


Abstract
Transient ischemic dilation (TID) in the setting of abnormal stress–rest cardiac SPECT myocardial perfusion imaging (MPI) has been linked with increased cardiovascular risk. However, the significance of TID in the setting of an otherwise normal SPECT MPI study has not been clearly established. In this study, cardiac CT was used to evaluate the prevalence of atherosclerotic lesions and the severity of coronary artery stenosis in patients with TID of the left ventricle with or without associated myocardial perfusion defects on SPECT MPI. Methods: The study population consisted of 1,553 consecutive patients who had undergone both cardiac CT and SPECT MPI within 1 mo between January 1, 2006, and September 1, 2011. Patients included in the study group had a pathologic TID value defined as ≥1.18 for men and ≥1.22 for women. Coronary CT angiography was used to evaluate each coronary segment for the presence and composition of atherosclerotic plaque and the degree of coronary stenosis. TID-positive patients were compared with a 2:1 risk-factor-matched-pair control cohort without TID. Results: TID was identified in 30 patients who were compared with TID-negative risk-factor-matched controls (n = 60). When compared with the TID-negative control cohort, TID-positive patients had no significant differences in the presence and extent of atherosclerosis, the degree of coronary artery stenosis, or the calcium score at cardiac CT. Similarly, there were no significant differences in these CT measures in TID-positive patients with a normal perfusion study (n = 20) when compared with TID-negative patients with a normal perfusion study (n = 48). In addition, there was no significant difference in the incidence of major adverse cardiac events when comparing both the TID-positive patients and the TID-negative control cohort and when comparing patients who were TID-positive with normal perfusion with patients who were TID-negative with normal perfusion. Conclusion: The presence of TID with an otherwise normal SPECT MPI study does not translate into a greater extent of coronary artery disease as assessed by cardiac CT or increased risk for future major adverse cardiac events.
- myocardial perfusion imaging
- SPECT
- coronary computed tomography angiography
- transient ischemic dilation
- coronary artery disease
Transient ischemic dilation (TID) on stress SPECT myocardial perfusion imaging (MPI) is defined as the apparent presence of left ventricular (LV) dilation on poststress relative to rest images. Several mechanisms for this phenomenon have been proposed, however, there is no clear consensus as to the pathophysiology resulting in the finding of TID (1–5). Previous studies have suggested that TID in the context of reversible myocardial perfusion defects is associated with increased risk of severe, extensive multivessel coronary artery disease (CAD) (1,6,7). TID in the setting of an abnormal SPECT MPI study has also been linked with increased cardiovascular risk and poor cardiovascular outcomes (8–11). However, the significance of TID in the setting of an otherwise normal SPECT MPI study has not been clearly established. It is thought that TID in the setting of an otherwise normal MPI study may represent balanced ischemia, which would make relative perfusion defects difficult to visualize and would put these patients into a high cardiovascular risk category. However, insufficient data are available on the coronary status of patients with TID and normal SPECT MPI studies, and no study has investigated atherosclerotic plaque burden and composition using coronary CT angiography (cCTA) in such patients.
In an effort to further define the clinical significance of TID in the setting of normal SPECT MPI studies, we used cCTA to evaluate in detail the prevalence and severity of coronary artery stenosis as well as atherosclerotic lesions and their composition (calcified, noncalcified, mixed) in patients with TID and normal SPECT MPI studies. We compared our findings with an age-, sex-, race-, and risk-factor-matched control group without TID and patients with TID and pathologic SPECT MPI studies.
MATERIALS AND METHODS
Study Design and Patients
The study protocol was approved by the Institutional Review Board who waived the need for individual patient informed consent for this retrospective analysis. This study was conducted in compliance with the Health Insurance Portability and Accountability Act. The population consisted of 1,553 consecutive patients who had undergone both SPECT MPI and cCTA within a month of each other between January 1, 2006, and September 1, 2011. Patients who had undergone previous revascularization or interventional procedures between SPECT MPI and cCTA imaging were excluded.
The study patients were those with a pathologic TID value defined as ≥1.18 for men and ≥1.22 for women (6), yielding a total of 30 patients with a finding of TID, of which 10 patients had a myocardial perfusion defect and 20 patients who had an otherwise normal SPECT MPI study. A SPECT MPI study was classified as showing a myocardial perfusion defect if the defect was medium or large. If the defect was considered small, the SPECT MPI study was classified as positive for a perfusion defect if the lesion was thought to represent a true perfusion defect rather than an artifact.
The patients with TID were matched to TID-negative control patients in a 1:2 ratio for age within 2 y, race, sex, and presence of major cardiovascular risk factors (hypertension, hyperlipidemia, nicotine abuse, family history, body mass index [BMI], and diabetes mellitus).
Outcome data were retrospectively collected on all patients in both the study and the control group by chart review through September 1, 2013. The length of follow-up varied from 3 to 7 y. We recorded the occurrence of major adverse cardiac events (MACEs) including cardiovascular death, nonfatal myocardial infarction, coronary revascularization, and acute coronary syndrome. There was only 1 patient lost to follow-up of the 90 patients in the study.
Cardiovascular Risk Factors
Hypertension was defined by a blood pressure of ≥140 mm Hg systolic or ≥90 mm Hg diastolic or use of antihypertensive medication. Diabetes mellitus was defined as fasting glucose ≥ 126 mg/dL or use of antidiabetic treatment. Hyperlipidemia was defined as a total cholesterol level of ≥200 mg/dL or use of lipid-lowering medication. Patients were considered smokers only if current tobacco use was stated. A positive family history was defined as a first-degree relative with a history of premature (women < 65 y or men < 55 y) myocardial infarction or sudden coronary death.
Stress–Rest SPECT MPI Protocol
SPECT MPI acquisition and processing were performed in accordance with guidelines of the American Society of Nuclear Cardiology (12). In summary, a single-day rest–stress MPI protocol was used, with approximately 370 MBq (10 mCi) and 1,110 MBq (30 mCi) of either 99mTc-sestamibi or 99mTc-tetrofosmin administered intravenously at rest and stress, respectively. On the basis of the physician’s assessment and discretion, the patients completed either a treadmill exercise stress protocol or a pharmacologic vasodilator protocol, in accordance with guidelines of the American Society of Nuclear Cardiology. Exercise stress tests were completed using either a Bruce or a modified Bruce treadmill protocol, and the stress dose of radiotracer was administered at symptom-limited peak stress, for example, physical fatigue. In the event of an inadequate exercise stress test, for example, failure to reach target heart rate (85% of the age-predicted maximal heart rate), the patient was immediately converted to the pharmacologic stress test protocol. Pharmacologic stress tests were completed using 0.4 mg of regadenoson (Lexiscan; Astellas) administered via intravenous bolus, followed by a normal saline flush. The stress dose of radiotracer was administered intravenously approximately 20 s after regadenoson. Stress tests were supervised by a cardiologist and completed according to standard protocols (13).
Sixteen-phase electrocardiogram (ECG)-gated and nongated stress and rest images were acquired with a dual-head, T2 or T6, hybrid SPECT/CT camera (Symbia; Siemens Medical Solutions). Low-dose attenuation-correction CT scans were acquired immediately after the rest and stress SPECT image acquisitions. The studies were reconstructed using Siemens Syngo VA60A software. Emission data were reconstructed using a gaussian smoothing filter with scatter correction, followed by FLASH3D (Siemens) iterative reconstruction (8 iterations and 8 subsets). Rest data were filtered with a full width at half maximum of 12.0, and stress data used a full width at half maximum of 9.0. Gated rest and stress data were reconstructed with filtered backprojection and Butterworth smoothing, using a 0.25 cutoff with an order of 5 and a 0.3 cutoff with an order of 5, respectively. Short-axis, horizontal long-axis, and vertical long-axis images were automatically generated. In cases for which the software failed to detect LV contours, manual contour correction was performed by an experienced technologist. Also, if there was significant patient motion noted during review of raw projections, motion-correction software was applied. Automated analysis of the reconstructed acquisition data was performed using Corridor4DM software (version 2010; Invia Medical Imaging Solutions). Semiquantitative analysis was performed on a 5-point scale (0, normal; 1, equivocal; 2, moderate; 3, severe reduction in tracer uptake; and 4, no detectable uptake) based on a 17-segment model (14). Cine wall motion and wall thickening analyses were also performed, and LV ejection fraction was calculated. Two experienced observers, masked to patient data and all imaging results, in consensus evaluated myocardial perfusion images for reversible and fixed perfusion defects.
For the purposes of this study, the reported TID ratios were based on the gated SPECT images. Automated analyses of the reconstructed images were completed by Corridor4DM-SPECT computer software (14), which automatically determined the apex, base, and myocardial borders of the left ventricle. The sums of the calculated rest and stress gated SPECT data were used to automatically calculate the total nongated 3-dimensional LV volumes. From these values, the TID, defined as the ratio of LV volumes at stress and rest, was automatically calculated by the Corridor4DM-SPECT software.
CT Scan Acquisition and Reconstruction Protocol
cCTA studies were acquired on first- or second-generation dual-source CT systems (Siemens). Initially, noncontrast CT coronary artery calcium scoring was performed. The cCTA scan protocol was chosen on the basis of individual patient characteristics (heart rate/rhythm, BMI) with the goal of minimizing radiation exposure. Scan protocols included prospectively ECG-triggered high-pitch spiral acquisitions (with second-generation dual-source CT), prospective ECG triggering, and traditional retrospective ECG gating with default use of ECG-dependent tube current modulation. Contrast medium enhancement was achieved by injection of 60–90 mL of iodinated contrast material (Iopromide, Ultravist 370 mgI/mL; Bayer), injected at 6 mL/s through an 18-gauge intravenous antecubital catheter using a dual-syringe injector (Stellant D; Medrad). Scanning parameters were 2 × 128 × 0.6 mm (2 × 64 × 0.6 mm for first-generation dual-source CT) section acquisition and 280 ms (330 ms for first-generation dual-source CT) gantry rotation time. A 120-kV tube potential was used in patients with a BMI > 25 kg/m2, whereas the tube potential was reduced to 100 kV in patients with a BMI < 25 kg/m2.
Coronary CT Angiogram Evaluation
For the evaluation of CAD, the 17-segment model based on the American Heart Association classification was used (15). Two experienced observers in consensus assessed the degree of stenosis using automatically generated curved multiplanar reformations along the vessel centerline (Circulation; Siemens). Coronary segments were visually graded as normal (0%–25% lumen diameter narrowing), moderate stenosis (26%–50% lumen diameter narrowing), or significant stenosis (lumen diameter narrowing > 50%). Coronary atherosclerotic plaque was visually classified per segment according to the CT-based criteria of coronary artery atherosclerosis as either calcified or noncalcified (16–18). Mixed plaque was defined by the presence of both calcified and noncalcified components.
Statistical Analysis
Categoric data were presented as frequencies and percentages and were compared using the χ2 test. Normally distributed continuous data were presented as mean ± SD and were compared using the 2 tailed t test for independent samples. In the case of nonnormal distribution, we evaluated the differences in plaque volume between TID-positive patients and their control groups using the Mann–Whitney test. All statistical analyses were performed using SPSS software (release 18.0; SPSS). A P value < 0.05 was considered statistically significant.
RESULTS
Baseline characteristics and demographics of patients with TID and their matched-pair controls are provided in Table 1. There were no statistically significant differences in the prevalence of risk factors in the study patient cohort and matched controls including age, race, sex, hyperlipidemia, hypertension, diabetes mellitus, family history, BMI, or smoking (P > 0.05).
Baseline Patient Characteristics
Variables regarding SPECT myocardial perfusion image acquisition and interpretation are summarized in Table 2. Patients in the TID-positive group had a TID value of 1.29 ± 0.1, and patients without TID had a TID value of 0.94 ± 0.13. Fourteen patients in the TID-positive group had undergone a pharmacologic vasodilator study, and 18 patients in the TID-negative control cohort had undergone exercise stress. We also recorded the presence of atrial fibrillation, the maximum heart rate, and the maximum systolic blood pressure. There were equally no differences between heart rate, blood pressure during stress, and the presence of atrial fibrillation between the 2 groups, suggesting no difference in hemodynamics between the 2 groups during SPECT MPI.
Patient Physiologic Parameters During SPECT MPI
When all patients with TID (n = 30) were compared with the non-TID control group (n = 60), there were no significant differences in the presence or extent of atherosclerotic plaque (P = 1.00), the calcium score (P = 0.98), the presence and number of significant stenosis (>50%) in one of the major cardiac vessels (left main, left anterior descending, left circumflex, right coronary artery) (P = 0.80), or the presence of a perfusion defect on SPECT MPI (P = 0.20). Therefore, in this study the presence of TID was not associated with more advanced atherosclerosis, coronary stenosis, or evidence of ischemia (Fig. 1).
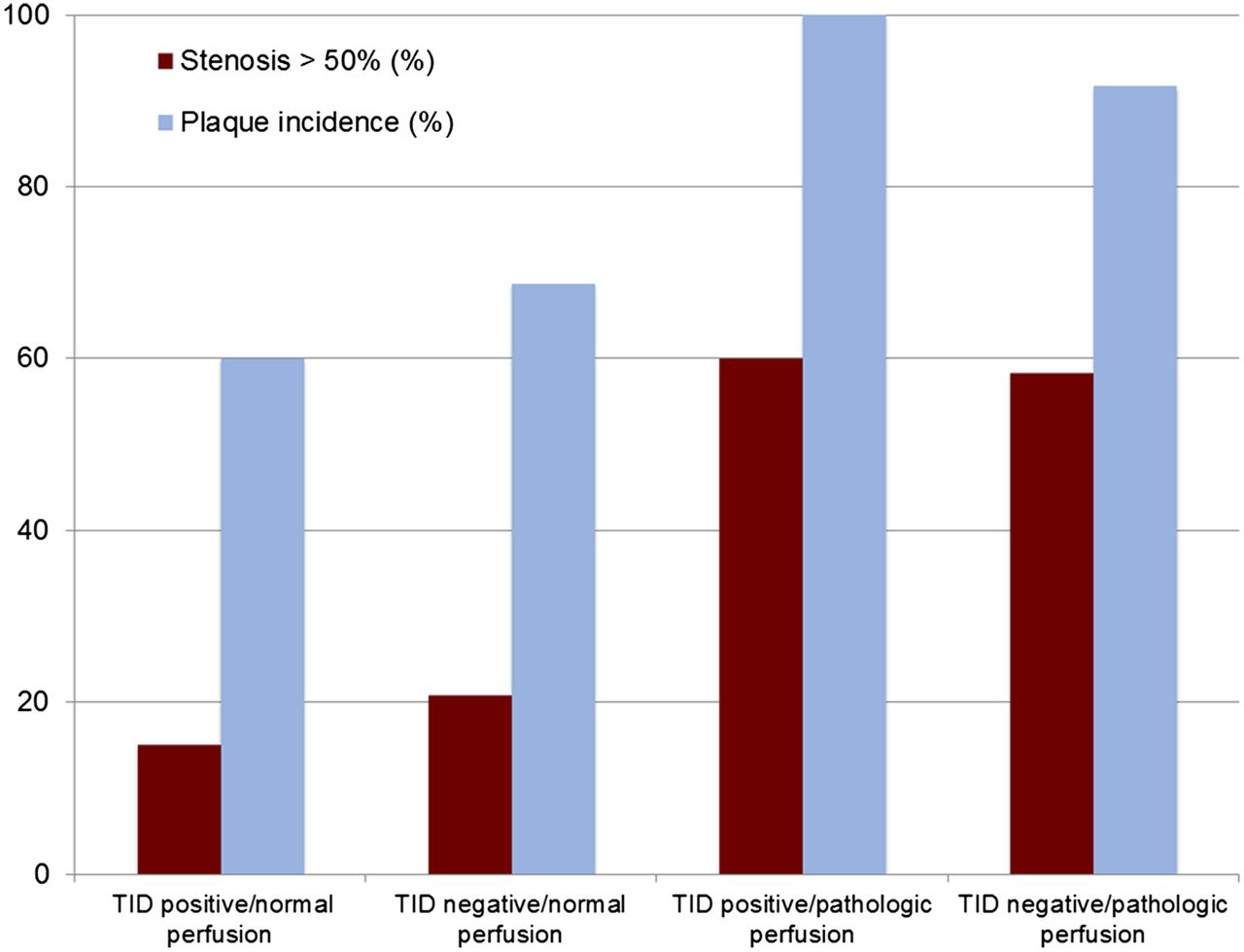
Prevalence of coronary artery plaques and significant stenosis. Prevalence of coronary artery plaque and significant stenosis found on cCTA in TID-positive and -negative patients in setting of both normal and pathologic myocardial perfusion on SPECT.
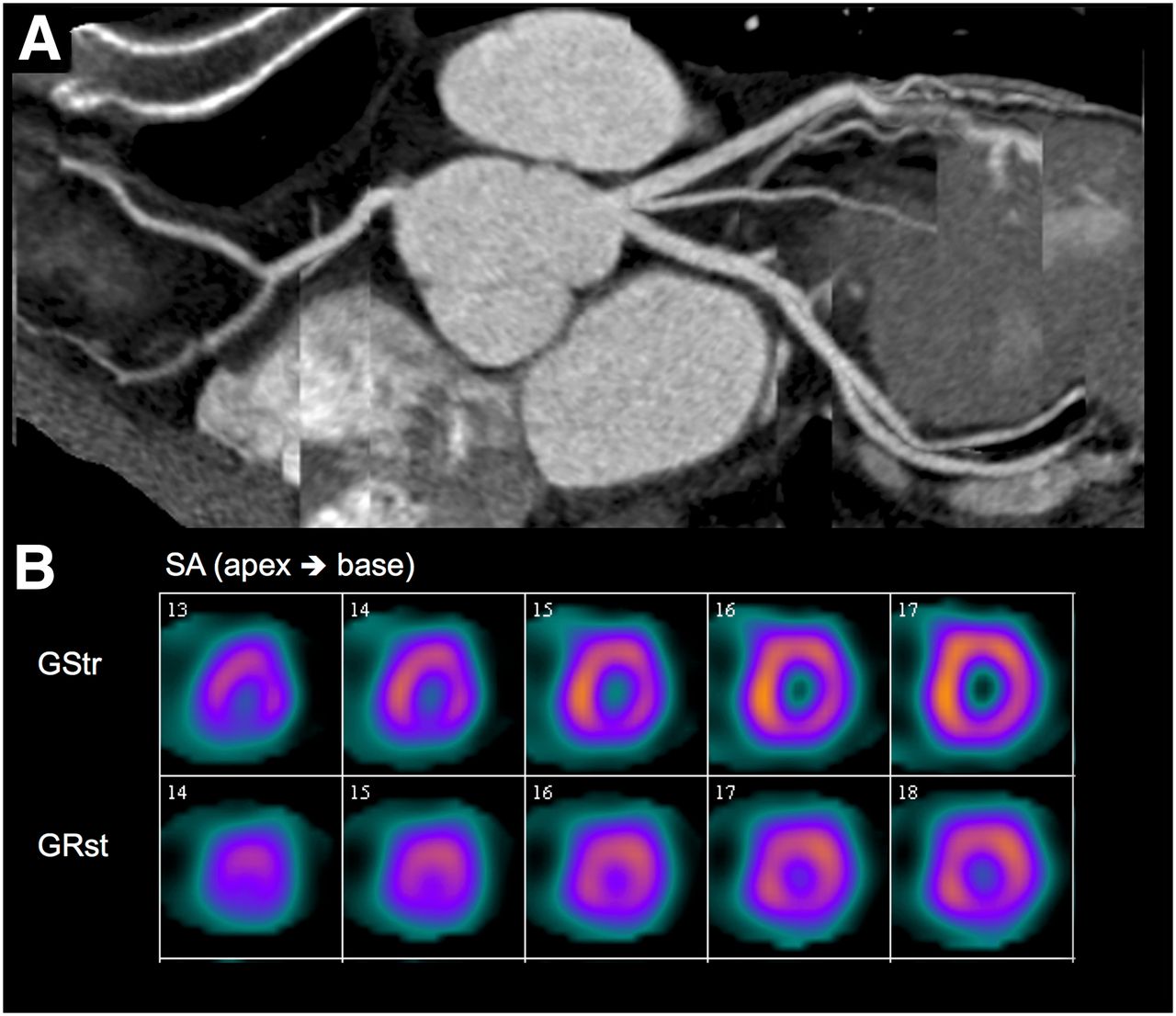
Comparing patients who were TID-positive with no perfusion defect (n = 20) (Fig. 2) with patients from the control group who were TID-negative with no perfusion defect (n = 48), we found no significant differences in the presence or extent of atherosclerotic plaque (P = 0.58/P = 0.32), the calcium score (P = 0.90), or the presence of significant stenosis (>50%) (P = 0.74). Accordingly, in patients with normal myocardial perfusion on SPECT MPI the finding of TID was not predictive of more advanced atherosclerosis or of more significant coronary artery stenosis in this cohort. In patients from the study and control populations with a perfusion defect, patients with TID (n = 10) (Fig. 3) did not have a greater prevalence or severity of atherosclerosis or coronary stenosis when compared with patients who were TID-negative (n = 12) (P > 0.05). Thus, in the presence of evidence of myocardial ischemia, TID was not predictive of a significant increase in underlying plaque or coronary obstruction.
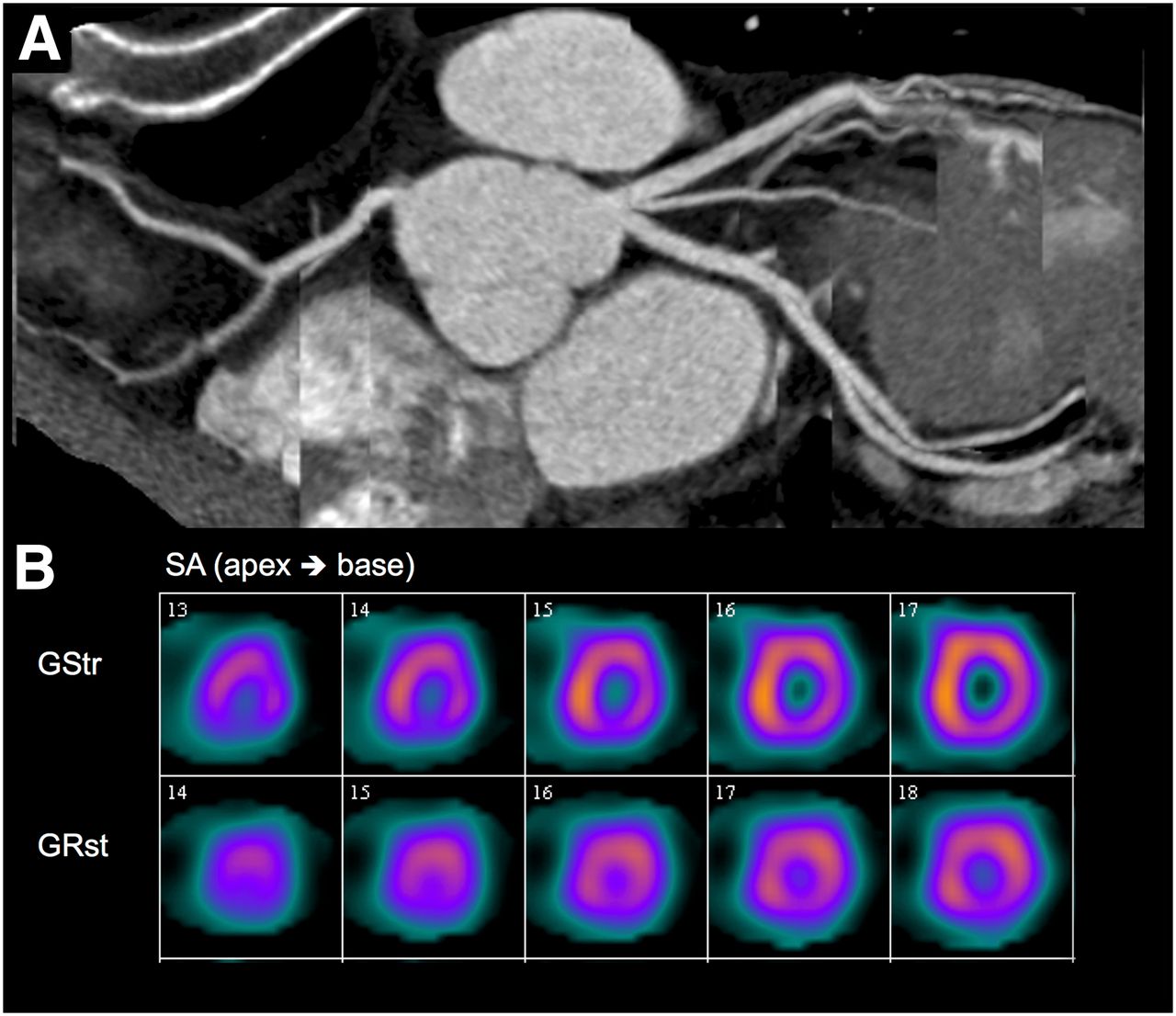
cCTA and SPECT in TID-positive/normal perfusion patient. A 54-y-old woman with exclusion of CAD at cCTA (A) and normal myocardial perfusion on SPECT imaging (B). GRst = (ECG)-gated rest study; GStr = (ECG)-gated stress study; SA = short axis.

cCTA and SPECT in TID-positive/pathologic perfusion patient. (A) A 68-y-old man with significant coronary artery stenosis of proximal and mid portion of left anterior descending artery (arrows). (B) SPECT imaging revealed myocardial perfusion defect in corresponding segments. GRst = (ECG)-gated rest study; GStr = (ECG)-gated stress study; SA = short axis.
When TID-negative patients without perfusion defects (n = 48) were compared with patients who were TID-negative with a perfusion defect (n = 12), patients with a perfusion defect had a significantly (P < 0.05) higher prevalence of plaque and significant (>50%) stenosis (Fig. 1).
On outcome analysis, there were 2 of 30 patients with TID and 4 of 60 patients in the non-TID control group who suffered a MACE during follow-up. There was no significant difference between the incidence of MACEs in patients with TID versus the non-TID control group (P = 1.0). In patients who were TID-positive without perfusion defect, 1 of 20 suffered a MACE during follow-up, compared with 1 of 48 patients from the control group who were TID-negative without perfusion defect. Again, there was no significant difference in the incidence of MACEs when comparing these 2 groups (P = 0.52). However, there was a significantly (P = 0.004) higher incidence (3/12) of MACEs in the group of patients who were TID-negative with a perfusion defect than in the group that was TID-negative without perfusion defect (1/48).
DISCUSSION
The purpose of this study was to evaluate the degree of coronary stenosis as well as atherosclerotic plaque composition and extent on cCTA in patients with TID on SPECT MPI. The subgroup of patients with isolated TID without associated myocardial perfusion abnormalities is of particular interest because the literature has been inconclusive on the clinical significance of this finding as a marker of high risk of cardiac events. In this study, findings at cCTA in patients with TID were compared with a risk-factor-matched-pair control group without TID. Results suggest that the presence of TID in the setting of a normal SPECT MPI study is not associated with more extensive atherosclerotic plaque or a greater degree of coronary stenosis. As expected, patients with a perfusion defect were significantly more likely to have CAD, compared with patients with normal perfusion independent of the finding of TID on SPECT MPI.
Several mechanisms have been described to explain the finding of TID in the setting of an otherwise normal SPECT MPI study. The first mechanism commonly discussed suggests that the count-poor, severely ischemic subendocardium at stress appears during imaging to be part of the LV cavity surrounded by a rim of better perfused epicardium. In comparison to images at rest, perfusion is improved in the subendocardium and the LV cavity appears smaller (4). This phenomenon is often referred to as balanced ischemia (5). Other studies have linked long-standing hypertension to the presence of TID (5,19). This condition also results in a relative reduction in subendocardial perfusion during stress, possibly because of the increased epicardial diastolic pressure required to perfuse the entire width of the myocardium. Diabetes mellitus has been associated with the finding of TID in the setting of normal perfusion studies (20). Emmett et al. suggested that the microvascular disease caused by diabetes could cause subendocardial ischemia and result in the finding of TID (21). In our study, however, we controlled for both hypertension and diabetes, ensuring there was no significant difference in the prevalence of these risk factors between the study patient cohort and matched controls.
Small cardiovascular outcome studies have evaluated the clinical implication of the presence of TID in patients with otherwise normal myocardial perfusion on SPECT MPI. Abidov et al. found that this patient group, especially patients in the highest quartile of elevated TID values, had an independent and incremental risk for future cardiac events. The investigators advised against reporting such patients to be in a low-risk category (22). However, a more recent study by Valdiviezo et al., including more than 20,000 patients undergoing SPECT MPI, compared 28 patients with TID and otherwise normal myocardial perfusion to findings on catheter angiography. Results demonstrated that TID with a normal SPECT MPI study was not associated with more extensive or severe CAD. There were no differences in the prevalence of coronary disease at catheter angiography, the number of vessels with significant coronary stenosis, the presence of multivessel or left main disease, or the CAD prognostic index (23). Mandour Ali et al. investigated the predictive accuracy and the statistical frequency of false-positive TID findings in patients with normal MPI studies. Results indicated that the prevalence of TID in patients with an otherwise normal SPECT MPI study is low and that measurement variance is the cause of most TID findings in patients with normal SPECT MPI, which in turn leads to a poor predictive accuracy of TID and poor correlation with adverse cardiac outcomes (24).
The results in the current study, which, to our knowledge, represent the first cCTA evaluation of patients with TID and normal myocardial perfusion on SPECT MPI, are consistent with the catheter angiographic findings of Valdiviezo et al. However, cCTA provides additional information regarding the presence and composition of nonobstructive atherosclerosis, which may not be demonstrated at catheter angiography. In this study, patients with TID and normal perfusion did not have more extensive CAD by cCTA, compared with patients in the risk-factor-matched control group with no TID and normal perfusion. No significant increase in the prevalence of atherosclerosis (P = 0.58) or high-degree coronary vessel stenosis (P = 0.74) was found. In addition, there was no significant increase in the number of atherosclerotic plaques, including calcified, noncalcified, and mixed plaques (P = 0.32). There was no evidence that the finding of TID in the setting of a normal myocardial perfusion suggests the presence of balanced ischemia due to more severe multivessel disease, compared with patients with TID-negative studies.
In the complete TID study population (n = 30), including 10 patients with perfusion defects and 20 patients with normal perfusion, there were no differences on cCTA indicative of more advanced atherosclerosis or obstructive CAD when compared with the TID-negative control group. In addition, patients with TID did not have a statistically significant increase in presence of myocardial perfusion defects when compared with the control population without TID (10/30 vs. 12/60; P = 0.197).
Furthermore, patients who were TID-positive with a perfusion defect (n = 10) did not have a significant increase in the severity for CAD, including the number of significant stenosis and the incidence of atherosclerotic plaques (P = 0.67, P = 1.00), compared with patients who were TID-negative with a perfusion defect (n = 12). This finding is in contrast to previous studies that have suggested that the finding of TID in the setting of a perfusion defect is indicative of severe and extensive CAD (1,6,7).
As expected, the presence of a perfusion defect predicted a significant increase in the cCTA findings consistent with CAD. Consistent with the findings of Valdiviezo et al., these data suggest that TID, regardless of the presence or absence of a perfusion defect, may not be as strong an indicator of high-risk CAD as past studies have suggested.
Mandour Ali et al. concluded that measurement variance is the cause of most TID findings in patients with an otherwise normal SPECT MPI study, which in turn may lead to a poor predictive accuracy of TID and poor correlation with adverse cardiac outcomes (24). We agree that in the broader population of patients with TID and an otherwise normal SPECT MPI study, variance may lead to the poor predictive accuracy of TID. However, in our study population the TID-positive group had a significantly higher TID value (1.29 ± 0.1, compared with 0.94 ± 0.13 in patients without TID), which would argue against measurement variance as an explanation for the differences on cCTA and outcomes between patients with and without TID observed in our study.
Our analysis of outcome data revealed no significant difference in the incidence of MACE in patients with TID versus the non-TID control group. In addition, there was no difference in the incidence of MACE in TID-positive patients without perfusion defect when compared with those in the control group who were TID-negative without perfusion defect. The outcome data suggest that TID without a perfusion defect may not be as strong an indicator of high-risk CAD as past studies have postulated. Overall, the outcome data further support our conclusion that patients with TID in the setting of an otherwise normal SPECT MPI study are not at an elevated risk for future MACEs, and further invasive work may not be routinely warranted.
As expected, there was an increased risk for MACE in TID-negative patients with a perfusion defect when compared with TID-negative patients without perfusion defect. This suggests that a perfusion defect correlates with MACE, which has been well described in the literature (1,6,7) and is consistent with our findings on cCTA.
Despite the common notion that TID is a high-risk finding, more recent evidence and the results of the current study suggest that in the setting of a normal SPECT MPI study referral to invasive angiography may not be routinely warranted. The use of cCTA in patients with TID may be an effective noninvasive imaging procedure to further evaluate the extent of underlying atherosclerosis in these patients. Clinically, patients who have TID in the setting of an abnormal SPECT MPI study should continue to be regarded as a high-risk population and further work-up is warranted. However, TID does not reliably predict more extensive atherosclerotic plaque, differences in plaque composition, multivessel disease, or clinically significant coronary stenosis.
The study was conducted at a single academic center with a potentially unique tertiary care referral patient population. Therefore, the findings may not be applicable to all patient populations and medical facilities. This study might also be limited by the potential for referral bias because the patient population consisted of individuals who underwent both cCTA and SPECT MPI at our institution. The potential for individuals who had more severe cardiac symptoms and received multiple modality work-ups may skew the overall results. However, the use of 2 relatively noninvasive means of cardiac evaluation is less likely to skew the data than previous studies that evaluated the presence or absence of CAD with invasive techniques.
Another limitation of our study is the relatively small sample size. Our sample started with 1,553 patients who received both cCTA and stress MPI testing. Approximately 1.9% of screened patients were found to be TID-positive, which is consistent with the published overall incidence of TID on SPECT MPI of 1%–2% of the population of patients undergoing SPECT MPI. The small cohort of patients with both cCTA and stress testing was the limiting factor for this study sample, and future larger, multicenter studies are needed.
CONCLUSION
The presence of TID with an otherwise normal SPECT MPI study does not translate into a greater extent of CAD as assessed by cCTA or risk for future MACEs. Therefore, further invasive work-up in this group of patients may not be routinely warranted. Patients with TID and myocardial perfusion defects, however, should be regarded as a high-risk population.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. U. Joseph Schoepf receives research support from and/or is a consultant for Bayer, Bracco, General Electric, Medrad, and Siemens. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 24, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
RERERENCES
- Received for publication May 6, 2013.
- Accepted for publication February 24, 2014.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.