


Abstract
Merkel cell carcinoma (MCC) is a rare but aggressive skin cancer with limited evidence on the role of PET scanning. The primary aim of this study was to assess the impact of 18F-FDG PET in the staging and management of MCC. Methods: A single-institution review using clinical outcome data collected until February 2012 was performed of patients with MCC who underwent staging PET scanning between January 1997 and October 2010. Management plans were recorded prospectively at the time of the PET request, and follow-up outcomes were recorded retrospectively. The clinical impact of PET was scored using our previously published criteria: “high” if the PET scan changed the primary treatment modality or intent; “medium” if the treatment modality was unchanged but the radiation therapy technique or dose was altered. The primary objective was to test the hypothesis that the true proportion of patients who have a high- or medium-impact scan would be greater than 25%. Results: The median follow-up of 102 consecutive patients was 4.8 y. The results of staging PET had an impact on patient management in 37% of patients (P < 0.003). High- and medium-impact scans were recorded for 22% and 15% of patients, respectively. PET staging results differed from conventional staging results in 22% of patients, with PET upstaging 17% and downstaging 5%. The 3- and 5-y overall survival was 60% (95% confidence interval, 50%–71%) and 51% (95% confidence interval, 41%–64%), respectively. In stratification by PET-defined stage, the 5-y overall survival was 67% for patients with stage I/II disease but only 31% for patients with stage III disease (log-rank P < 0.001). The 5-y cumulative incidence of locoregional failure, distant failure, and death was 16.6%, 22.3% and 14.3%, respectively. On multivariate analysis, only PET stage (P < 0.001) and primary treatment modality (P = 0.050) were significantly associated with overall survival. The primary treatment modality was not associated with progression-free survival when stratification was by tumor stage. Conclusion: The use of 18F-FDG PET scans had a great impact on patients and may play an important role in the prognostic stratification and treatment of this disease.
Merkel cell carcinoma (MCC) was first described in 1972 (1). It is an aggressive skin carcinoma with a predisposition for local recurrence and carries a high risk of both nodal and distant metastases. Although rare, MCC is increasing in reported incidence, at least in part because of improved pathologic diagnosis. In the United States, the incidence of MCC increased 3-fold from 0.15 cases per 100,000 in 1986 to 0.44 cases per 100,000 in 2001 (2). Optimal management is difficult to define, given the relative rarity of the disease. Treatment recommendations have been based largely on single-institution observational studies. Historically, surgery has been the mainstay of treatment, but resection has been associated with high rates of locoregional failure if not followed by postoperative radiation therapy (RT) (3–6). Irrespective of the modalities of treatment utilized, patient outcomes are generally poor, with the presence of nodal disease being the most powerful predictor of survival (4).
PET with 18F-FDG is a promising functional imaging modality for the evaluation of MCC. Most of the existing publications on PET in MCC were on series that included few patients (7–10). At the time we designed the current study, the largest previously published series reporting the use 18F-FDG PET in MCC was from Sydney, Australia, on 18 patients, of whom 12 underwent staging PET scans. The authors reported a change in management in 9 of these patients. Because of the promising nature of these early reports, our group performed a retrospective analysis of our experience to evaluate the role of PET in MCC and its ability to stratify prognosis. Since completion of our analysis, a retrospective study from the Dana-Farber/Brigham and Women’s Cancer Center reported results on 61 patients undergoing staging scans, of whom 18F-FDG PET/CT upstaged 16% (11). That study did not assess patient survival outcomes.
The Peter MacCallum Cancer Centre has over 15 y of experience in performing 18F-FDG PET scanning for MCC. Institutional policy is to refer patients with MCC for 18F-FDG PET staging only when treatment with curative intent is considered. The primary aim of this study was to assess the incremental benefit of PET staging over conventional staging in the initial management of MCC patients for whom curative therapy was planned. We studied the impact of PET on patient management and investigated the prognostic value of PET stage and pretreatment factors on survival and patterns of failure.
MATERIALS AND METHODS
This study was approved by an independent review board to assess all patients treated at the Peter MacCallum Cancer Centre between January 1997 and October 2010. Over this interval there was a progressive evolution in the technology, with initial studies being performed on a stand-alone PET scanner (Quest; GE Healthcare). Since 2002, a range of PET/CT scanners has been used, including a Discovery LS (2002–2008; GE Healthcare), Discovery STE (2006 to the present; GE Healthcare), Discovery 690 (2011 to the present; GE Healthcare), and Biograph 64/40 (2009 to the present; Siemens Medical Solutions). All scanners were maintained and calibrated to manufacturer specifications. All PET data were reconstructed using 3-dimensional ordered-subset expectation maximization. Table 1 summarizes the acquisition methodology. The study inclusion criteria required that all patients have histologic confirmation of MCC and underwent adequate conventional staging investigations in addition to a staging 18F-FDG PET scan. Adequate staging was defined as at least a physical examination, chest imaging with radiography or CT, and CT of the locoregional nodal stations. Management plans before and after the staging 18F-FDG PET scan were recorded prospectively at the time of the PET request as part of an institutionwide prospective observational study. All other clinical parameters were recorded retrospectively up to February 2012. The impact of PET was assessed according to previously published institutional criteria (12). A “high-impact” result was defined as a change of treatment modality (e.g., surgery to RT) or a change of intent (e.g., curative to palliative). A “medium-impact” result was defined as no change in the treatment modality but alteration of the RT planning technique or dose. A “low-impact” result was defined as no change in treatment modality, technique, or intent.
PET Acquisition Methodology
The standardized uptake values (SUVs) of metabolically avid disease on the staging 18F-FDG PET scans were calculated by a single observer and independently verified by a second observer. A semiautomatic autocontouring process using an SUV threshold of 2.5 was applied to define the volume of interest and adjusted as appropriate to adequately cover the 18F-FDG–avid lesion. The maximum SUV (SUVmax), mean SUV (SUVmean), metabolic volume, and percentage injected dose were measured for each patient using the most metabolically active lesion on 18F-FDG PET (either local, nodal, or distant). All parameters were referenced to the background metabolic liver activity and a region of healthy normal tissue to control for any errors in SUV attributes or camera calibration factors. Any scans with incorrect calibration parameters were discarded from the analysis.
The primary study hypothesis was that in patients undergoing a staging 18F-FDG PET scan, the true proportion of scans that have a high impact would be greater than 10%, and medium- or high-impact scans would be greater than 25%. These thresholds were selected as values that were considered to be clinically relevant. The secondary study objectives were to characterize pretreatment prognostic factors, including PET stage and SUV, and determine their relationship with patterns of failure (locoregional and distant), progression-free survival (PFS), and overall survival (OS).
Treatment Policy
During the study period, both surgery and RT (with or without concurrent chemotherapy) were considered acceptable definitive management strategies. When RT was used, the typically prescribed dose was 50 Gy in 25 fractions (or equivalent), to a generous margin (3–5 cm) around the primary disease site. The draining lymph nodes were treated in continuity with the primary site, provided the nodes were within 20 cm of the primary. In patients receiving chemotherapy in addition to RT, carboplatin and etoposide were administered during weeks 1 and 4 of RT and then again 2 and 5 wk after RT was completed (weeks 7 and 10).
Statistical Methods
The time until events was measured from the staging 18F-FDG PET scan. For the primary objective, the null hypothesis of a true high impact rate of 10% or less and a medium or high impact rate of 25% or less was tested against the 2-sided alternative assuming a binomial distribution (t test). The Kaplan–Meier product limit method was used to characterize the OS and PFS rates and their respective 95% confidence intervals (CIs). The log-rank test was used to evaluate the impact of potential prognostic factors on survival outcomes, and a univariate Cox proportional hazards model was used to estimate the hazard ratios. The presence of a positive resection margin, the size of the primary, the conventional stage, the PET-defined stage, nodal involvement, the primary treatment modality, the presence of residual metabolic disease, the presence of lymphovascular invasion, and the primary site were used as candidate explanatory variables. A multifactor Cox proportional hazards model was built using backward elimination for OS as the response event. Nonsignificant explanatory variables were eliminated from the model with a significance level of 0.05. The models were subsequently repeated to test for an association with progression-free survival. The association between SUVmax and SUVmean and survival was tested for the subset of patients with metabolically apparent disease at the time of 18F-FDG PET.
RESULTS
The study included 102 evaluable patients who had staging 18F-FDG PET scans. The median follow-up time was 4.8 y. Patient characteristics are described in Table 2. Histopathologic reports were recoverable for 89 of the 102 patients. Perineural invasion was not described for any patient, but lymphovascular space invasion was reported for 19. Stand-alone PET was used in 21 patients, and hybrid PET/CT was used in 81. In patients receiving RT as part of their definitive management (n = 72), the biological effective doses (as described by Fowler et al. (13)) were similar, with a median, mean, and interquartile range of 60 Gy, 59 Gy, and 59.5–60 Gy, respectively.
Patient Characteristics
Impact of Staging 18F-FDG PET Scans
The impact of 18F-FDG PET over conventional staging is tabulated in Table 3. The proportion of high-impact PET scans was significantly greater than 10% (P < 0.001), and the proportion of medium- or high-impact scans was significantly greater than 25% (P < 0.003).
Impact of Staging PET Scan
In total, staging 18F-FDG PET resulted in a change in the management plan for 37% of patients. Of the 23 PET scans that had a high impact on the management of patients, 14 (62%) resulted in a change in treatment modality, 5 (21%) in a change in treatment intent, and 4 (17%) in a change in both treatment modality and RT technique. Of the 5 patients for whom the treatment intent changed, 4 were upstaged because of distant metastases and were treated with palliative intent, whereas 1 was downstaged from suspected but unproven distant metastatic disease and treated with curative intent.
Incongruent staging findings between conventional and PET investigations were found for 22 patients, with PET upstaging 17 patients and downstaging 5 patients. Of the 17 patients who were upstaged because of the PET scanning, 4 (24%) were upstaged because occult distant metastatic disease (stage IV) was found and 13 (76%) because occult nodal disease (stage III) was found. Of the 5 patients who were downstaged because of PET scanning, 2 were downstaged from suspected stage IV and 3 were downstaged from stage III.
Survival Outcomes
Of the 102 patients with staging PET, 4 patients who had PET-defined stage IV disease were treated with purely palliative intent and were excluded from the survival analysis. A further patient received chemotherapy only, without definitive surgery or RT, and was also excluded, resulting in a total of 97 eligible patients for the OS and PFS analysis.
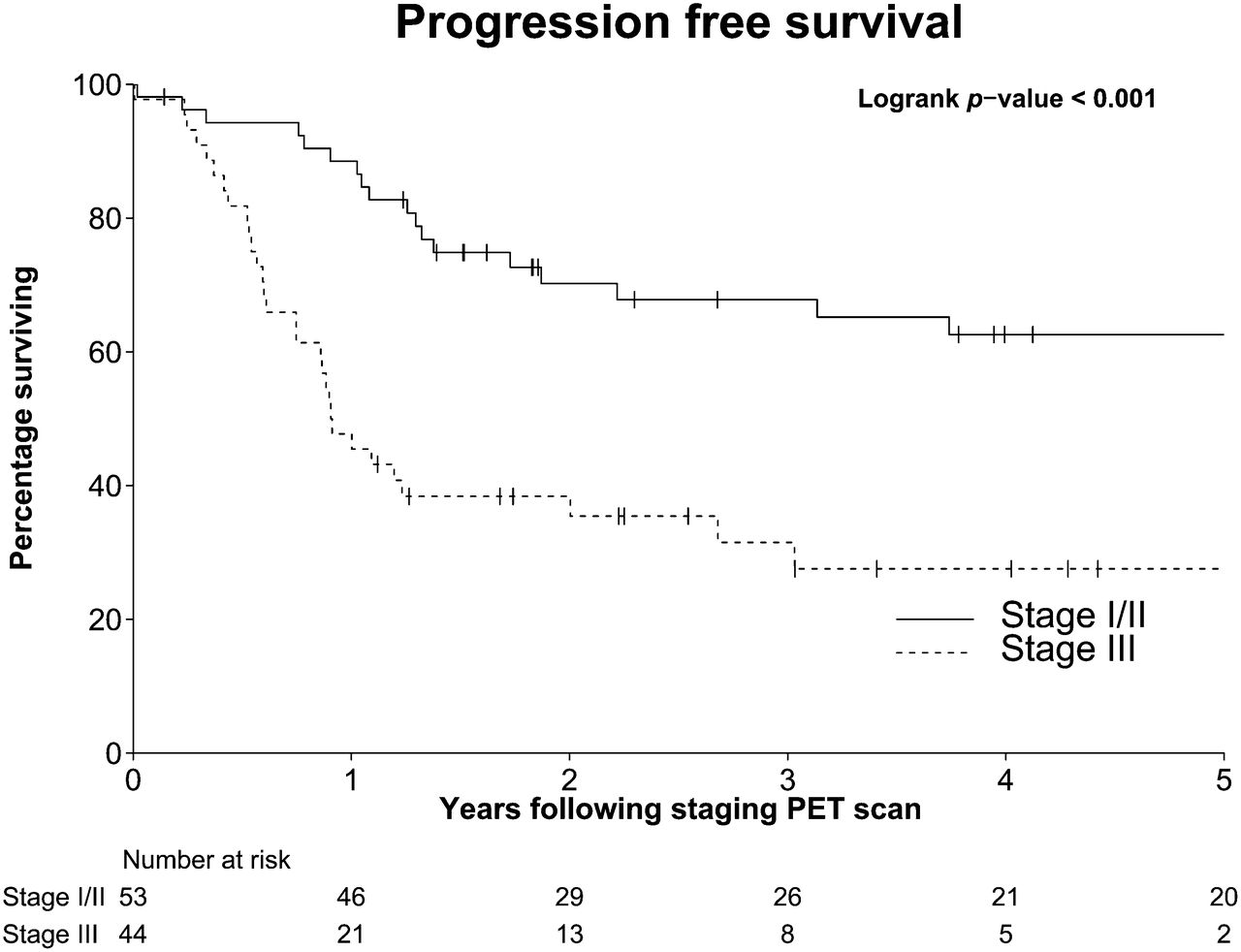
OS was 60% at 3 y (95% CI, 50%–71%) and 51% at 5 y (95% CI, 41%–64%). When categorized by the PET-defined stage according to the American Joint Committee on Cancer, OS at 3 y was 78% (95% CI, 67%–91%) for stage I/II and 37% (95% CI, 23%–57%) for stage III. OS at 5 y was 67% (95% CI, 54%–83%) for stage I/II and 31% (95% CI, 18%–54%) for stage III (Fig. 1). OS grouped according to staging concordance between conventional and PET imaging is displayed in Figure 2. The 13 patients with discordant staging investigations due to upstaging to stage III disease on PET had a survival that closely approximated patients who had stage III disease concordantly on both PET and conventional imaging.
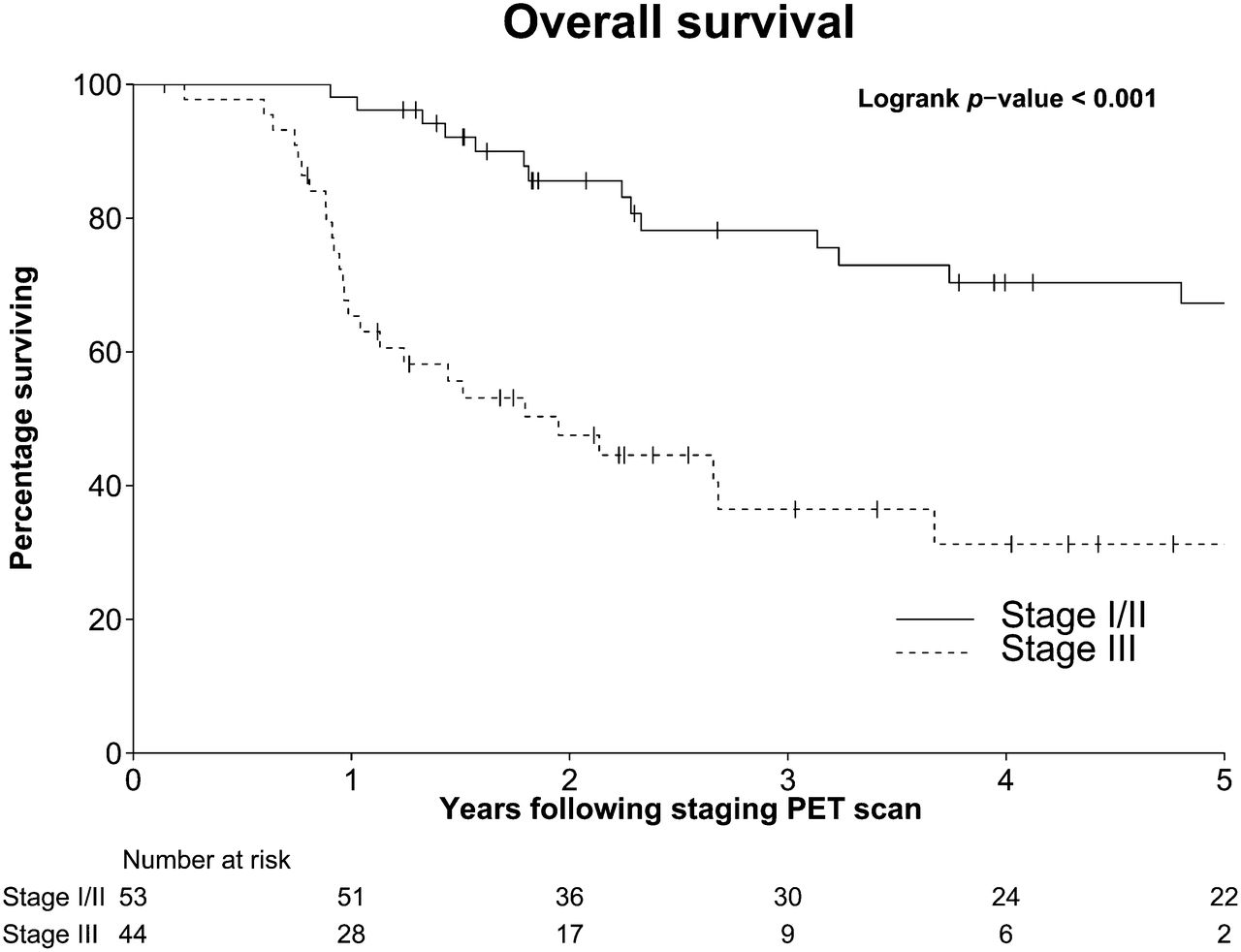
OS according to PET-defined stage.
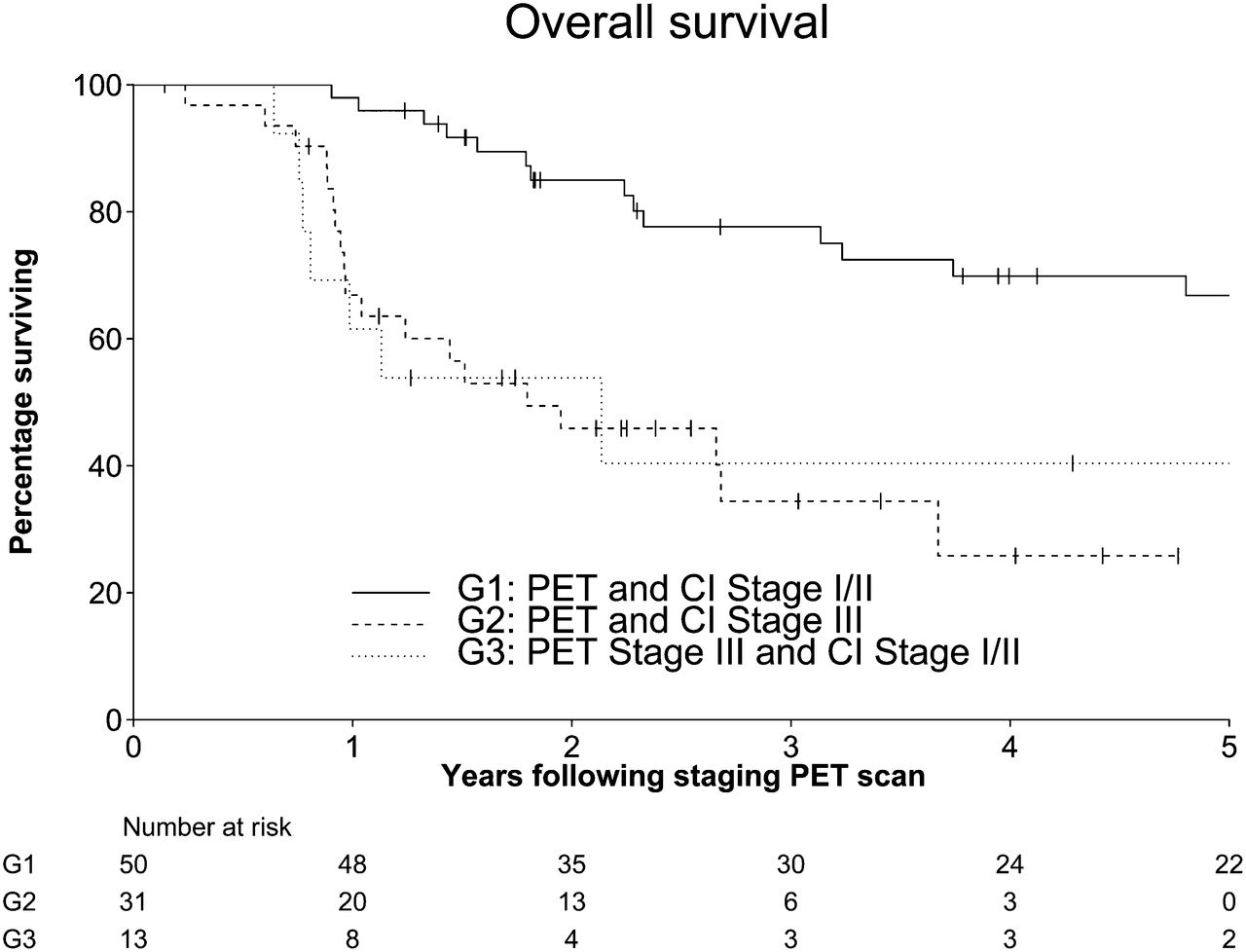
OS grouped by concordance/discordance between PET-based stage and conventional imaging (CI)–based stage.
PFS was 51% at 3 y (95% CI, 42%–63%) and 47% at 5 y (95% CI, 37%–59%). After initial treatment, 37 patients (38%) relapsed. Of these, the first site of failure was distant in 21 patients, whereas 17 patients first relapsed locally or within regional nodal stations. The cumulative incidences of locoregional failure, distant failure, and death at 3 y were 15.1%, 22.3%, and 11.2%, respectively. At 5 y, the corresponding figures were 16.6%, 22.3%, and 14.3%, respectively. When categorized by the PET-defined stage according to the American Joint Committee on Cancer, PFS at 3 y was 68% (95% CI, 56%–82%) for stage I/II and 32% (95% CI, 20%–50%) for stage III. The corresponding PFS at 5 y was 63% (95% CI, 50%–78%) for stage I/II and 28% (95% CI, 16%–47%) for stage III (Fig. 3).
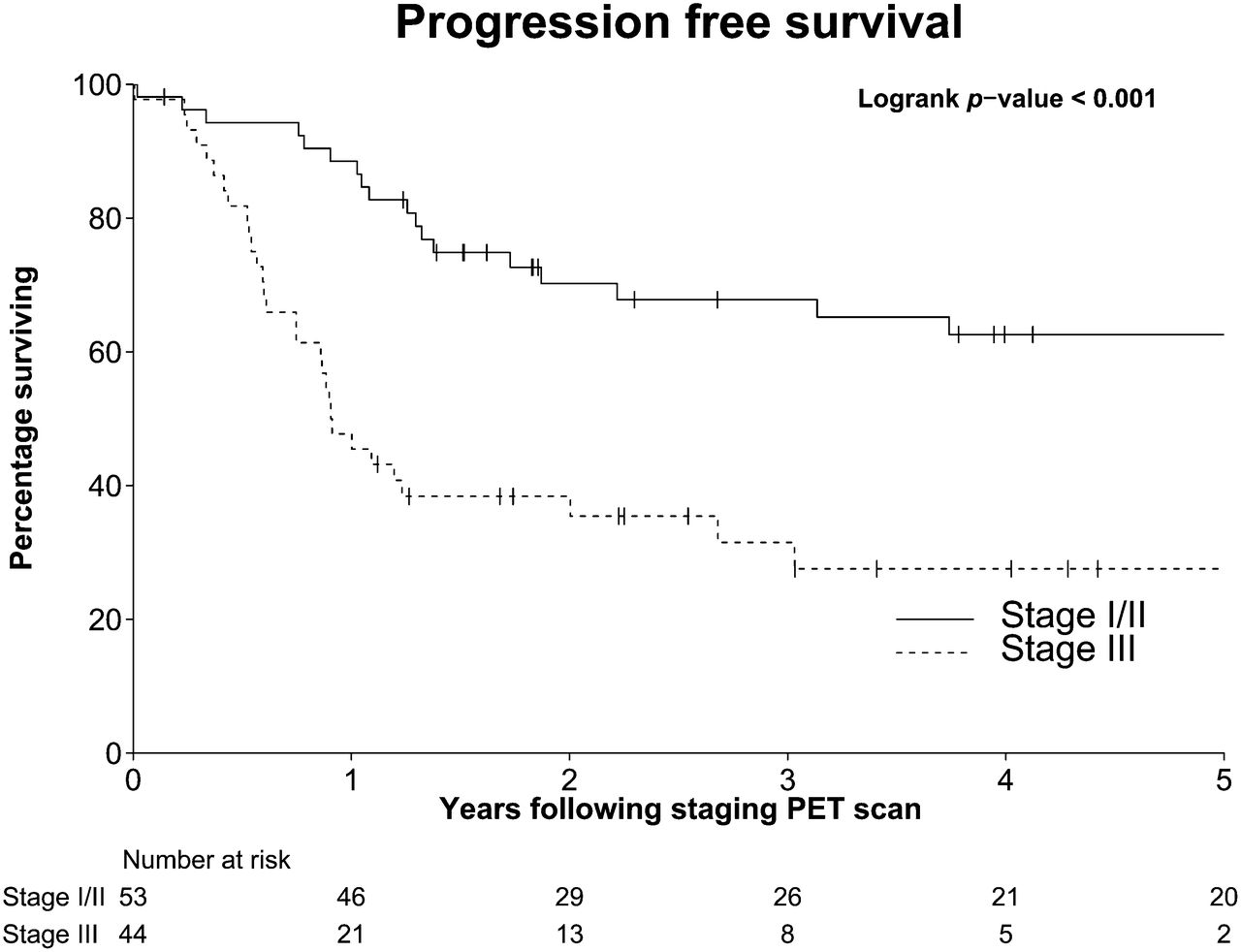
PFS according to PET-defined stage.
Prognostic Factors for Survival
The 5-y OS was 39% (95% CI, 23%–66%) for patients receiving surgery alone and 42% (95% CI, 25%–70%) for RT or chemoradiation therapy alone. The 5-y OS for the combination of surgery and adjuvant RT or chemoradiation therapy was 64% (95% CI, 50%–83%). A univariate Cox regression analysis was performed using pretreatment prognostic factors known and postulated to be prognostic for OS and PFS (Table 4). The size of the primary, the presence of nodal involvement on PET, the primary treatment modality, and the presence of any apparent metabolically active disease on PET were all statistically significantly associated with both OS and PFS. Lymphovascular space invasion was associated with OS (P = 0.015) but not with PFS (P = 0.079). Neither the presence of a positive resection margin nor the primary site of disease correlated with either OS or PFS.
Univariate Analysis for OS and PFS
A multifactor Cox regression model was created using the explanatory variables listed in Table 4 with backward elimination. Conventional stage, PET nodes, and presence of residual metabolic disease were not included in the model because of high multicolinearity with PET stage. Only PET stage and primary treatment modality remained statistically significant for OS (Table 5). Patients with stage III disease on PET were at a 3.8 times greater risk for death than were patients with stage I/II disease (HR, 3.8; 95% CI, 1.9–7.8).
Multifactor Cox Regression Analysis for OS
For 31 of the patients who had apparent metabolic disease at the time of staging PET, the original PET data could be recovered for analysis and the liver and normal-tissue background calibration could be verified. The metabolic activity was normally distributed in these patients, with a mean SUVmax of 10.3 (interquartile range, 6.0–13.3) and an SUVmean of 4.8 (3.5–5.6). In these patients, the SUVmax and SUVmean were not statistically associated with OS or PFS (Table 6).
Impact of SUV on OS and PFS in Patients with Gross Metabolic Disease
PFS by Treatment Modality
The primary treatment modality was significantly associated with PFS on the univariate analysis (P = 0.028). However, when stratified for tumor stage, there was no therapeutic advantage for any primary treatment strategy in either stage I/II disease (P = 0.569) or stage III disease (P = 0.133) (Table 7). On multifactor Cox regression, only PET stage was significantly associated with PFS (P = 0.133). Patients with PET stage III disease were at 3.1 times greater risk for death or progression than were patients with stage I/II disease (HR, 3.1; 95% CI, 1.7–5.6)
PFS According to Primary Treatment Modality
DISCUSSION
The Trans-Tasman Radiation Oncology Group 96.07 phase II multiinstitutional study investigated the combination of synchronous carboplatinum chemotherapy with RT in the curative treatment of locally advanced MCC (14) after initial biopsy or resection. In that study, the reported 3-y OS was 76%. By comparison, our series showed a 3-y OS and PFS of 60% and 51%, respectively. Unlike the previous series, 28% of the patients in our series were treated with surgery alone without adjuvant therapies. Additionally, there were no study exclusion criteria for performance status or other comorbidities. Most of our patients relapsed within the first 3 y, with PFS at 5 y only minimally changed from 51% to 47%. Despite having an aggressive form of cutaneous malignancy with a propensity for early relapse, patients in our series had a median survival of 6.8 y from diagnosis. MCC was commonly metastatic to lymph nodes, with a large proportion of our patients (45%) already having nodal disease before definitive treatment of their disease (Fig. 4). Notably, these patients were at 5.5 times greater risk of death (hazard ratio, 5.5; 95% CI, 2.8–10.8) than were patients without nodal disease.
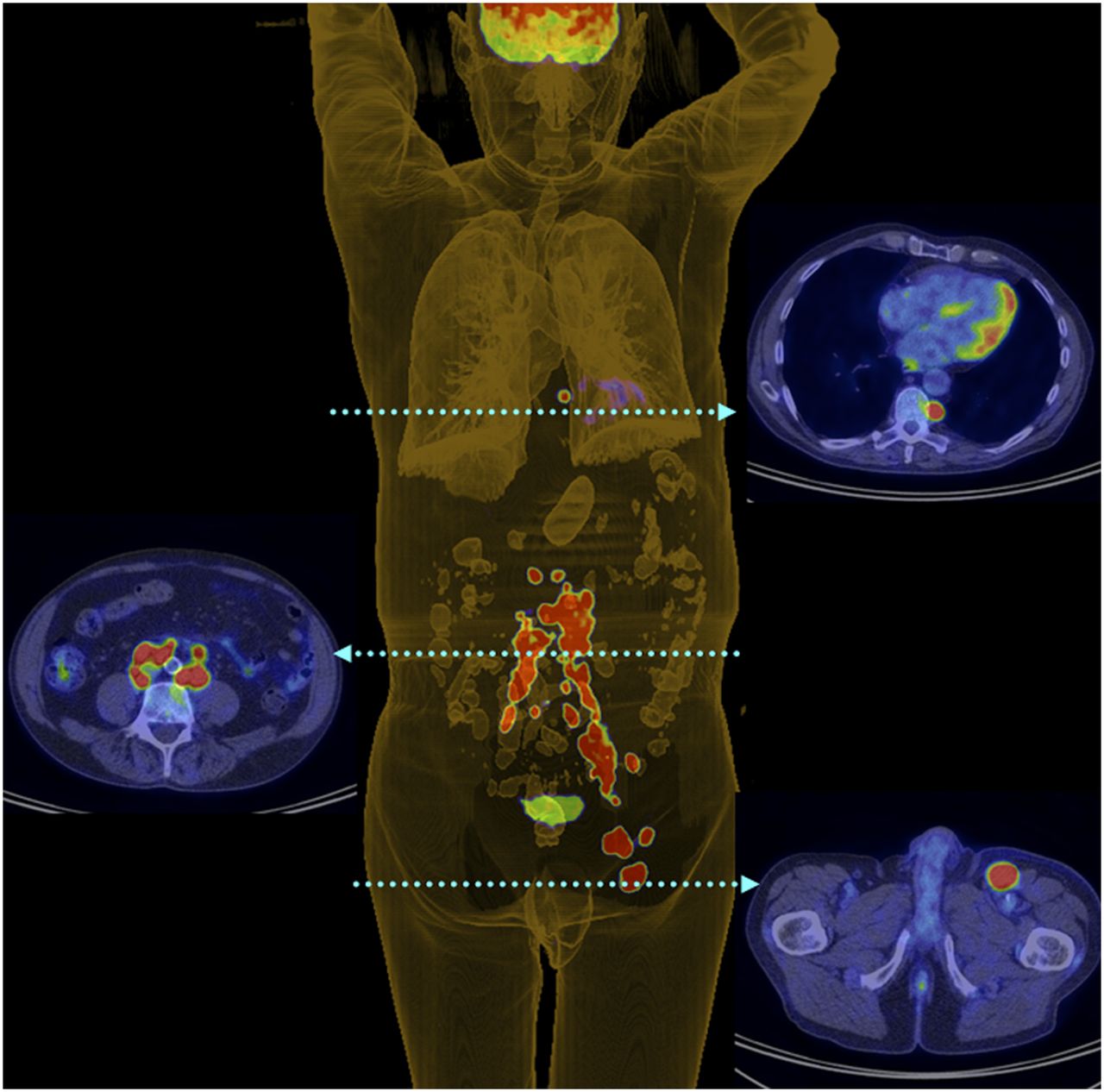
Three-dimensional PET digital reconstruction showing left inguinal nodal and extensive retroperitoneal and thoracic nodal metastases in patient with left-lower-limb MCC.
The use of staging 18F-FDG PET appears to influence the management plans of a significant proportion of patients with MCC. The largest previously reported series on staging 18F-FDG PET was published in 2012 by Hawryluk et al. (15). That series addressed the use of staging PET in 61 patients. The authors reported that PET/CT upstaged 5% (1/22) of stage IIIA patients and upstaged 50% (4/8) of stage IIIB patients, giving an overall upstaging in 16%. In our series, 18F-FDG PET contributed to altered staging in 22 patients (22%) but led to a change in management in 38 patients (37%). By comparison, our institution has previously reported that 18F-FDG PET alters treatment intent or modality of treatment in 34% of patients with non–small cell lung cancer (12) and alters staging and RT technique of head and neck squamous cell cancers (16) in 34% and 29%, respectively. The similarity of results from a single institution across these diseases indicates that the incremental benefit of staging 18F-FDG PET may be as significant in MCC as it is in more common but similarly aggressive cancers.
In our series, MCC proved to be a highly metabolically intense disease, with a mean SUVmax of 10.3 and an SUVmean of 4.9. A similar analysis of 16 patients by Golan et al. (17) reported that the SUVmean of 18F-FDG–avid disease was 4.7 and was in agreement with reports by Igaru et al. (18) and Concannon et al. (11). Hawryluk et al. (15) reported a mean SUVmax of 7.2 in regional and distant metastases. In our patient cohort, increasing metabolic activity was not statistically associated with OS (SUVmax, P = 0.078; SUVmean, P = 0.082). No subgroup of patients had a worse prognosis based on SUV parameters alone. As a consequence of the long period over which cases were acquired, multiple PET scanners were used. Although this factor potentially compromises the reproducibility of semiquantitative measurements, all but 3 of the positive scans used to calculate SUV were done on hybrid PET/CT devices. We believe that the large interpatient variations of tumor metabolism observed would likely far outweigh the relatively minor technical difference between the various scanners. Nevertheless, conclusions drawn from the SUV analysis in isolation should be interpreted with caution.
There is not enough randomized evidence on MCC to support the use of adjuvant therapies after initial surgery. One analysis of the Surveillance, Epidemiology, and End Results database by Mojica et al. (19) suggested an improvement in OS with adjuvant RT after surgery. Surgical intervention was a component of therapy in 89% of the cases (n = 1,487). In that series, 31% of patients had nodal involvement. The median survival for the entire cohort was 49 mo. The median survival for those patients receiving adjuvant RT was 63 mo, compared with 45 mo for those treated with surgery alone. In contrast, in our series 45% of patients had nodal involvement. Despite more advanced disease, the median survival in our series compares favorably at 82 mo. The 5-y OS was 39% for those treated with surgery, 42% for those treated with RT or chemoradiation therapy alone, and 64% for those patients treated with surgery and adjuvant RT or chemoradiation therapy. Consistent with the Surveillance, Epidemiology, and End Results database and previous reports (3–5), our results suggest that surgery should be followed by adjuvant RT or chemoradiation therapy.
The currently active multi-institutional Trans-Tasman Radiation Oncology Group 96.07 study aims to prospectively address the utility of 18F-FDG PET in MCC and is aiming to recruit 50 patients (ClinicalTrials.gov identifier NCT01013779). This important study may provide much-needed prospective evidence to clarify the utility of 18F-FDG PET in this disease. However, given the relatively small sample size of this trial, a definitive conclusion on the utility of this investigation may not be reached. Until the results of this study are available, our study remains the largest and most definitive assessment of the role of 18F-FDG PET in the staging of MCC. Given the range of ongoing evolution of PET technology over the course of this retrospective series, the role of SUV as a prognostic marker remains uncertain and it is possible that the impact may be even higher with current-generation PET/CT scanners with time-of-flight capability and enhanced reconstruction algorithms such as point-spread function.
CONCLUSION
In this study, 18F-FDG PET scans changed the management of 37% of MCC patients and altered the stage of 22%. Our data emphasize the ability of 18F-FDG PET to stratify prognosis with stage, as 18F-FDG PET was the strongest prognostic factor for survival. If these results can be validated by similarly large series from other institutions, staging 18F-FDG PET should become part of the standard management of MCC.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We gratefully acknowledge the assistance of Annette Hogg and Elizabeth Drummond for maintenance and interrogation of the prospective PET database at Peter MacCallum Cancer Centre.
Footnotes
Published online Jun. 10, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 12, 2012.
- Accepted for publication February 24, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-FDG PET/CT for Posttreatment Surveillance Imaging of Patients with Stage III Merkel Cell Carcinoma
- Merkel Cell Carcinoma, Version 1.2018, NCCN Clinical Practice Guidelines in Oncology
- Advances in Immunotherapy for Metastatic Merkel Cell Carcinoma: A Clinician's Guide
- Nonmelanoma Cutaneous Head and Neck Cancer and Merkel Cell Carcinoma: Current Concepts, Advances, and Controversies
- 15-Year Experience of 18F-FDG PET Imaging in Response Assessment and Restaging After Definitive Treatment of Merkel Cell Carcinoma
- Relationship Between 18F-FDG Accumulation and Lactate Dehydrogenase A Expression in Lung Adenocarcinomas
- Merkel Cell Carcinoma, Version 1.2014