


Article Figures & Data
Figures
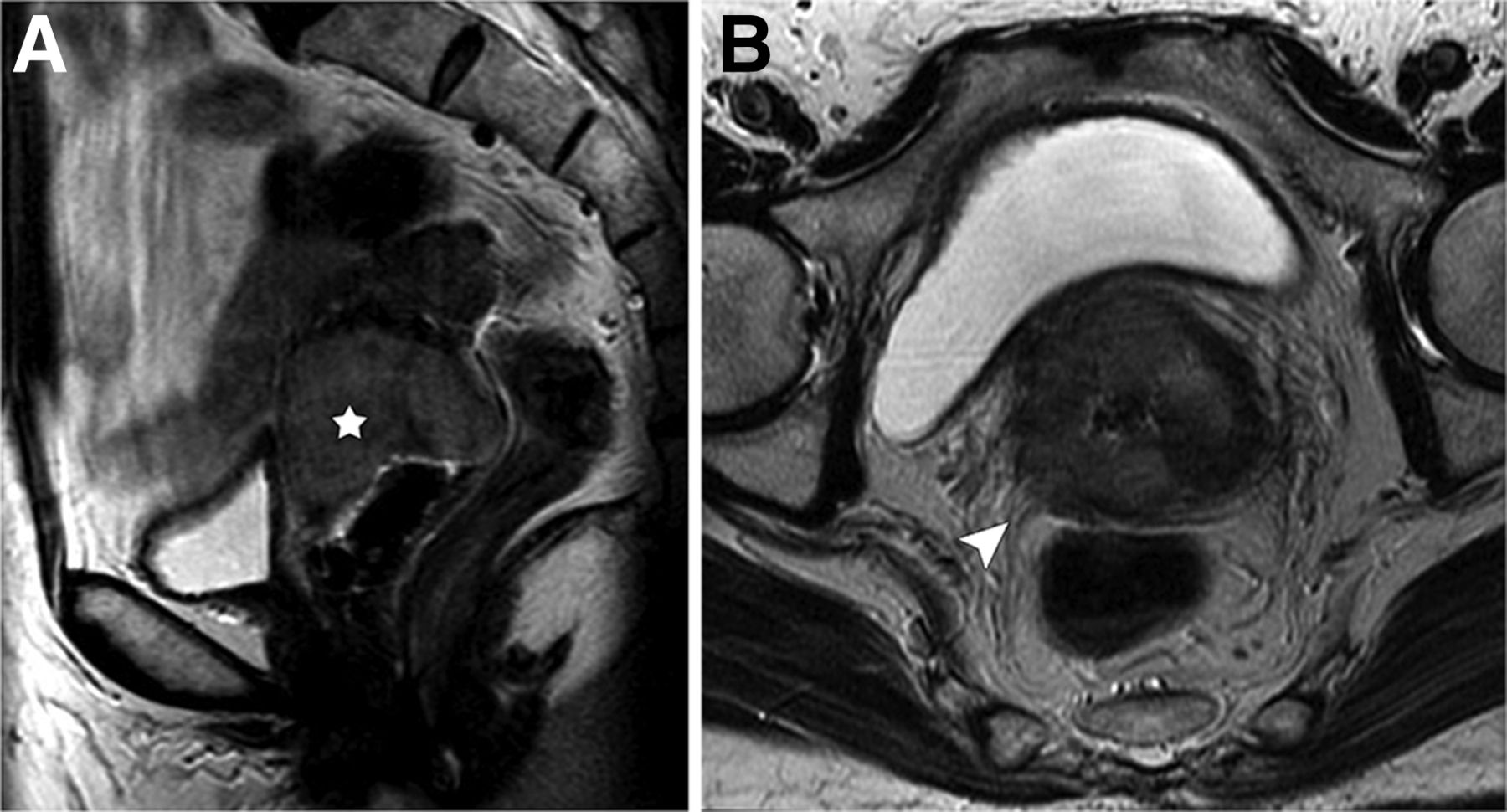
- FIGURE 1.
MR imaging of cervical cancer with parametrial extension. Fast spin echo T2-weighted sagittal image (A) shows 4.3-cm solid intermediate-signal tumor (star) that, on axial image (B), invades radially out of cervix into adjacent right parametria (arrowhead).
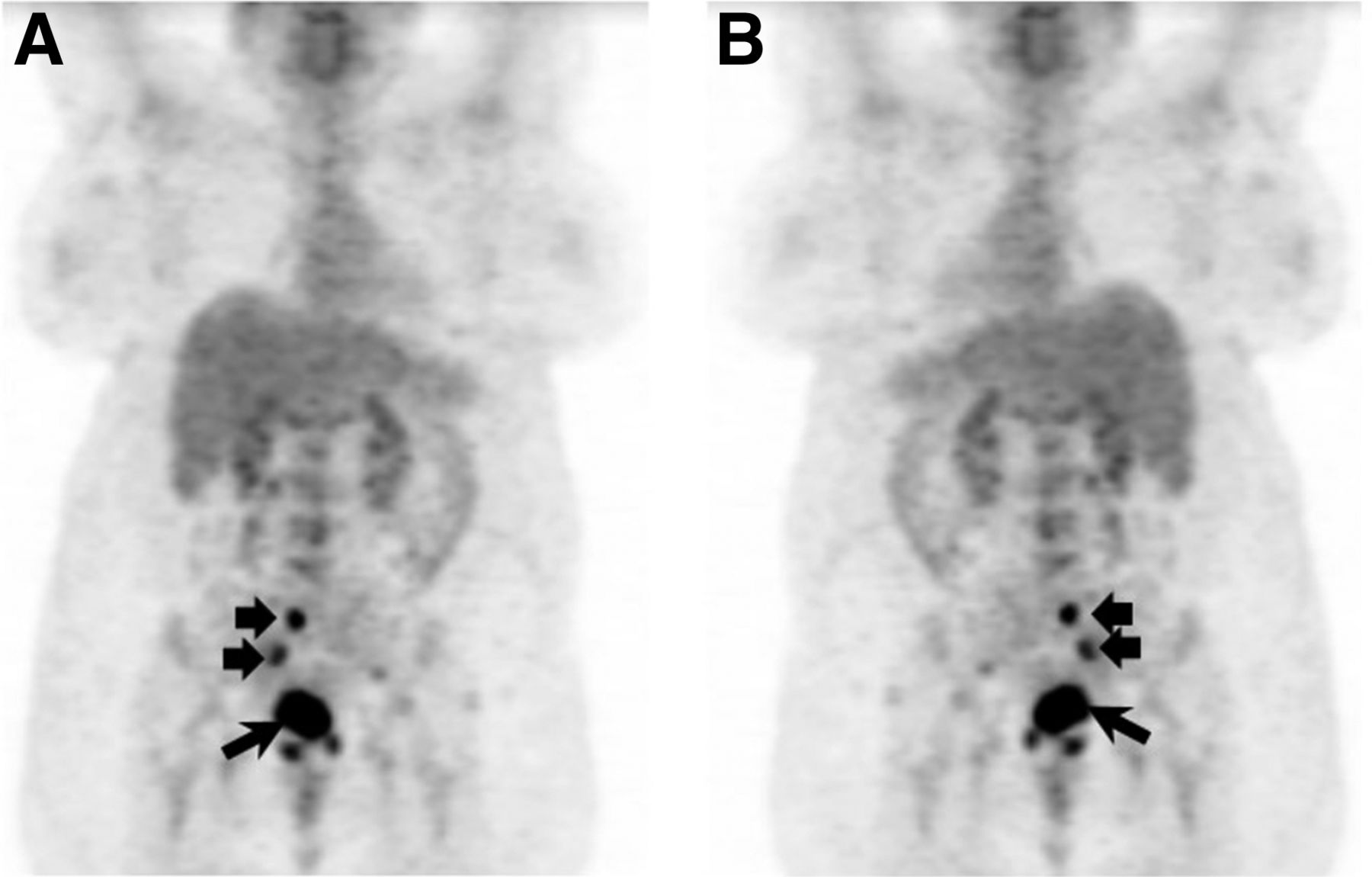
- FIGURE 2.
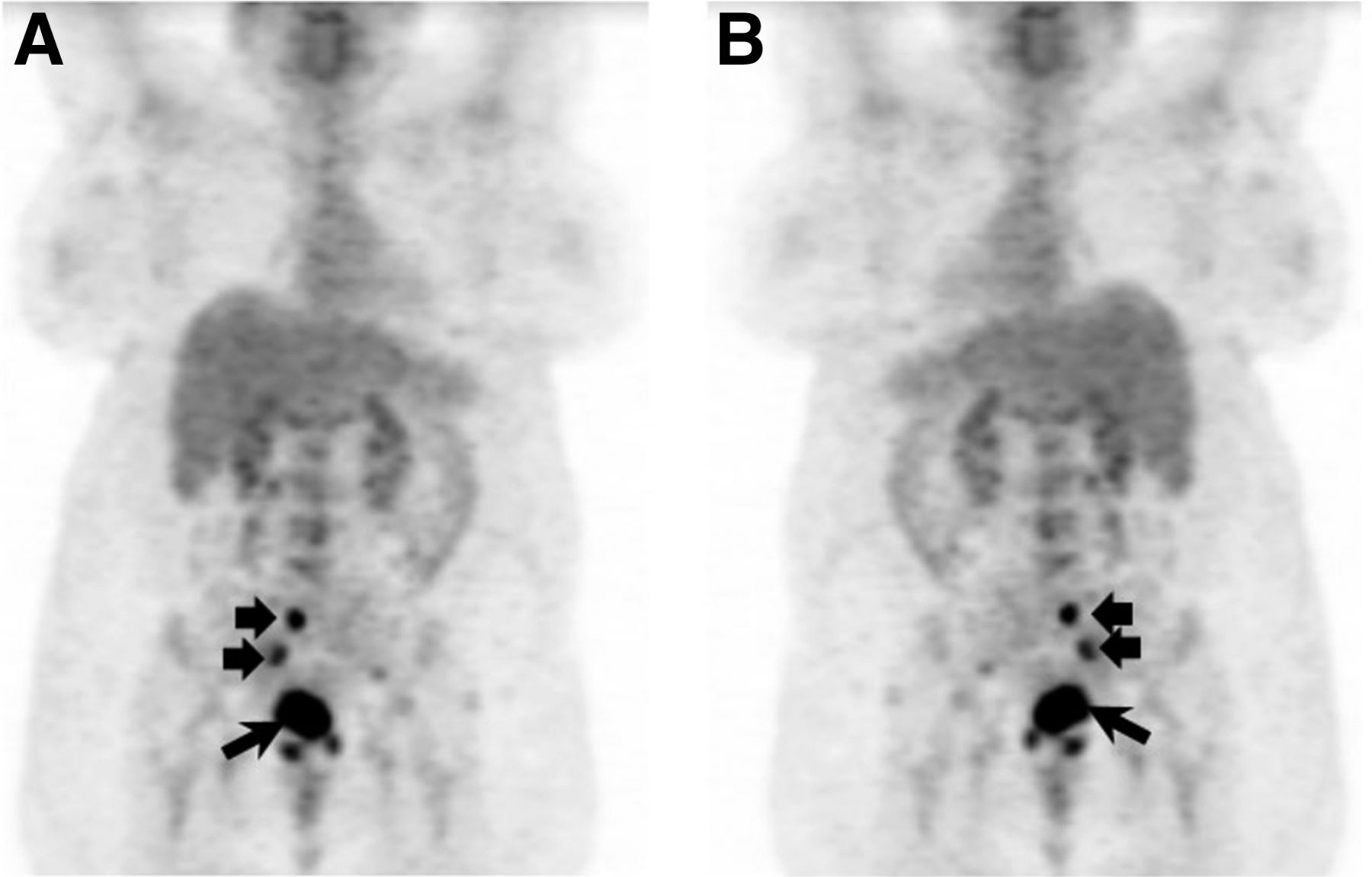
18F-FDG PET of cervical cancer lymphadenopathy. Anterior (A) and posterior (B) reprojection images demonstrate intense tracer uptake within known primary cervical carcinoma (long arrow) and right pelvic lymph node metastases (short arrows).
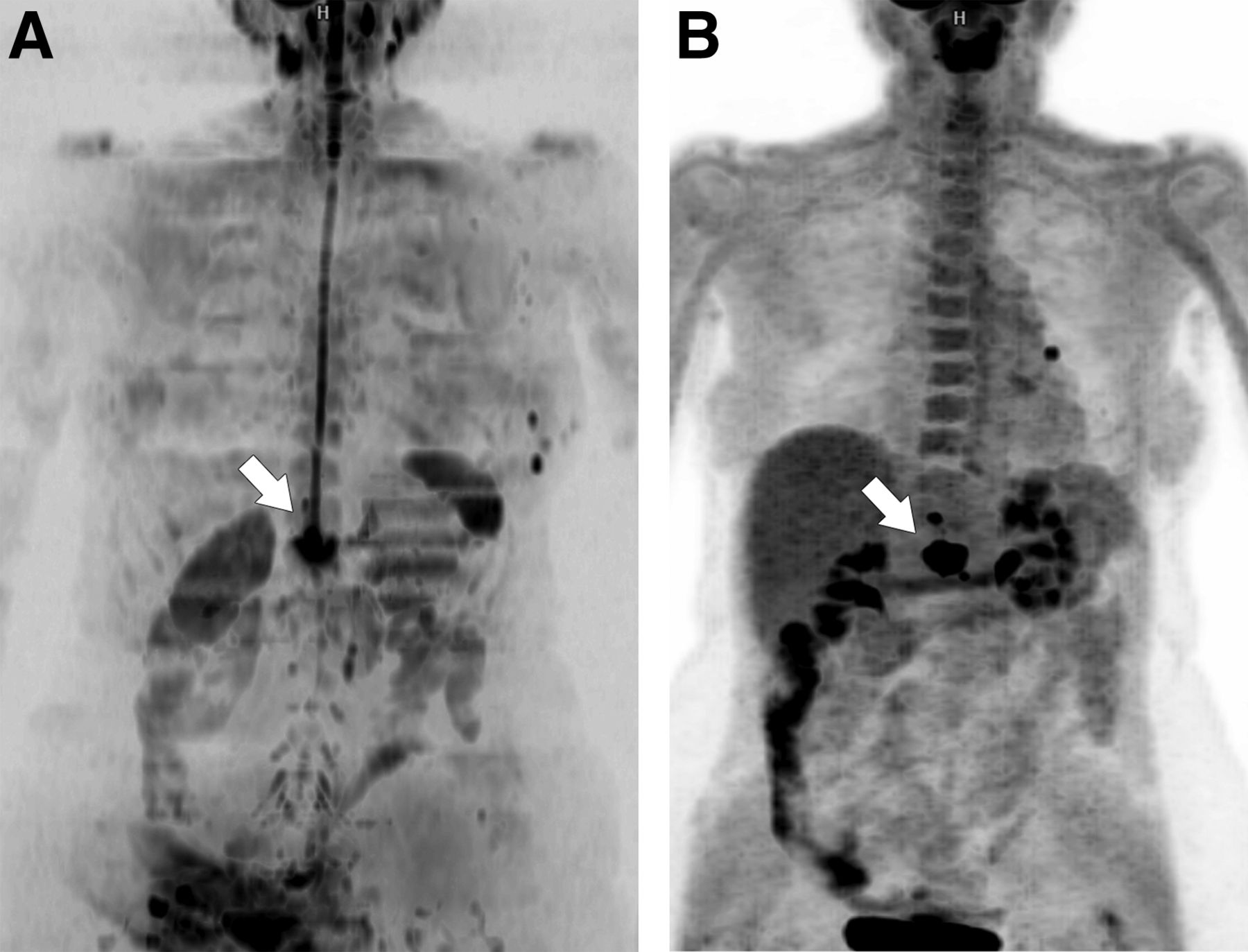
- FIGURE 3.
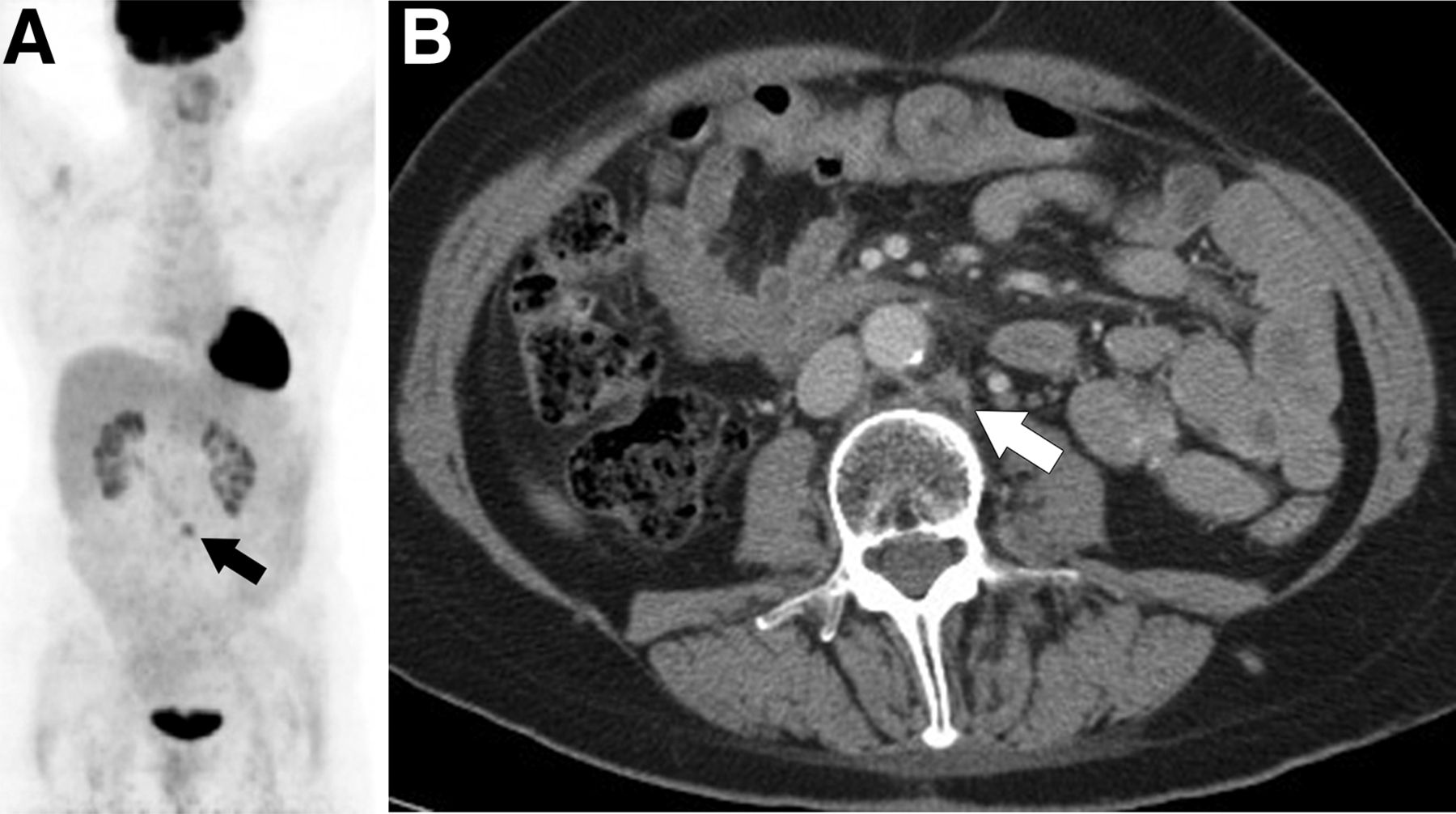
18F-FDG PET/CT of recurrent endometrial cancer. Coronal PET image (A) demonstrates focus of uptake in mid abdomen (arrow) corresponding to normal-sized paraaortic node (arrow) on diagnostic CT (B). Biopsy confirmed recurrent tumor.
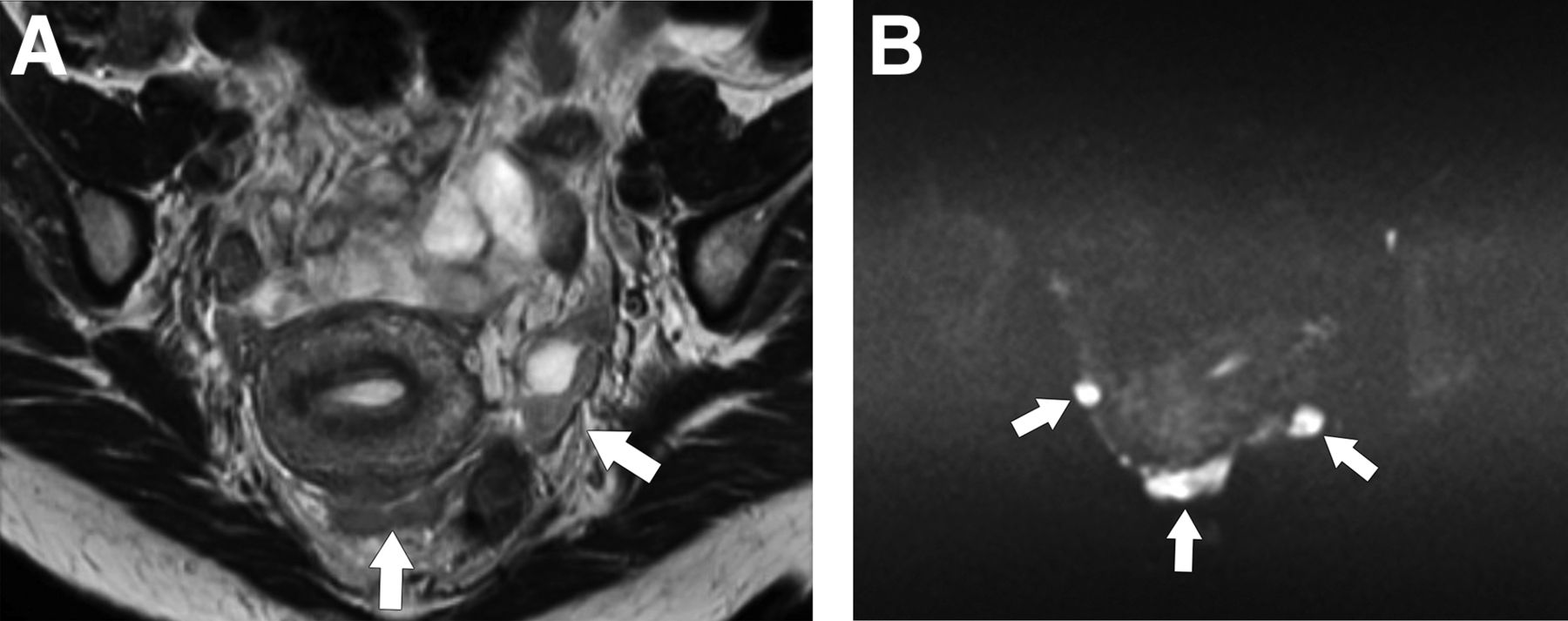
- FIGURE 4.
MR imaging of peritoneal carcinomatosis from ovarian cancer. Tumor nodules (arrows) are of intermediate signal intensity on axial fast spin echo T2-weighted image (A) but are much more conspicuous and bright on diffusion-weighted image (B).
- FIGURE 5.
Whole-body DWI (A) and 18F-FDG PET (B) images of patient with endometrial cancer recurrence in retroperitoneal node invading adjacent vertebra (arrow).
- FIGURE 6.
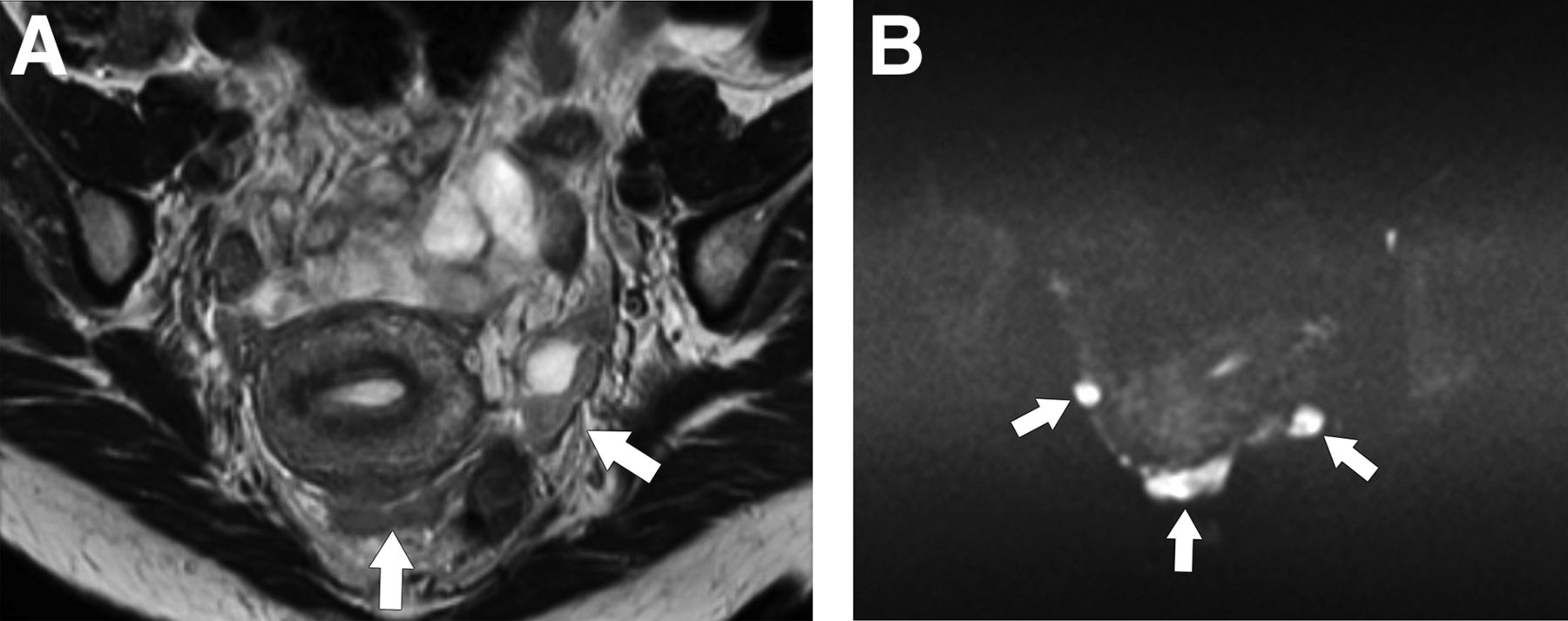
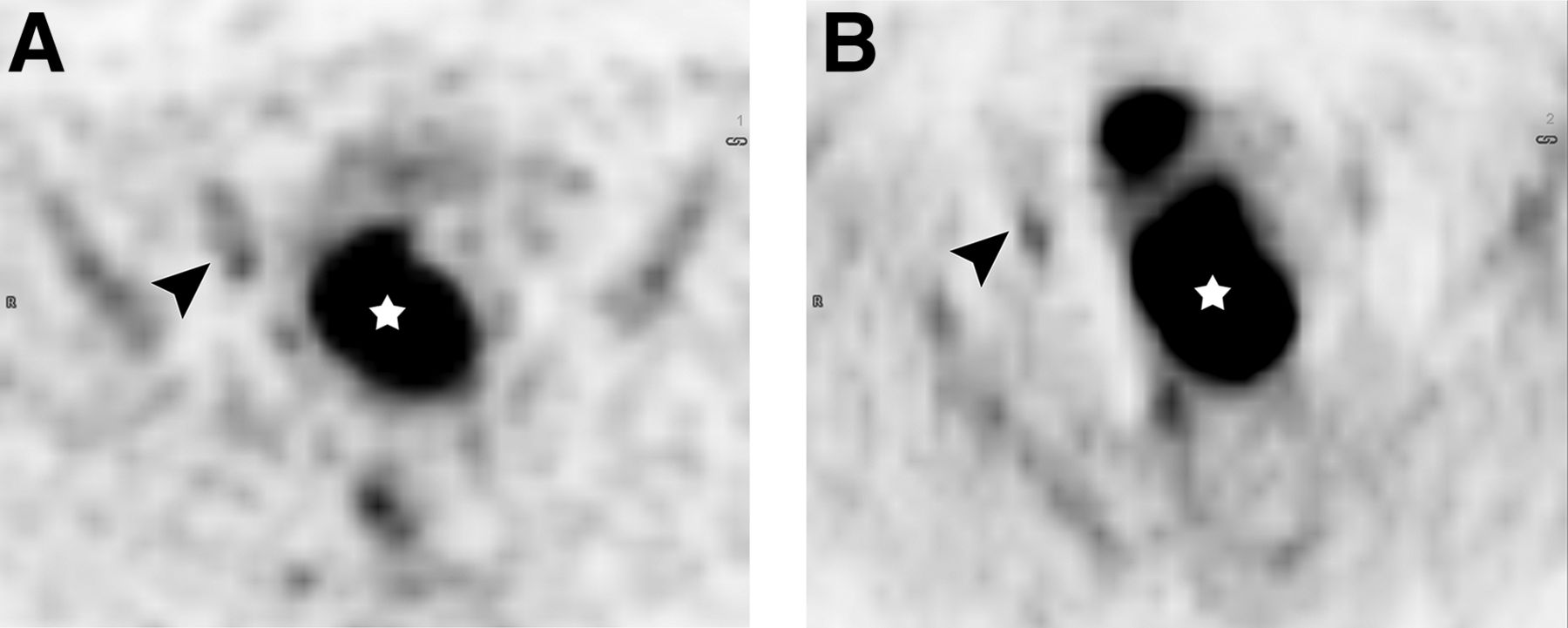
PET/MR imaging of cervical cancer with lymphadenopathy. Axial 18F-FDG PET image (A) and diffusion-weighted image (B) show 18F-FDG–avid and diffusion-restricted primary tumor (star) and right pelvic lymph node metastasis (arrowhead) confirmed pathologically. Node was normal by size criteria (not shown).
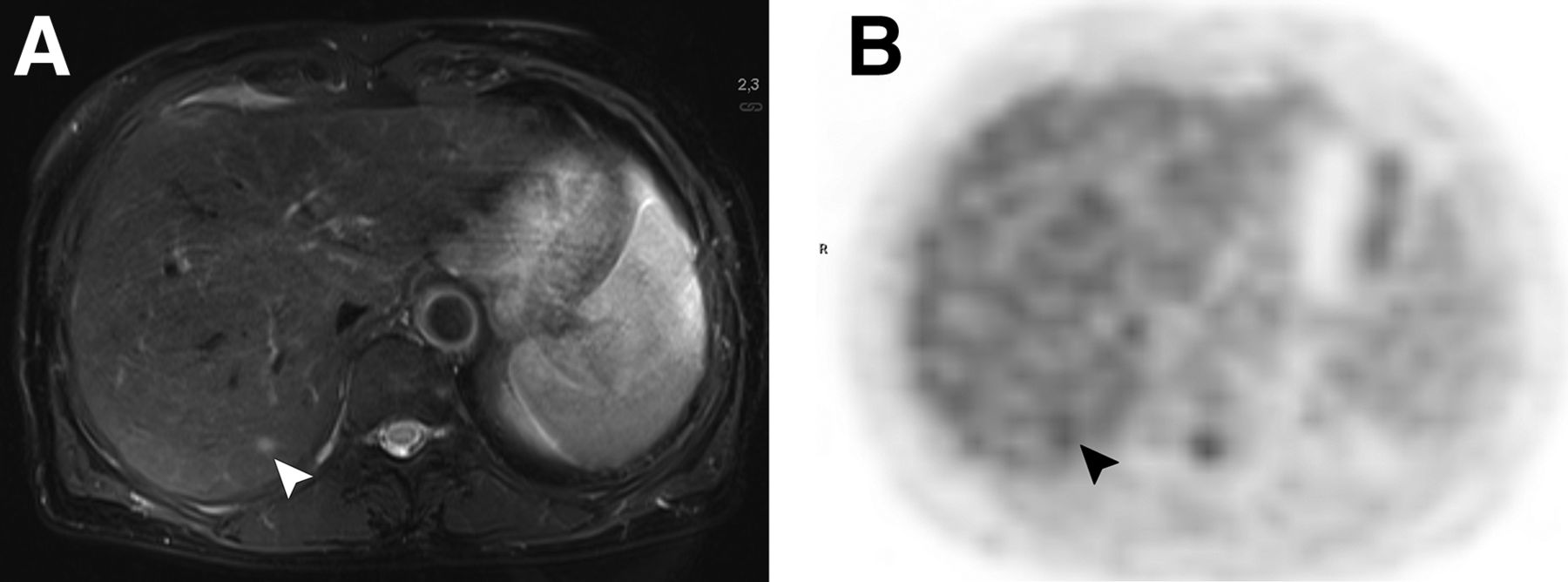
- FIGURE 7.
PET/MR imaging of liver metastasis from endometrial cancer. Axial T2-weighted image (A) shows 5-mm lesion (arrowhead) conspicuous on MR image but not on corresponding 18F-FDG PET image (B). Lesion decreased in size with chemotherapy.


Tables
Parameter MR imaging 18F-FDG PET/CT Uterine cervical cancer: pretreatment Early detection Poor Poor Differential diagnosis (benign vs. malignant) Possible Poor Extent of tumor spread Tumor size Best Poor Endocervical margin distance Best Poor Parametrial involvement Best Possible Lower-third-of-vagina involvement Possible Poor Pelvic sidewall involvement Possible Possible Hydronephrosis Possible Possible Bladder mucosal involvement Possible Poor Rectal mucosal involvement Possible Poor Pelvic and paraaortic lymphadenopathy Possible Best Distant metastases (lymph nodes and bone) Possible Best Distant metastases (liver) Best Possible Distant metastases (lung) Poor Possible Uterine cervical cancer: posttreatment Local or regional surveillance or suspected recurrence Best Possible Whole-body surveillance or suspected recurrence Possible Best Uterine endometrial cancer: pretreatment Early detection Poor Poor Differential diagnosis (benign vs. malignant) Possible Possible Extent of tumor spread Greater than half thickness of myometrium extension Best Possible Cervical stromal involvement Best Possible Uterine serosal or adnexal involvement Best Possible Vaginal or parametrial involvement Best Possible Pelvic and paraaortic adenopathy Possible Best Bladder mucosal involvement Possible Poor Bowel mucosal involvement Possible Poor Distant metastases (lymph nodes and bone) Possible Best Distant metastases (liver) Best Possible Distant metastases (lung) Poor Possible Uterine endometrial cancer: posttreatment Local surveillance or suspected recurrence Best Possible Whole-body surveillance or suspected recurrence Possible Best Ovarian cancer: pretreatment Early detection Poor Poor Differential diagnosis (benign vs. malignant) Best Poor Extent of tumor spread Ovary confined Best Poor Pelvis confined Possible Possible Abdominal involvement Possible Possible Retroperitoneal adenopathy Possible Best Peritoneal or pleural effusion Possible Poor Distant metastases (lymph nodes and bone) Possible Best Distant metastases (intraparenchymal liver) Best Possible Distant metastases (lung) Poor Possible Ovarian cancer: posttreatment Local or regional surveillance or suspected recurrence Best Possible Whole-body surveillance or suspected recurrence Possible Best Poor = poor modality choice or insufficient data; best = best modality choice; possible = possible modality choice.
Comparative assessment of modality includes clinical options, such as pelvic examination and optical imaging (e.g., colposcopy, cystoscopy, or proctoscopy), with biopsy.
Modality Sensitivity Specificity CT, cervical (5,9) 31%–57% 92%–97% CT, endometrial (22) 28%–64% 78%–94% MR imaging, cervical (5,9) 37%–55% 93%–94% MR imaging, endometrial (20,22) 59%–72% 93%–97% PET/CT, cervical (7,8) 72%–75% 96%–100% PET/CT, endometrial (20,21) 74%–77% 93%–100%
Supplemental Data
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}