


Visual Abstract

Abstract
The purpose of this study was to investigate the diagnostic and prognostic value of 18F-FDG PET/CT for surveillance imaging in patients treated for stage III Merkel cell carcinoma (MCC). Methods: This retrospective study included 61 consecutive stage III MCC patients who were clinically asymptomatic and underwent surveillance 18F-FDG PET/CT. Findings were correlated with either pathology or clinical/imaging follow-up. The median follow-up period was 4.8 y. Statistical analyses were performed. Results: 18F-FDG PET/CT detected unsuspected recurrences in 33% patients (20/61) with lesion-based sensitivity, specificity, and accuracy of 92%, 93%, and 93%, respectively. The mean ± SD SUV for malignant and benign lesions was 7.5 ± 3.9 and 3.8 ± 2.0, respectively. Unknown distant metastases, as first recurrence site, were noted in 12 of 61 patients. Those with positive disease on 18F-FDG PET/CT within 1 y of definitive treatment had relatively worse overall survival (P < 0.0001). After adjustment on stage, risk of death increased with a higher SUVmax (hazard ratio for 1 unit = 1.17; P = 0.006) and with a higher number of positive lesions on 18F-FDG PET/CT (hazard ratio for 1 additional lesion = 1.60; P < 0.001). Conclusion: Postdefinitive treatment surveillance 18F-FDG PET/CT scanning detects unsuspected recurrences and has prognostic value. Inclusion of 18F-FDG PET/CT within the first 6 mo after definitive treatment would be appropriate for surveillance and early detection of recurrence. Our data merit further studies to evaluate the prognostic implications.
Merkel cell carcinoma (MCC) is a rare aggressive cutaneous malignancy of neuroendocrine origin that has shown increasing incidence in the United States, with a reported increase of 95% during the years 2000–2013 (1,2). Patient survival depends on the stage of disease at diagnosis (3–5), with stage III MCC noted for higher metastatic potential and decreased survival than stages I and II (5-y cumulative incidence [CI] of death, 10%–15%) and substage IIIa having higher disease-specific survival than substage IIIb (5-y CI of death, 22% for IIIa and 53% for IIIb) (4,6).
After definitive therapy, recurrences occur in approximately 25%– 50% of patients, with a median time to recurrence of about 8 mo, and 90% recurrences occur within 2 y (3,6–9). Follow-up is therefore imperative in MCC, especially in higher stage disease. National Comprehensive Cancer Network (NCCN) guidelines recommend routine follow-up visits every 3–6 mo for 3 y and every 6–12 mo thereafter (3). Complete physical examination including skin and lymph node assessment is the mainstay. Currently, 18F-FDG PET/CT is not integrated in the routine follow-up. Imaging with contrast-enhanced CT and MRI is used, as clinically warranted on a case-by-case basis (3,10,11).
The overall sensitivity and specificity of 18F-FDG PET/CT for detecting primary or metastatic MCC ranges from 86% to 100% and 89% to 100%, respectively (10,12–19), and impact on management has been noted in up to 45% of patients (13,18–22). Prior studies have limited data on surveillance, include small number of patients and surveillance scans, lack pathologic correlation, and have variable disease stage and clinical status of patients. The aim of this study was to evaluate diagnostic and prognostic performance of surveillance 18F-FDG PET/CT scans obtained at least 1 mo after definitive treatment in asymptomatic patients with stage III MCC.
MATERIALS AND METHODS
This was an institutional review board–approved single-institution retrospective study, performed in compliance with Health Insurance Portability and Accountability Act regulations, and the requirement to obtain informed consent was waived. A total of 61 patients treated for stage III MCC who underwent surveillance 18F-FDG PET/CT imaging as part of standard of care were included. Staging was performed at the time of diagnosis, according to American Joint Committee of Cancer guidelines, eighth edition (23). Stage III disease included patients with suspected lymph node involvement either positive only on sentinel lymph node biopsy in patients with known primary (stage IIIA known primary), positive on clinical examination in patients with unknown primary (stage IIIA unknown primary), or positive on clinical examination and confirmed by pathology (stage IIIB) (23). Patients were not on active treatment at the time of the scan, were without any evidence or suspicion of disease as per the clinical assessment of referring physicians, and had a minimum interval of at least 1 mo since the completion of first definitive treatment. Electronic medical records were reviewed for clinicopathologic data, and mean follow-up duration was 4.8 y.
After 6 h of fasting and preinjection serum blood glucose of <200 mg/dL, patients were intravenously injected with 370--555 MBq of 18F-FDG. Whole-body scans were acquired 60--90 min after injection from vertex to toes, with patients supine. Low-dose (120--140 kV, 80 mA) CT scans with oral contrast were obtained and used for attenuation correction of PET images. All images were reviewed on a PACS workstation using the VCAR imaging suite (AW Suite 2, GE Healthcare). Maximum SUVs, normalized to body weight, were determined.
A total of 221 18F-FDG PET/CT scans were reviewed. Location, size, and SUV of 107 suspicious lesions were noted. Histopathologic correlation was available for 30 lesions as standard of reference, and clinical/imaging follow-up (≥6 mo) was performed for the remaining 77 lesions. Findings were classified as true-positive for recurrence/metastasis if confirmed by either positive histopathology from biopsies/resections or presence of detectable lesion at corresponding site on follow-up imaging showing increase in SUV or size. Comparison of findings was performed in 28 pairs of PET/CT and CT/MRI (limited regions/areas) scans acquired within 1 mo.
Statistical Methods
Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy with 95% CIs were calculated, using pathology and clinical/imaging follow-up as a reference standard. Time to recurrence was defined as time from the end of primary treatment to first recurrence detected on 18F-FDG PET/CT, confirmed pathologically or clinically; alive patients without recurrences were censored at their last date of follow-up, and deaths before recurrence were considered as competing risk. Cumulative rates of recurrence were calculated using the Aalen--Johansen estimator. Overall survival was defined from first surveillance PET/CT scan to date of death; alive patients were censored at their last date of follow-up. A Kaplan--Meier curve was used to estimate survival rates. Landmark analyses were used to compare survival, based on scan positivity at 3, 6, and 12 mo (i.e., events occurring before the landmark time were excluded, and the time was calculating from the landmark time). Survival curves were compared with a log-rank test. Cox-proportional hazards model were used for univariable/multivariable analysis to assess prognostic value of PET parameters. Scan positivity, lesion SUV, number of lesions, and disease substage were correlated with survival. Factors with a P value < 0.20 in univariate analysis were entered in multivariate analysis, and a backward variable selection was done. Adjusted hazard ratios (HRs) are presented, along with 95% CI. Statistical analysis was performed using R, version 3.5.0 (R Core Team).
RESULTS
Patient Characteristics
Patient, scan, and tumor characteristics are described in Table 1. The median interval between end of treatment and first surveillance 18F-FDG PET/CT scan was 3.7 mo (range, 1.1–23.3 mo). The time interval between consecutive scans predominantly ranged between 1.5 mo and 1.6 y, usually based on the clinician’s discretion.
Patient, Tumor, and 18F-FDG PET/CT Scan Characteristics
18F-FDG PET/CT Scan-Based Analysis
Of 221 18F-FDG PET/CT scans, 39 showed 18F-FDG–positive foci. Pathology confirmed recurrent MCC in 15 of 39 scans, and clinical/imaging follow-up confirmed recurrence in another 11 scans. Incidental second malignancy was detected in 1 scan. Overall, true-positive findings were seen in 27 scans (12%, 27/221). False-positive findings were seen in 12 scans (5%, 12/221) and confirmed on pathology in 2 and on clinical/imaging follow-up in 10 scans. A total of 182 18F-FDG PET/CT scans were negative for recurrent disease, of which 4 of the 221 (2%) were falsely negative, all confirmed on pathology. The remaining 178 scans (81%, 178/221) were true-negative based on clinical/imaging follow-up.
Lesion-Based Analysis
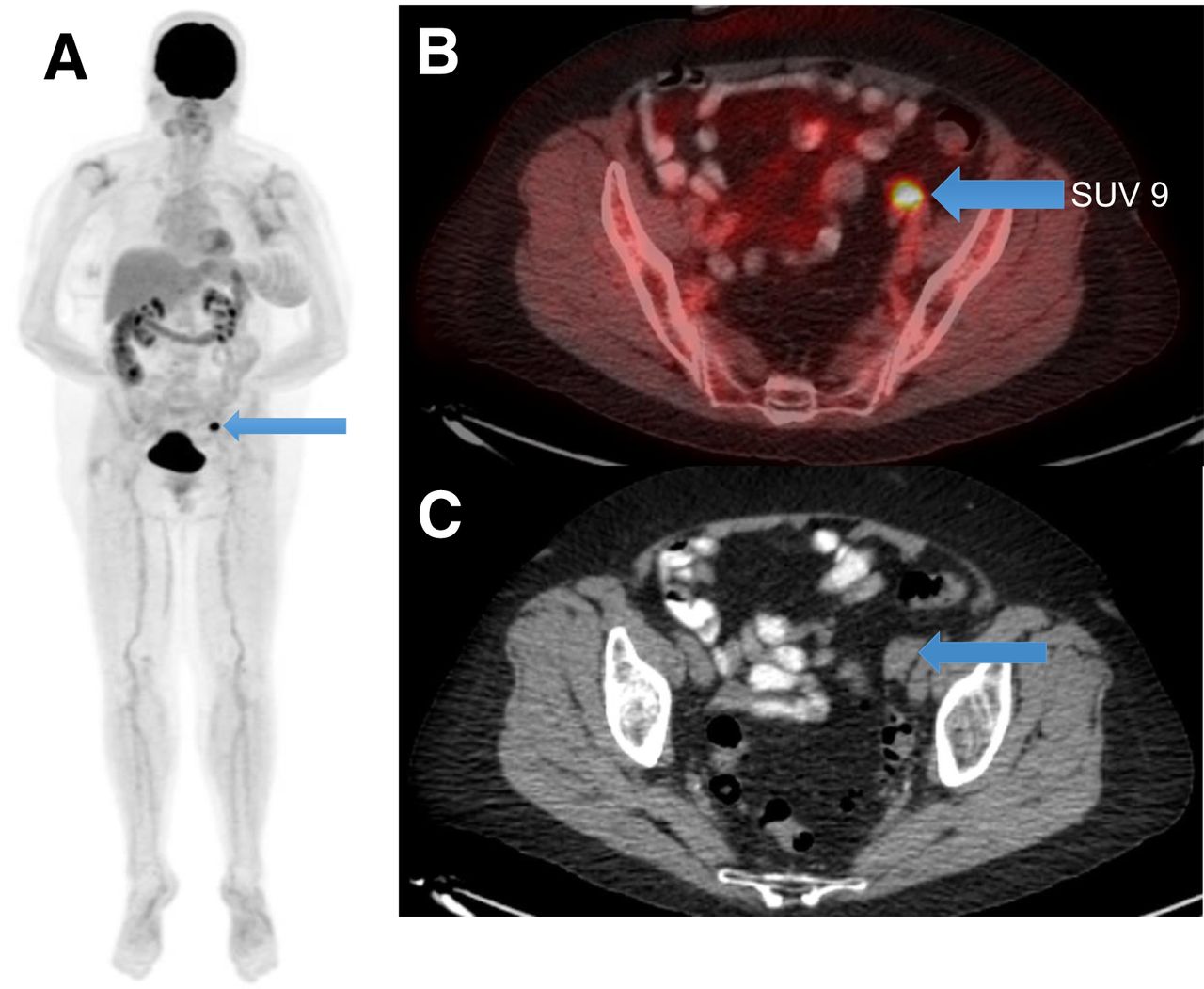
A total of 107 sites of abnormal 18F-FDG avidity were noted (Fig. 1), for which pathology confirmed disease in 24 sites and clinical/imaging follow-up confirmed in 68 sites. False-positive 18F-FDG uptake was seen in 15 sites, including nasal and axillary cutaneous sites (confirmed on pathology), pelvic fracture, rib fracture, 9 reactive neck and mediastinal nodes, and cutaneous sites in thigh and foot (confirmed on clinical/imaging follow-up). Two lesions were thought to be benign but were later confirmed as recurrent disease on pathology—lung infiltrates and neck node. Two in-transit metastases in the thigh and arm were also missed on 18F-FDG PET/CT because they were below PET resolution and too small to characterize.

Asymptomatic 70-y-old woman with left arm MCC (s/p excision, left axillary lymphadenectomy, radiation to axilla) underwent surveillance 18F-FDG PET/CT scan 3.3 mo after treatment. 18F-FDG PET/CT (A; maximum-intensity projection, arrow) scan revealed solitary focal 18F-FDG uptake in left pelvis (B; fused PET/CT, SUV 9, arrow) in a nodular soft-tissue-density lesion in left adnexa (C; axial CT, arrow). USG pelvis showed solid mass in left ovary measuring 1.8 x 1.4 x 1.6 cm, corresponding to site of abnormality on 18F-FDG PET/CT. Patient underwent salpingo-oophorectomy and pathology was positive for MCC. s/p = status post; USG = ultrasound.
Overall SUVmean ± SD for 18F-FDG–avid malignant and benign lesions was 7.5 ± 3.9 (range, 1.7–18.9) and 3.8 ± 2.0 (range, 1.6–6.0), respectively; for local recurrence, 6.5 ± 4.1 (range, 1.7–18.9); and for distant metastases 8.0 ± 3.7 (range, 2.3–18.0). Mean SUV for 18F-FDG–avid distant nodes was 7.1 (range, 2.3–12.7) and for osseous lesions 8.2 (range, 4.0–13.4). Mean size of 18F-FDG–avid distant nodal metastases was 1.3 cm in short axis (range, 0.6–2.1 cm). SUVmean ± SD for false-positive findings was 3.7 ± 1.2 (range, 1.6–6.0). On the basis of the ROC curve, the optimal cutoff SUV of 5.4 was associated with a low sensitivity of 54.9% but high specificity of 91.4% (Fig. 2).

Receiver-operating-characteristic (ROC) curve for benign versus malignant lesion prediction based on SUVmax. FPR = false-positive rate; TPR = true-positive rate.
Lesion-based sensitivity, specificity, PPV, NPV, and accuracy of PET/CT scan, calculated on the basis of correlation either with pathology or with clinical/imaging follow-up, was 92%, 93%, 86%, 96%, and 93%, respectively, whereas scan-based sensitivity, specificity, PPV, NPV, and accuracy was 90%, 94%, 69%, 98%, and 93%, respectively.
Patient-Based Evaluation
Overall, 20 patients had relapse detected on 18F-FDG PET/CT. The cumulative rate of detecting recurrences was 8.2% (95% CI, 1.3, 15.1%) within 3 mo, 16.4% (95% CI, 7.1, 25.7%) within 6 mo, and 26.2% (95% CI, 15.2, 37.3%) within 12 mo after definitive treatment. Local or locoregional relapse at or adjacent to the site of primary was seen in 8 patients, with a median interval of 4.5 mo (range,1.1–14.7 mo) from the end of treatment; disease sites included cutaneous/subcutaneous lesions in extremities (number of patients, n = 4); nodal disease in posterior auricular, inguinal, and axillary region (n = 3); and cutaneous lesion in leg with inguinal node (n = 1). Four of these 8 patients subsequently developed distant metastases. Distant metastasis, as first site of recurrence, was seen in 12 of the total 61 patients, with median interval of 7.2 mo from the end of treatment (range, 3.0–41.9 mo).
18F-FDG PET/CT findings led to implementation of treatment in 20 patients (33%, 20/61). Surgery only was performed in 4 patients including excision of cutaneous/subcutaneous lesions in extremities (number of patients, n = 3) and bilateral salpingo-oophorectomy (n = 1). Radiation only was performed in 7 patients, with sites including retroperitoneal/pelvic nodes (n = 4), pancreas (n = 1), vertebrae (n = 1), mediastinal node, and subcutaneous thigh lesion (n = 1). Chemotherapy only was administered in 3 patients, whereas 2 patients received both chemotherapy and radiation therapy to osseous sites and 1 patient received chemotherapy and radiation therapy to subcutaneous/skin lesions in lower extremities in 2 different settings. Two patients received surgery followed by radiation therapy in axilla and groin, whereas 1 patient received immunotherapy.
Comparison with CT/MRI
Comparison with 28 CT/MRI scans and PET/CT scans was available in 17 of 61 patients (28%). Of 28 CT/MRI scans, 7 showed suspicious findings. Of 7 scans, 6 were true-positives as confirmed by histology in 4 and clinical follow-up in 2. A false-positive finding was seen in 1 CT scan, confirmed on clinical follow-up that demonstrated a borderline enlarged inguinal node (non-18F-FDG–avid) in a patient with primary disease in the groin. Two findings were falsely negative on CT, including biopsy-proven in-transit metastases in thigh (non-18F-FDG–avid) and inguinal node (18F-FDG–avid) positive for recurrence in imaging follow-up. Two findings including a lung nodule and bone lesion, suspicious on 18F-FDG PET/CT and positive for recurrent disease on clinical/imaging follow-up, were outside the regional field of view of the CT/MRI scan.
Prognostic Analyses
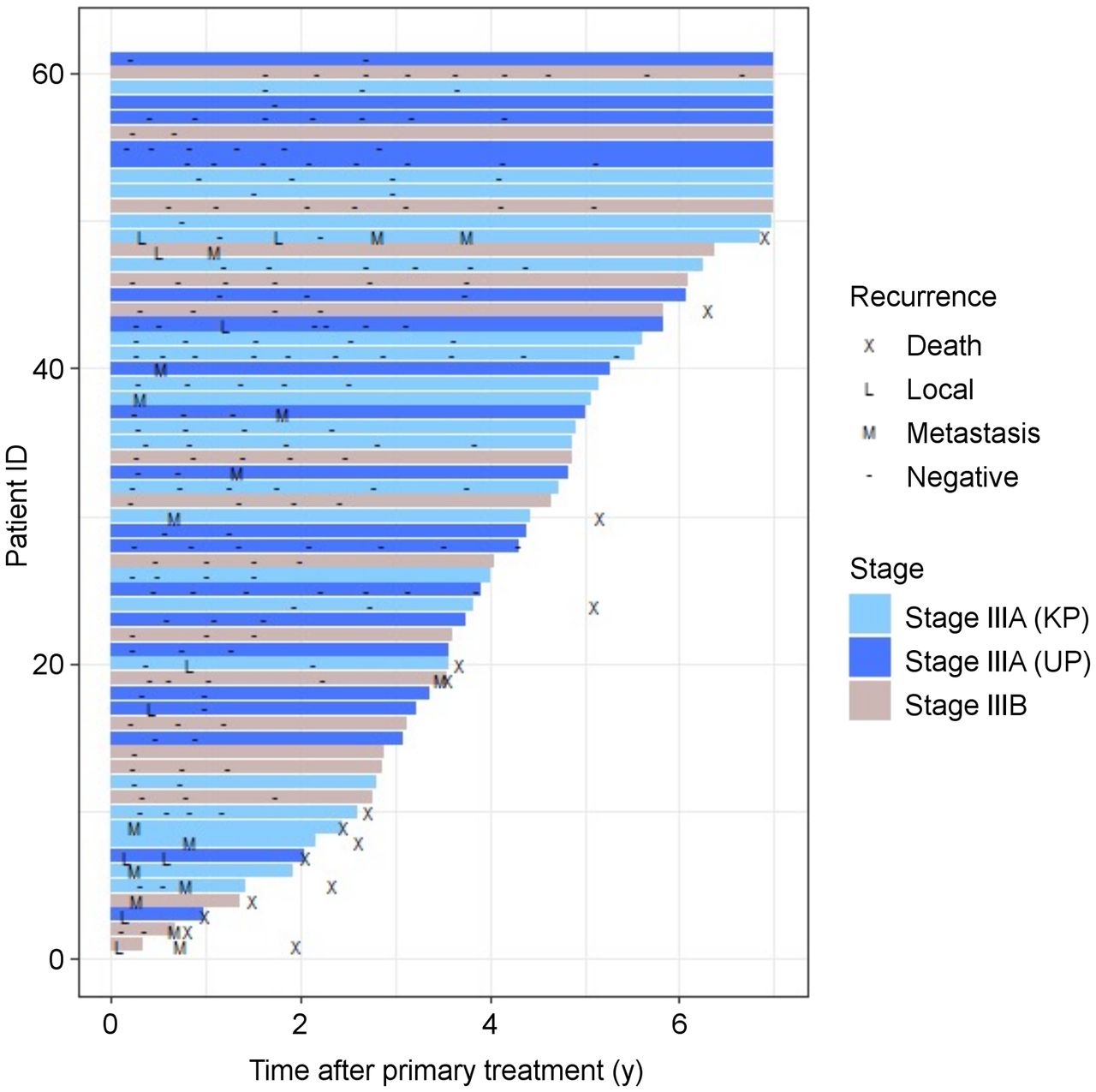
Mean follow-up duration was 4.8 y (range, 8 mo–18 y) after first surveillance 18F-FDG PET/CT. Among the 43 patients with negative scan results at 3 mo, 7 (16%) had a positive scan result later. Among the 41 patients with negative scan results at 6 mo, 5 (12%) had a positive scan result later. Among the 39 patients with negative scan results at 12 mo, 3 (8%) had a positive scan result later. Surveillance of patients is represented in the swimmer plot demonstrating the time points of 18F-FDG PET/CT scan positivity and the follow-up duration (Fig. 3). Most of the recurrences developed within 1.5 y after the end of primary treatment. On the basis of the timing of the scan, statistical analysis revealed better overall survival (OS) in patients with a negative 18F-FDG PET/CT scan result, as compared with patients with positive scan result, within 3 mo (P < 0.0001), 6 mo (P < 0.0001), and 12 mo after treatment (P < 0.0001) (Fig. 4).

Swimmer plot illustrating information about local and distant recurrences, confirmed on pathology, during follow-up on surveillance 18F-FDG PET/CT scans since end of primary treatment for all included stage IIIA known primary (KP), IIIA unknown primary (UP), and IIIB MCC patients (n = 61).

OS of patients based on findings and timing of 18F-FDG PET/CT scan (A, at 3-mo; B, at 6 mo, and C, at 12 mo after definitive treatment, respectively).
Univariable statistical analysis showed that the risk of death increased with a positive surveillance 18F-FDG PET/CT scan result, higher SUV, and higher number of 18F-FDG–avid lesions (Table 2). Multivariable analysis showed that risk of death was increased with higher SUV (HR for 1 unit = 1.17; 95% CI, 1.05 to 1.31; P = 0.006) and number of 18F-FDG–avid lesions (HR for 1 additional lesion = 1.60; 95% CI, 1.25 to 2.04; P < 0.001) and was decreased for patients with stage IIIA (unknown primary) compared with stage IIIA (known primary) (HR = 0.09; 95% CI, 0.01 to 0.99, Table 2). 18F-FDG PET/CT scan positivity was not evaluated in the multivariable model as we used a summary of the number of positive lesions.
Univariate and Multivariate Prognostic Models for OS
DISCUSSION
In this study, 18F-FDG PET/CT showed high sensitivity and specificity of 92% and 93%, respectively, to detect recurrent MCC lesions in local as well as distant sites. Overall, 12% (27/221) of surveillance 18F-FDG PET/CT scans were true-positive for recurrence, and 81% were true-negative. 18F-FDG PET/CT results contributed to implementation of treatments in 33% (20/61) patients. We also assessed the prognostic significance of 18F-FDG PET/CT, specifically in patients treated for stage III disease, which, to our knowledge, has never been reported before.
On the basis of our results, early inclusion of 18F-FDG PET/CT within the first 6 mo after definitive treatment is suitable to initiate imaging surveillance in stage III MCC patients. Although none of our patients had clinically evident disease after receiving definitive treatment, unexpected true-positive 18F-FDG PET/CT findings were detected in local or locoregional nodes in 13% (8/61) patients at a median interval of 4.5 mo after treatment; all patients had normal-appearing skin and negative clinical nodal exam. Additionally, unexpected findings were seen in distant organs including ovaries, pancreas, bone, and distant lymph nodes in 20% (12/61) of patients at a median interval of 7.2 mo after treatment. Only a few prior studies have partly evaluated follow-up 18F-FDG PET/CT in MCC, with relapse noted in 7%–15% scans and overall impact on management seen in 20%–32% patients (10,12–13,16,18,20–21). However, these studies were limited due to small patient cohort, small number of surveillance PET/CT scans included, variable disease stage, unclear clinical status of the patient at the time of scanning, and varying indications for including 18F-FDG PET/CT scans, for example, monitoring treatment response, clinically suspected recurrence, or ongoing surveillance (16,18,20,22).
We also observed that most recurrences developed within 1.5 y after definitive treatment, and 18F-FDG PET/CT enabled identification of unsuspected disease relapse, leading to appropriate treatment planning. This invites further studies, preferably of a prospective nature, to evaluate the appropriate time intervals of performing surveillance imaging in the initial posttreatment years. On the basis of our data, surveillance 18F-FDG PET/CT scans obtained within the first 6 mo of end of definitive treatment and follow-up scans spaced at intervals of 6–9 mo for at least 2 y may be beneficial, considering that most recurrences are detected within the first 2 y of diagnosis (3,6–9). Currently, there is no consensus on follow-up surveillance imaging of asymptomatic patients after treatment completion. Another study has shown slightly different results with longer mean time to recurrence of 15.3 mo, which may have been due to variable disease stage of included patients (18). A few studies that demonstrated median time to recurrence of 6–9 mo have not clearly explained the imaging modality used to detect recurrence (3,24–27).
The OS of patients with recurrence detected on 18F-FDG PET/CT was significantly reduced compared with patients with negative 18F-FDG PET/CT scan results. It is of interest that the chances of developing recurrence decreased with increasing elapsed time from the end of treatment. In our cohort, 16%, 12%, and 8% of patients who had negative 18F-FDG PET/CT scan results at 3, 6, and 12 mo after treatment, respectively, developed recurrences. In addition, the OS of patients was negatively impacted by a higher number of 18F-FDG–avid lesions and higher SUV, suggesting higher disease burden; this higher disease burden has often been reported in other malignancies as well (28). To our knowledge, none of the prior studies in the literature has demonstrated the prognostic role of surveillance 18F-FDG PET/CT scans in MCC patients. In the study by TROG (Trans Tasman Radiation Oncology Group), postradiation-treatment 18F-FDG PET/CT scans were acquired at 9 wk after the end of radiation therapy in patients with ongoing systemic treatment. The study showed positive findings in 5 of 41 patients (12%) and no impact on patient survival at 3 y (16). The nonsignificant results were attributed to small number of patients with positive PET findings and early intervention with salvage treatment (16).
In our study, 18F-FDG PET/CT showed false-positive findings in 8 patients, mainly in cutaneous sites and reactive lymph nodes with relatively low-grade uptake. These false-positive findings can be explained by overexpression of glucose transporters in infectious/inflammatory etiology (29). Histopathologic correlation is therefore needed to confirm disease in sites that appear equivocal on 18F-FDG PET/CT. Compared with CT/MRI, 18F-FDG PET/CT scanning detected disease in sites that were outside the conventional imaging field of view and in nodes that were not suspicious by size criteria on CT/MRI. The in-transit metastases were falsely negative on both conventional and metabolic imaging, perhaps related to the small size.
Our study is limited by retrospective design; variable timing of initiation, and continuation, of surveillance imaging; as well as the lack of pathologic correlation for all lesions. We did not study the cost–benefit analysis of performing 18F-FDG PET/CT scans for surveillance as it was beyond the scope of the current study; however, the risk–benefit ratio will need evaluation in future studies to understand the economic impact.
CONCLUSION
Surveillance whole-body 18F-FDG PET/CT is a sensitive imaging modality in posttreatment follow-up of asymptomatic stage III MCC patients. Our data indicate that initiating surveillance 18F-FDG PET/CT within 6 mo after completion of definitive treatment in stage III MCC may be useful in early detection of recurrence. Further scans spaced at intervals of 6–9 mo for at least 2 y may be beneficial. Larger prospective studies may help further validate these findings.
DISCLOSURE
This research was funded in part through the NIH/NCI Cancer Center Support Grant P30 CA008748. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the diagnostic and prognostic value of 18F-FDG PET/CT in surveillance imaging of stage III MCC patients?
PERTINENT FINDINGS: In this retrospective study, 61 posttreatment stage III MCC patients were included who were clinically asymptomatic, and 18F-FDG PET/CT detected unsuspected recurrent disease in 33% patients, with a high sensitivity and specificity of 92% and 93%, respectively. Risk of death was increased with higher number of 18F-FDG–avid lesions (P < 0.001) and higher lesion SUV (P = 0.006) on 18F-FDG PET/CT. Patients with recurrent disease on 18F-FDG PET/CT, within 1 year of definitive treatment, had relatively worse OS (P < 0.0001).
IMPLICATIONS FOR PATIENT CARE: Early implementation of surveillance 18F-FDG PET/CT in patients with stage III MCC allows detection of unsuspected recurrences, leading to appropriate treatment planning, and has a potential prognostic role.
Footnotes
Published online Oct. 7, 2021.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 12, 2021.
- Revision received September 25, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.