


Abstract
Folate receptor (FR) can be used as a therapeutic target because of its expression on different epithelial cancers, such as ovarian, non–small cell lung, endometrial, and breast cancer. Assessing FR expression in tumors may help to identify patients who can benefit from FR-targeted therapeutics, such as vintafolide and farletuzumab. Different methods exist to detect FR expression. Tissue sampling has limited clinical utility, mainly because it requires an invasive procedure. 99mTc-etarfolatide, a 99mTc-labeled folate conjugate, is in late-phase trials in Europe and the United States. It allows noninvasive, whole-body imaging of the FR. This review focuses on this FR-imaging agent and how it may be used to direct FR-targeted therapy.
FOLATE RECEPTOR AND CANCER
Folate is a water-soluble B vitamin that is essential for cellular processes such as nucleotide biosynthesis (1). Cellular folate transport can be mediated by folate receptors (FRs), of which the α and β subtypes are the most studied (2).
FR expression has been shown in varying levels in many epithelial tumors (3). Few nonmalignant tissues, such as epithelial cells in the kidney and placenta, show FR expression, as most cells use the reduced folate carrier for folate transport (4). For some tumors, such as ovarian cancer, FR expression is associated with tumor stage and grade and is a negative prognostic factor (5,6). FRs are involved in tumor progression in various ways. First, the fact that FRs transport folate into cells appears to support proliferation of malignant cells (7). Second, FR expression was found to be associated with chemotherapy resistance in ovarian cancer, potentially by mediating apoptosis resistance (6). Third, FR expression seems to support cell motility, as its expression in ovarian cancer is associated with downregulated E-cadherin expression (7).
Targeting of FR is an attractive anticancer treatment with limited toxicity. Different treatments targeting the FR have been developed, such as farletuzumab, vintafolide, EC1456 (a folate-tubulysin conjugate in phase 1 trials), and IMGN853 (an anti-FR antibody-maytansinoid conjugate in phase 1 trials) (8). Farletuzumab and vintafolide have shown clinical promise in phase 2 and 3 trials (3,9). Farletuzumab is an FRα-specific monoclonal antibody that can induce cell death through complement-dependent cytotoxicity and antibody-dependent cell-mediated cytotoxicity (9). Vintafolide can deliver chemotherapy to FR-expressing cells, as it is a conjugate of folate and the chemotherapeutic agent desacetylvinblastine monohydrazide (3).
Because activated macrophages express FRβ, targeting FR may also be effective in treatment of inflammatory diseases, such as rheumatoid arthritis and osteoarthritis (8,10).
FR EXPRESSION ASSESSMENT
Assessing tumor FR expression can be both a prognostic and a diagnostic tool. Several methods have been used for FR detection, such as immunohistochemistry, polymerase chain reaction, quantitation polymerase chain reaction, or in situ hybridization (5,6). Although these methods can have high specificity and sensitivity, their clinical use requires a biopsy, typically taken only once of a single lesion. This gives an incomplete picture, as FR expression can be heterogeneous (11,12).
This cellular heterogeneity can occur between the primary lesion and distant metastases and during tumor evolution due to therapeutic resistance (12), thus creating a challenge to providing an accurate assessment of the patient’s FR status. Whole-body imaging using FR-radiolabeled conjugates can address this challenge by allowing noninvasive assessment of FR expression for multiple lesions and at different times (3,4,13). Additionally, FR imaging using radiolabeled conjugates leads to visualization of all functional FRs and not only FRα, a fact that is important because FR-targeted treatments need to be actively transported into the cell by functional FRs (of any isoform) (11).
Early studies of radiolabeled FRα-specific antibody MOv18 demonstrated ability to visualize FR expression in pelvic tumors (14). More recent studies have focused on the radiolabeled conjugates 111In-DTPA-folate (15) and 99mTc-etarfolatide (11).
99MTC-ETARFOLATIDE CHARACTERISTICS
99mTc-etarfolatide takes advantage of the more optimal SPECT imaging characteristics of technetium (half-life of 6 h and 140-keV photon) and has been evaluated in several clinical trials (1,3,11,13,16).
Preclinical studies showed that, compared with unmodified folate, 99mTc-etarfolatide has an affinity value for human FRs of 0.92 and a 3.2 nM dissociation constant, making 99mTc-etarfolatide suitable to visualize FR expression with high selectivity (17,18). The radiation dosimetry estimates of 99mTc-etarfolatide are similar to those of other 99mTc agents (average effective dose, 0.011 mSv/MBq), with the highest estimated doses being to the kidneys and urinary bladder wall (11). A 2-compartment pharmacokinetic model demonstrated rapid urinary and serum clearance, with relatively slow 99mTc-etarfolatide distribution from peripheral tissues into blood (11).
99MTC-ETARFOLATIDE IN CLINICAL TRIALS
99mTc-etarfolatide is being studied as a companion diagnostic imaging agent in multiple vintafolide clinical trials. To date, no safety concerns have been identified and the only 99mTc-etarfolatide–related adverse events were lower abdominal pain, nausea, and vomiting (occurring in <1% of patients) (11). Several phase 2 trials showed that 99mTc-etarfolatide imaging may be able to identify patients who are most likely to benefit from vintafolide (3,13). In a phase 2 trial (NCT00507741) of single-arm vintafolide treatment, heavily pretreated patients with ovarian cancer were categorized as FR(100%) if all evaluated lesions expressed FR (n = 14), FR(10%–90%) if at least one but not all lesions expressed FR (n = 22), and FR(0%) if no lesions expressed FR (n = 3) (13). The disease control rate (complete response + partial response + stable disease) was 57% in FR(100%) patients, compared with 36% and 33% in FR(10%–90%) and FR(0%) patients, respectively. Median overall survival also correlated with FR expression: 14.6 mo in FR(100%) patients, compared with 9.6 mo and 3.0 mo for FR(10%–90%) and FR(0%) patients, respectively (13).
Additionally, a randomized phase 2 trial (PRECEDENT, NCT00722592) confirmed that 99mTc-etarfolatide imaging can identify patients likely to benefit from vintafolide. This trial compared the efficacy of vintafolide combined with pegylated liposomal doxorubicin (PLD; combination arm) with that of PLD alone (control arm) in patients with recurrent platinum-resistant ovarian cancer (3). Median progression-free survival for FR(100)% patients (n = 23) was 5.5 mo in the combination arm and 1.5 mo in the control arm (P = 0.01), compared with 3.8 versus 5.4 mo (P = 0.468) for FR(0%) patients (n = 13) (3). The short progression-free survival of FR(100%) patients treated with PLD alone, compared with that of FR(0%) patients (1.5 mo vs. 5.4 mo, respectively), was suggestive of the potential tumor-promoting effects of FR. Furthermore, this phase 2 trial showed that FR(100%) patients significantly benefited from the addition of vintafolide to PLD treatment. In line with the mechanism of action of vintafolide, the progression-free survival of FR(0%) patients was not significantly altered by combination treatment.
Several studies exploring the potential of 99mTc-etarfolatide to assess FR2 expression are ongoing: a phase 3 trial (PROCEED, NCT01170650) in patients with 99mTc-etarfolatide–positive platinum-resistant ovarian cancer treated with vintafolide combined with PLD versus PLD alone; a randomized phase 2 trial (TARGET, NCT01577654) in patients with 99mTc-etarfolatide–positive lung cancer treated with vintafolide combined with docetaxel versus docetaxel alone versus vintafolide alone; and a phase 1 study (NCT01688791) in 99mTc-etarfolatide–positive patients with solid tumors for whom standard therapy has failed, assessing the maximum tolerated dose of vintafolide in combination with paclitaxel and carboplatin.
99MTC-ETARFOLATIDE IMAGING
Although early clinical trials have suggested that 99mTc-etarfolatide imaging can be used to select patients who are likely to respond to vintafolide therapy, there are both physiologic and technical factors that can affect imaging results and interpretation.
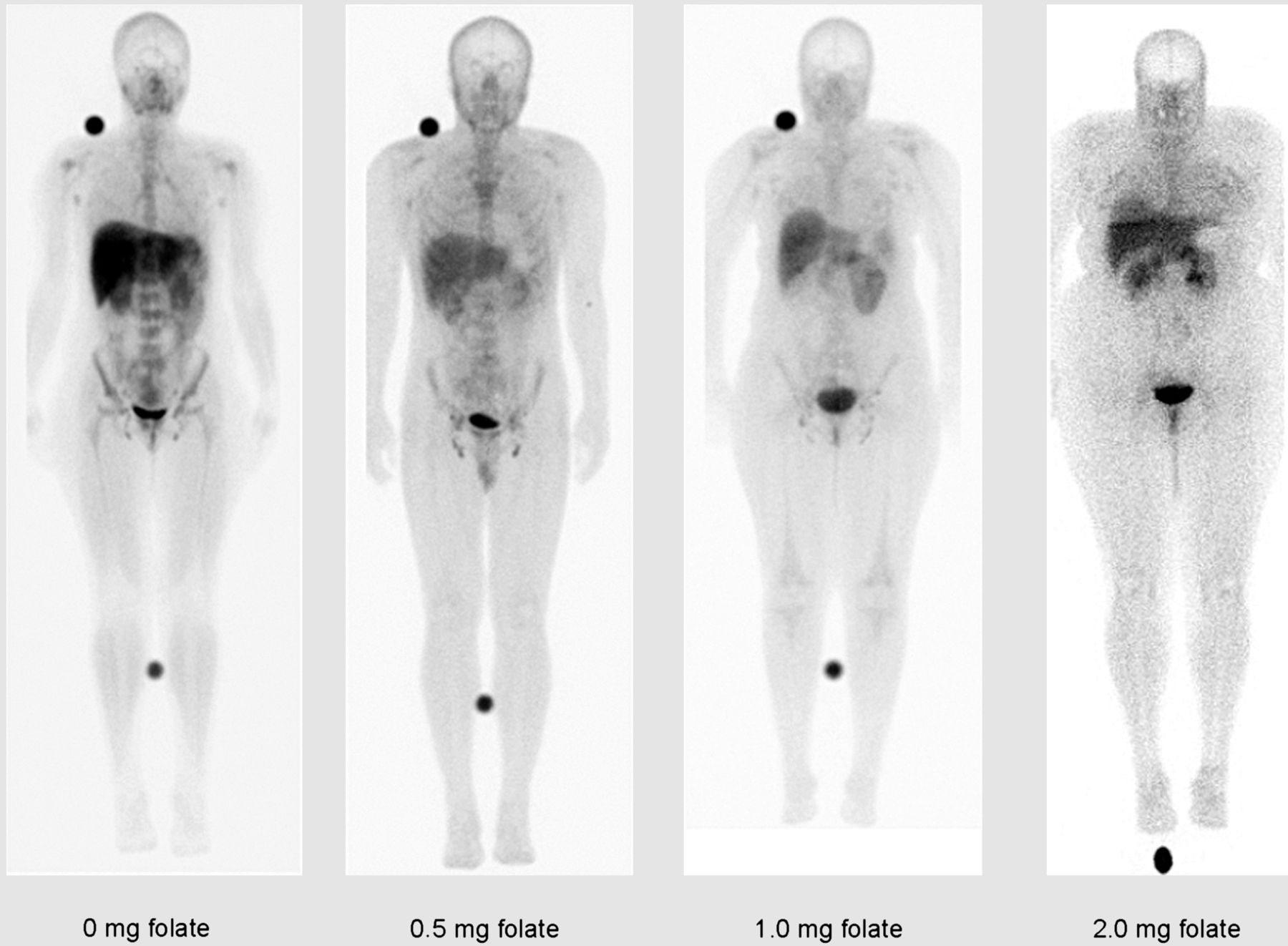
First, FR expression and 99mTc-etarfolatide physiologic uptake, which occurs in liver, kidneys, spleen, bladder, and, to a lesser extent, bone marrow, may complicate interpretation of FR expression in lesions close to these organs (11) (Fig. 1). To partially saturate FRs, and to reduce 99mTc-etarfolatide uptake in these organs, a small amount of folic acid is injected before 99mTc-etarfolatide administration.
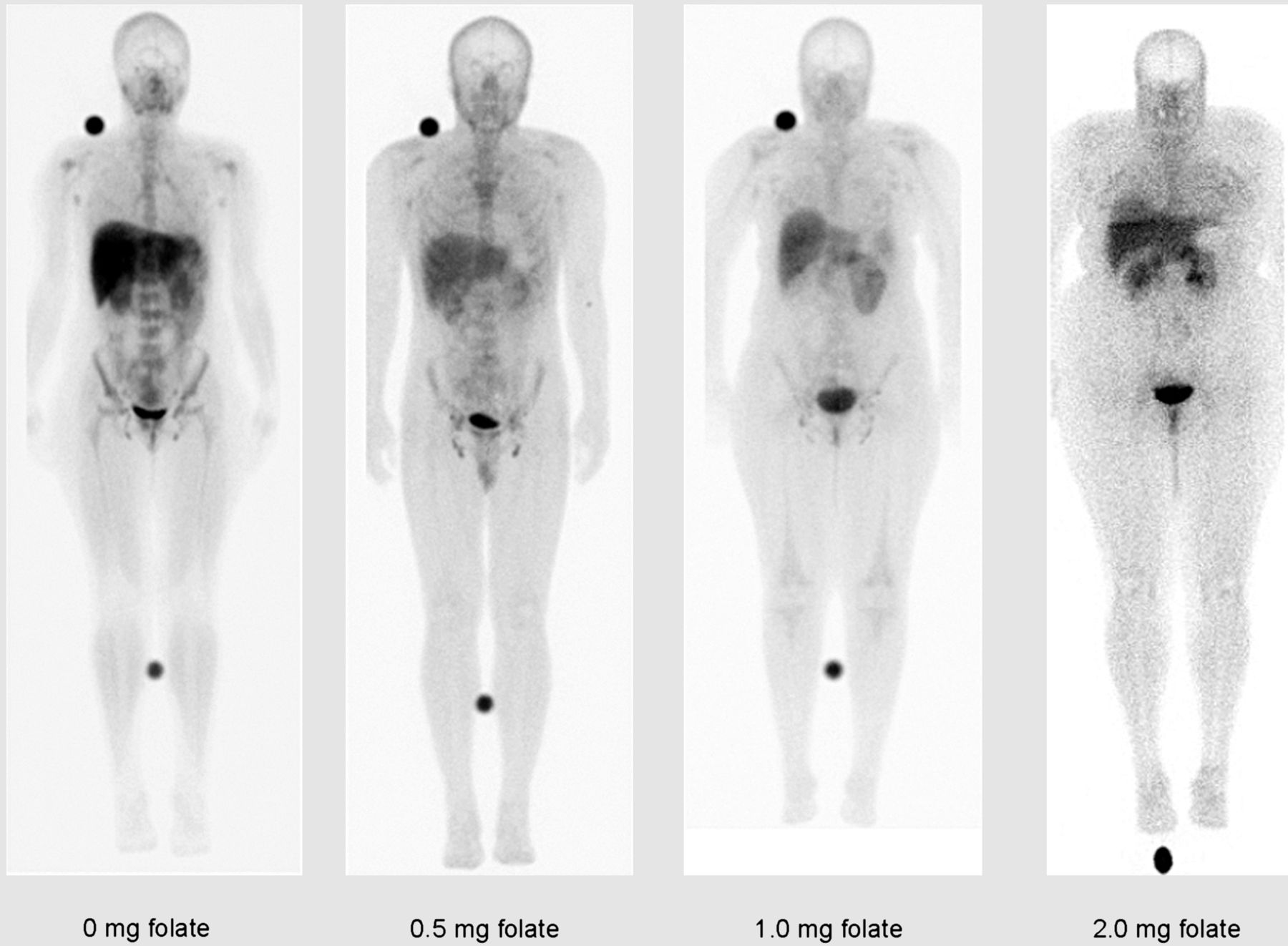
99mTc-etarfolatide biodistribution pattern (1 h after injection) after folate preinjection in healthy volunteers. In absence of folate preinjection, 99mTc-etarfolatide uptake is seen in liver, kidney, spleen, bladder, and bone marrow. This background organ activity is decreased with preinjected folate.
Because activated macrophages express FRβ and show uptake of 99mTc-etarfolatide, areas of infection or inflammation may falsely appear as FR-positive malignant lesions (8,19) (Fig. 2). Another FR-imaging agent, a conjugate of a reduced and alkylated form of folic acid (N5, N10-dimethyltetrahydrofolic acid) and 99mTc (2,5-dimethoxytetrahydrofuran-99mTc), has been found to more specially bind to FRα, which is often expressed on malignant cells, and less to FRβ, often expressed by peripheral blood monocytes or inflammatory macrophages (20).
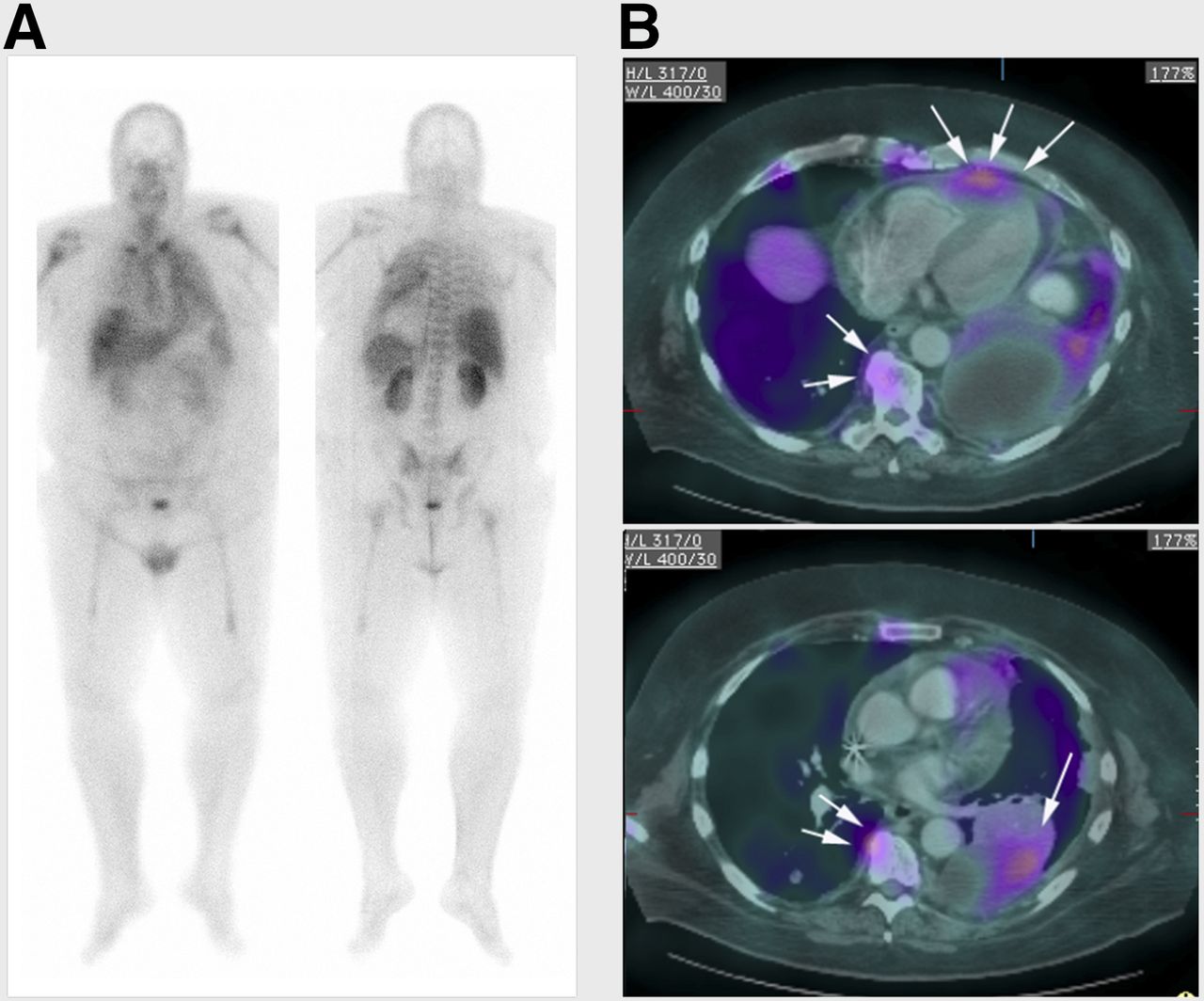
(A) Whole-body planar images obtained approximately 1 h after 99mTc-etarfolatide administration in lung cancer patient. (B) 99mTc-etarfolatide SPECT images were manually fused to patient’s prior CT images. SPECT/CT transaxial fusion images delineate tumor in left lower lobe (single arrow), with diffuse pleural spread of tumor and pericardial metastasis (triple arrows). 99mTc-etarfolatide uptake in inflammatory lesions such as benign osteophytes can be seen (double arrows).
The early imaging studies with 99mTc-etarfolatide used separate SPECT and CT images with only either visual side-by-side comparison or manual SPECT/CT fusion, because hybrid SPECT/CT cameras were not available. This technical limitation of using 2 noncontemporaneous studies may have limited these early studies. Integrated SPECT/CT cameras are becoming more prevalent. SPECT/CT fusion imaging should improve spatial localization and determination of FR-positive or -negative lesions (Figs. 2 and 3).
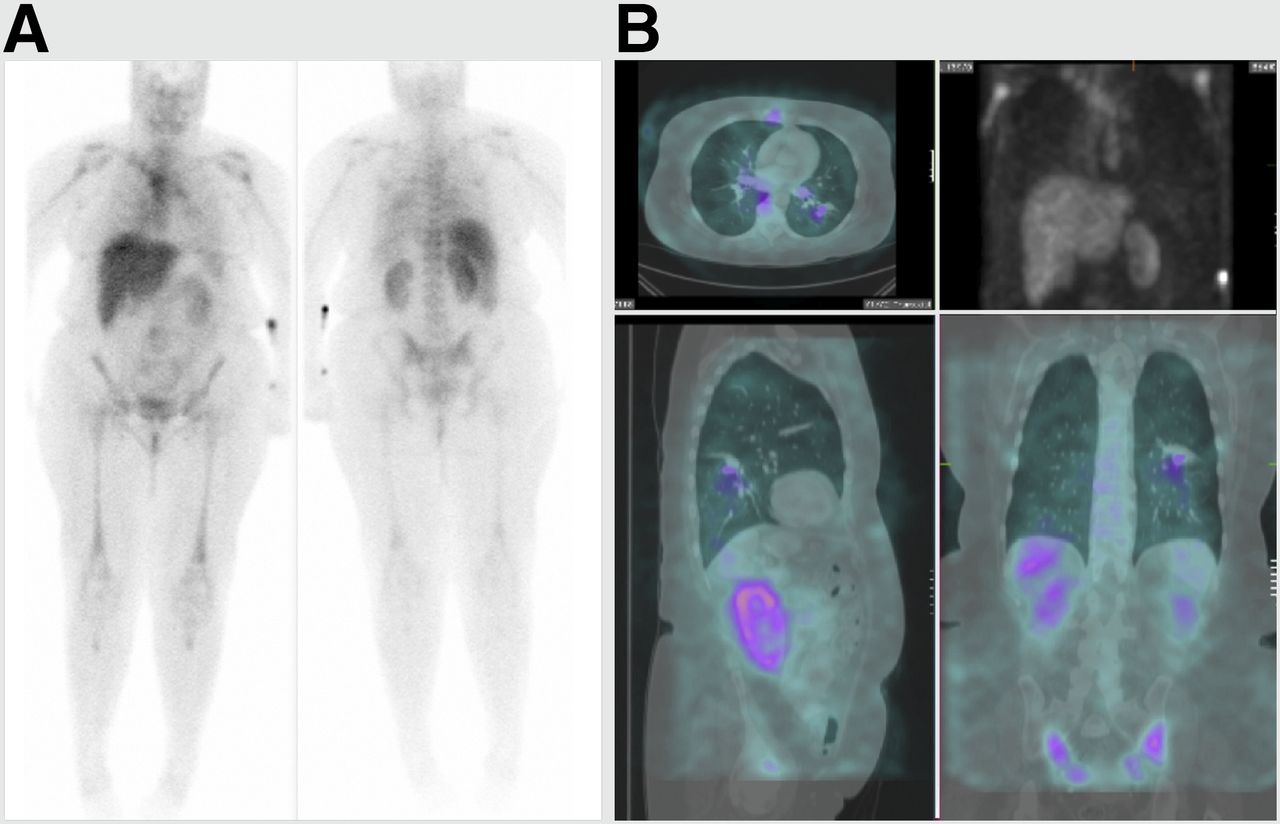
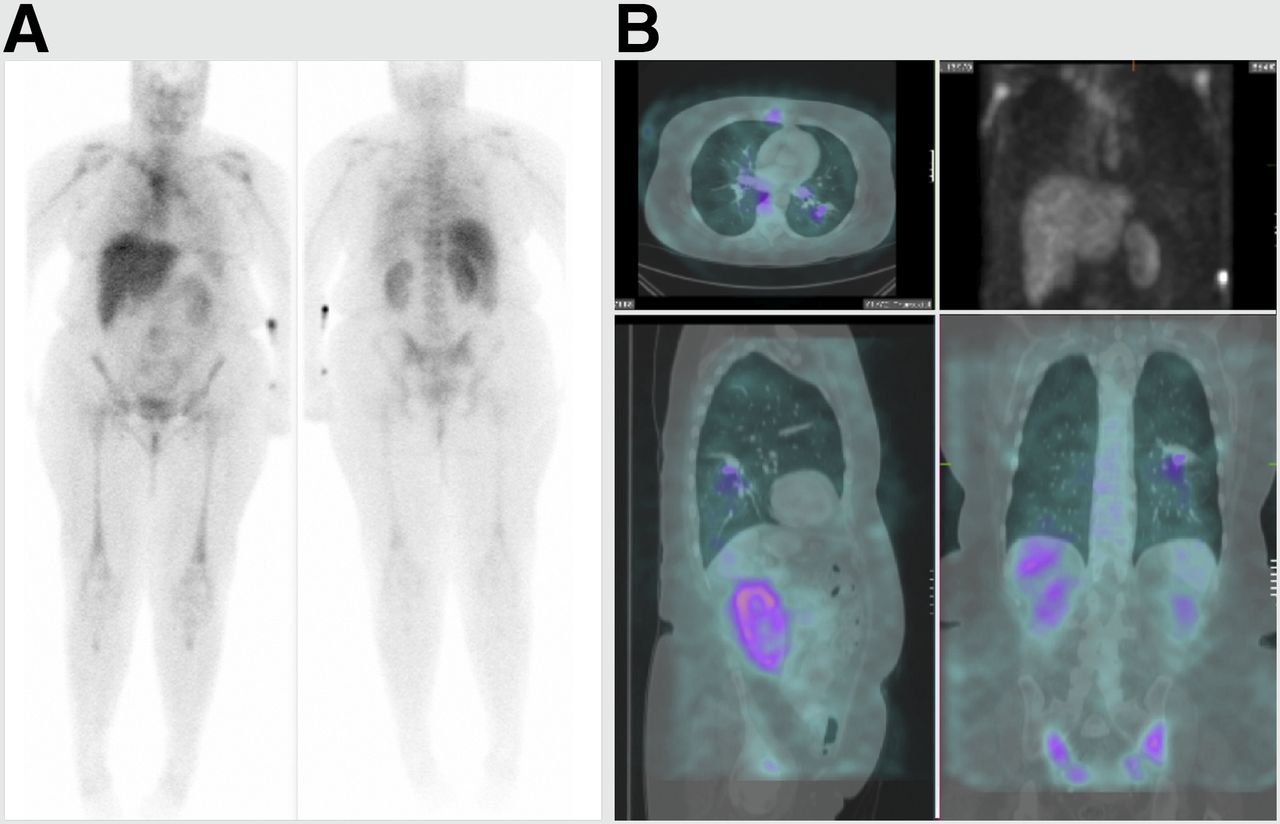
(A) Whole-body planar 99mTc-etarfolatide study for known pulmonary nodule obtained approximately 1 h after 99mTc-etarfolatide administration. As with other imaging agents, planar 2-dimensional imaging lacks image contrast and sensitivity for detecting 99mTc-etarfolatide binding to small pulmonary nodule in left lower lobe. (B) 99mTc-etarfolatide SPECT images with maximum intensity projection (upper right), transaxial (upper left), sagittal (lower left), and coronal (lower right) were manually fused to patient’s prior CT images, allowing for better anatomic localization and confirmation of FR binding to pulmonary nodule in this biopsy-proven non–small cell lung cancer.
At present, limited data exist on the correlation between FR expression as assessed by immunohistochemistry and 99mTc-etarfolatide uptake. One study showed a 61% agreement between methods (κ coefficient, 0.096; 95% confidence interval, –0.085 to 0.277) (11). The agreement was 72% for positive results and 38% for negative results (99mTc-etarfolatide–positive/–negative patients who are also FR immunohistochemistry–positive/–negative). These poor agreement scores could be related to tumor heterogeneity of FR expression, as immunohistochemistry analysis of primary tumors was compared with imaging of metastases (11). In addition, the immunohistochemistry did not identify FRβ, whereas 99mTc-etarfolatide imaging does.
PET FR IMAGING
Folate can be labeled with 18F (21–25). To date, 18F-fluorodeoxyglucose-folate and 3′-aza-2′-18F-fluorofolic acid seem the most promising PET FR imaging agents. Both have shown good tumor visualization, with limited accumulation in nonmalignant tissues (24,25). 68Ga-labeled radiofolates are also of interest because of their favorable biodistribution profile and 1-step radiolabeling (26,27). However, the short physical half-life of 68Ga (68 min) limits the time window for imaging compared with 18F (110 min) (21). Although there are promising preclinical results, clinical studies of PET folate imaging agents are needed for their further development.
POTENTIAL FUTURE APPLICATION OF 99MTC-ETARFOLATIDE IMAGING
99mTc-etarfolatide imaging may have other clinical applications. Because FR expression is prognostic for ovarian and lung cancer, 99mTc-etarfolatide imaging may be used as a prognostic tool (6,28). Intraoperative FR imaging with optical probes can improve staging and facilitates cytoreductive surgery (29). 99mTc-etarfolatide imaging may aid in selecting patients for intraoperative fluorescence FR imaging and help to identify deep-seated lesions that could be missed by intraoperative optical imaging because of limited signal penetration.
Preclinical studies have demonstrated that 99mTc-etarfolatide imaging can be used to visualize macrophage activation in atherosclerotic plaques and arthritis and to assess disease activity (30–32). One clinical study showed that 99mTc-etarfolatide imaging may be more sensitive than physical examination for assessing disease activity in rheumatoid arthritis patients (33). Other FR-imaging agents have potential to visualize macrophage activation in osteoarthritis and atherosclerosis (34,35).
CONCLUSION
99mTc-etarfolatide imaging has been shown to be valuable for selecting patients who may benefit from FR-targeted treatments. 99mTc-etarfolatide imaging may potentially also be useful for tumor staging or restaging, prognosis assessment, selection of patients for intraoperative fluorescence FR imaging, and assessment of inflammatory disease activity such as rheumatoid arthritis and osteoarthritis.
DISCLOSURE
Editorial and medical writing assistance (by Anna Hooijkaas, PhD, TRM Oncology, The Hague, The Netherlands) was funded by Endocyte Inc. Alan Maurer is a consultant and on the advisory board for Endocyte Inc. Philip Elsinga is a consultant for MSD. Stefano Fanti is on the advisory board for Endocyte Inc. Binh Nguyen is an employee of Endocyte Inc. Wim Oyen is a consultant for MSD and on the advisory board for Endocyte Inc. Wolfgang Weber is on the advisory boards for Endocyte Inc. and MSD. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 14, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 13, 2014.
- Accepted for publication March 17, 2014.





{kind=link}
{kind=link}
{kind=link}