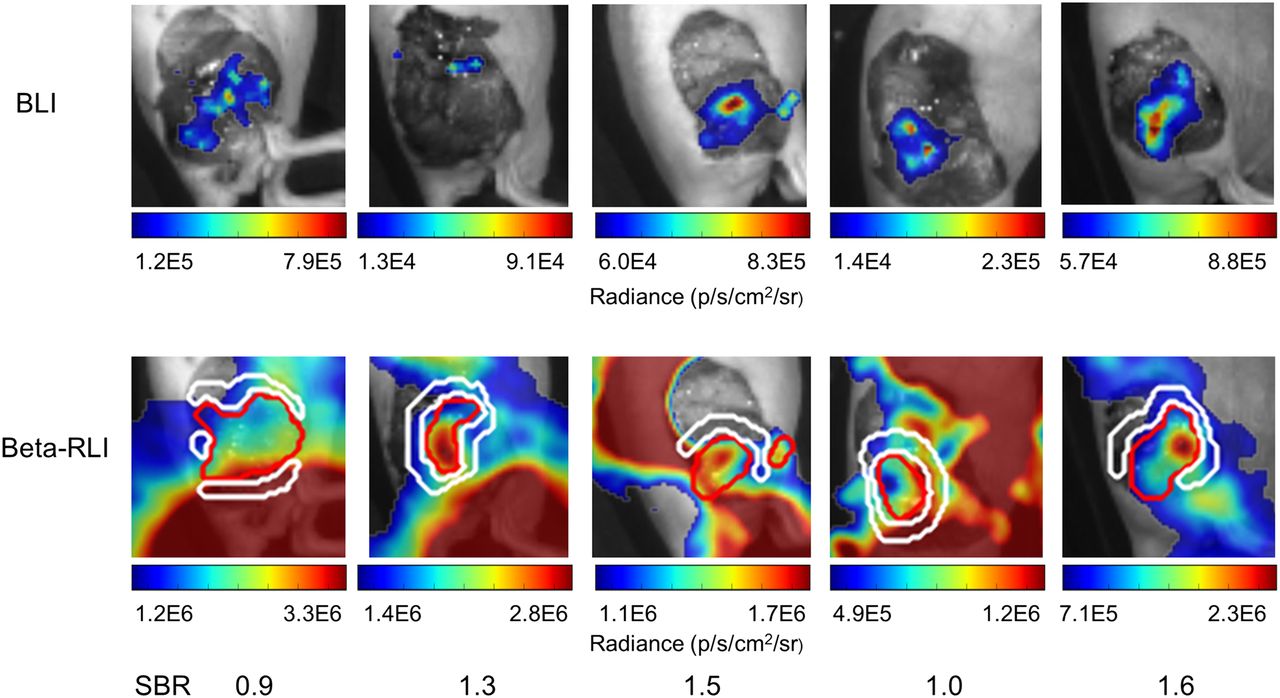
Figure 5 shows optical images of a mouse with a 71.0-kBq (1.92-μCi) B16F10-Luc tumor after tumor exposure. Although the tumor was clearly visible on β-RLI, there was negative contrast over the pigmented lesion on CLI. BLI confirms the presence of the tumor. On the other hand, the amelanotic A375 tumor (31.1 kBq [0.84 μCi]) was clearly visible on CLI, as shown in the left panel of Figure 6.

β-RLI, CLI, and BLI of a melanotic B16F10-Luc tumor with 71.0 kBq (1.92 μCi) of 18F-FDG by PET after tumor exposure. For β-RLI and CLI, red contours encircle the tumor. White contours encircle the background. SBRs are 3.6 for β-RLI and 0.7 for the CLI.

β-RLI and CLI of amelanotic A375 tumor with 31.1 kBq (0.84 μCi) of 18F-FDG by PET after serial resections. Serial resections included tumor exposure, partial resection, and full resection. For β-RLI and CLI, red contours encircle tumor. White contours encircle background. White arrows point to high signal from mouse knee, which may have been closer to scintillator than tumor bed.
Serial Resections
Figure 6 shows CLI and β-RLI of the A375 tumor after partial and full resections. The tumor signals were less apparent after partial resection and almost indiscernible after full resection for both modalities. On the β-RLI, the high background activity anterior to the tumor bed corresponds to the right knee. This structure may have been closer to the scintillator than the tumor bed, especially after serial restrictions of the initially exophytic tumor.
Table 2 shows SBRs of B16F10-Luc and A375 tumors after stages of serial resections for CLI and β-RLI. For CLI, partial and full resections of the A375 tumors demonstrated statistically significant decreases in SBR. However, for β-RLI, only full resections of the A375 and B16F10-Luc tumors demonstrated statistically significant SBR declines (P < 0.05 based on 1-sided t tests).
SBRs for Amelanotic A375 (n = 5) Tumors and Melanotic B16F10-Luc (n = 5) Tumors After Tumor Exposure, Partial Resection, and Full Resection
Residual Disease After Full Resection
All 10 mice that underwent full resections of B16F10-Luc tumors had residual disease based on BLI. The median SBR was 1.0 (minimum, 0.8; maximum, 1.6). Four of 10 tumors (40%) had an SBR greater than 1.2 and appeared discernible from background in Figure 7. The other 6 tumors were not easily discernible.
BLI and β-RLI after full tumor resections for 5 mice with B16F10-Luc tumors. For β-RLI, red contours encircle tumor. White contours encircle background. Each β image is scaled between minimum and maximum values within red contour to accentuate signal contrast within tumor bed. As such, background may appear saturated. High signal over tail region may be secondary to 18F-FDG accumulation from tail vein injection or urine. Image on very right corresponds to mouse in Figure 5.
DISCUSSION
In this study, we evaluated a method for the functional imaging of 18F called β-RLI. This method incorporates scintillator-based RLI with a γ-rejection strategy to preferentially image β particles. We then performed a comparative evaluation of β-RLI with CLI. Using in vitro experiments, we showed that β-RLI has 560-fold-greater photon sensitivity, which may allow for shorter acquisition times and less stringent requirements regarding ambient lighting intraoperatively. However, β-RLI also exhibited poorer spatial resolution (FWHM, 4.4 mm, vs. 1 mm for CLI), limited depth penetration secondary to the positron range of 18F (2.4 mm in water), and declines in both signal intensity and spatial resolution with increasing distance between the object and scintillator.
Using in vivo mouse models, we demonstrated statistically significant correlations between 18F-FDG activity and radiance for amelanotic lesions using β-RLI and CLI but not for melanotic lesions using CLI. Furthermore, 9 of 13 melanotic lesions had an SBR less than 1 for CLI, despite an SBR greater than 1 among all lesions for β-RLI. These results suggest that Cerenkov photons were absorbed by melanin. However, β-RLI often exhibited high background signal after resection, especially for surrounding structures closer to the scintillator (Fig. 6). Furthermore, CLI may provide a more quantitative assessment of tumor burden, as demonstrated by the statistically significant declines in SBR after both partial and full resections of the A375 tumors. Lastly, β-RLI is not suitable for imaging microscopic disease, as only 4 of 10 B16F10-Luc tumors with microscopic residual disease had an SBR greater than 1.2. Although CLI was not evaluated in this manner, its photon sensitivity is likely insufficient for evaluating microscopic disease (supplemental data).
The imaging properties for β-RLI are quite similar to those for β probes/cameras. With respect to photon sensitivity, a β prototype using a phoswich detector for electronic γ rejection exhibited lower photon sensitivity (2.5–14.0 cps/kBq depending on collimation) (14) than this β-RLI system (37.3 cps/kBq). However, β prototypes using the γ-subtraction technique that was adapted for β-RLI demonstrated a greater photon sensitivity (>100 cps/kBq) (12,13,16). β prototypes have a similar spatial resolution (1.6–5 mm) (13,15,16) and limited depth penetration (16). Furthermore, β probes also exhibit decreasing signal intensity and spatial resolution with increasing object–scintillator distance (14,15).
Over the past 2 decades, β probes have undergone intensive experimental and clinical evaluations for 18F-FDG–guided surgery. Experimental studies suggest that β probes offer real-time localization of tumor deposits superior to that of γ probes (24,25). In addition, clinical studies for the intraoperative tumor localization of melanomas (13) and other cancers (15,26) have yielded promising results.
Given the parallels between β-RLI and β probes/cameras, we would expect 18F-FDG–guided surgery to be the main clinical application for β-RLI. However, β-RLI has potential advantages over β probes/cameras. First, β-RLI has optical image overlay, which can allow the surgeon to correlate areas of increased activity with anatomic features. Second β-RLI can provide a large imaging field of view for efficient functional mapping of the operative bed.
There are other methods for improving the sensitivity of CLI without scintillators. Down-conversion involves using nanoparticles to shift the wavelength of Cerenkov light for better tissue penetration (27). However, most nanoparticles are exogenous agents that have not been approved by the Federal Drug Administration for human use. High-energy β-emitting radionuclides such as 90Y exhibit sensitivity superior to 18F. However, 90Y requires conjugation to peptides, such as arginine-glycine-aspartate, for tumor targeting (28).
Future research developments may revolve around scintillator design for improving the acquisition and image quality of RLI. First, a single-acquisition β-RLI technique could be realized by attaching a stainless steel grid onto a scintillating sheet. Because each image contains information from both RLI and block-RLI, interpolation algorithms could be used to recover the missing portions of these images before image subtraction for γ rejection, possibly allowing for decreased acquisition time and reduced image noise. Furthermore, γ rejection may be improved, because the scintillator and object often shift between RLI and block-RLI acquisitions. Second, spatial resolution may be improved through the incorporation of collimation (14) but at the expense of photon sensitivity. Third, flexible scintillators (29) may improve sensitivity by maximizing the contact between the tumor and scintillator and minimizing the effect of distance variations between the tumor and scintillator on signal intensities.
CONCLUSION
β-RLI can produce high-contrast functional images of both amelanotic and melanotic tumors in a shorter time frame than CLI. β-RLI limitations include poor spatial resolution, limited depth penetration, high background, and the need for acquiring 2 images. Further engineering developments are needed to realize the full clinical potential of this modality.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Funding for this work was provided by the RSNA research resident/fellow grant (RR1326), the Jacob Haimson endowed fellowship fund, the National Institutes of Health, the Stanford Department of Radiation Oncology, and the Key Program of National Natural Science Foundation of China (81230033). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We acknowledge the Stanford Small Animal Imaging Facility and the Stanford Radiochemistry Facility for providing the resources required for this study.
Footnotes
Published online Jul. 23, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 26, 2015.
- Accepted for publication July 8, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.