


Abstract
The aim of this study was to evaluate 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) PET for early prediction of the standard anatomic response and survival outcomes in patients with metastatic colorectal cancer (mCRC) receiving leucovorin, 5-fluorouracil (5-FU), and oxaliplatin (FOLFOX). Methods: The main eligibility criteria included histologically confirmed mCRC, ≥1 extrahepatic measurable lesions, and no prior chemotherapy in a metastatic setting. Chemotherapy consisted of leucovorin on day 1, followed by the continuous infusion of 5-FU on days 1 and 2, and oxaliplatin on day 3. In the second and subsequent cycles of chemotherapy, oxaliplatin was administered simultaneously with leucovorin on day 1. 18F-FLT PET scans were obtained 3 times during the first cycle of chemotherapy: before chemotherapy, 24 h after infusion of 5-FU (day 2), and 48 h after completion of chemotherapy (day 5). The maximum standardized uptake value (SUVMAX) of 18F-FLT was measured. Treatment responses were assessed by CT after 3 cycles of FOLFOX. Results: Eighteen patients were included in the study. The response rate after 3 cycles of FOLFOX was 27.8% (5/18). The SUVMAX was increased in responders (P = 0.043) and nonresponders (P < 0.001) on day 2 and was decreased, compared with baseline values, on day 5 in responders only (P = 0.043). Receiver-operating-characteristic curve analysis indicated that the use of a threshold of an SUVMAX increase on day 2 of ≤45.8% resulted in a sensitivity of 100%, specificity of 69.2%, and relative risk of 2.250 (P = 0.029) for the diagnosis of responders. Use of a threshold of an SUVMAX decrease on day 5 of ≥10.6% resulted in a sensitivity of 100%, specificity of 76.9%, and relative risk of 2.667 (P = 0.007). Patients with low 18F-FLT flare tended to have longer survivals than patients with high flare (2-y overall survival rate, 77.8% vs. 44.4%; P = 0.051). Conclusion: The 18F-FLT flare observed during 5-FU infusion was associated with poor treatment response in patients with mCRC. The degree of 18F-FLT flare might be used to predict the outcome of patients who receive infusional 5-FU–based chemotherapy.
- 18F-fluorothymidine
- positron emission tomography
- 5-fluorouracil
- oxaliplatin
- metastatic colorectal cancer
Colorectal cancer (CRC) is a major cause of cancer-related mortality worldwide (1). Approximately half of all patients diagnosed with CRC develop metastasis and are potential candidates for systemic chemotherapy (1,2). The overall response rate of metastatic CRC (mCRC) to first-line palliative chemotherapy is limited (<50%). An early and accurate assessment of response may allow clinicians to avoid the risk of unfavorable adverse events and unnecessary cost in the case of treatment failure and to move on to the next available therapy in the case of disease progression.
PET with 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) is potentially useful for the noninvasive measurement of cellular proliferation and may allow an early assessment of the response to chemotherapy (3). The FOLFOX regimen (oxaliplatin plus leucovorin and infusional 5-fluorouracil [5-FU]) is a reference doublet combination strategy widely used as a first-line chemotherapy. When 18F-FLT PET is used for treatment monitoring, drug-specific effects need to be considered. The best timing of therapy may also be variable, depending on the treatment (4).
The mechanism of 18F-FLT accumulation in the tumor involves nucleoside transporters and thymidine kinase 1. Adenosine triphosphate is an important cofactor for realizing the activity of thymidine kinase 1 (5,6). The upregulation and downregulation are controlled by distinct regulatory mechanisms. A negative feedback loop operates between the thymidine triphosphate pool and thymidine kinase 1, because maintenance of a balanced thymidine triphosphate pool is required for DNA replication and repair (7). By interfering with endogenous thymidine synthesis, 5-FU can cause rapid increases in the thymidine kinase levels (8,9), redistribution of nucleoside transporters (10), and marked retention of 18F-FLT. The temporary increase in retention of 18F-FLT, referred to as the flare effect, may be used in pharmacodynamic measurements of the effect of chemotherapeutic agents that block thymidylate synthase (11,12). On the other hand, by inhibiting the incorporation of thymidine triphosphate into DNA, oxaliplatin likely engenders an increase in the triphosphate nucleoside pool and reductions in thymidine kinase 1 levels and the trapping of 18F-FLT (13–15).
We hypothesized that 18F-FLT PET could be useful for identifying a subgroup of mCRC patients with clinical responsiveness to FOLFOX therapy. We conducted an exploratory study to assess the early prediction by 18F-FLT PET of the standard anatomic response and survival outcomes in patients with mCRC receiving FOLFOX.
MATERIALS AND METHODS
Study Design
This study was an open-label, nonrandomized, exploratory trial to assess whether 18F-FLT PET could be used to predict the clinical responsiveness of mCRC patients to FOLFOX as a first-line chemotherapy. The primary outcome measure was the standard anatomic objective response, as determined by the Response Evaluation Criteria in Solid Tumors (RECIST, version 1.0) (16) at 6 wk after first-line FOLFOX. The secondary outcome measure was survival outcome. This study was conducted in accordance with the Helsinki Declaration. All patients provided written informed consent before participation. The local Institutional Review Board approved the study protocol.
Patient Population
Patients were included if they had histologically confirmed adenocarcinoma that was not amenable to surgery or radiation therapy of curative intent, with ≥1 extrahepatic measurable lesions according to RECIST; an Eastern Cooperative Oncology Group performance status of 0–1; a life expectancy of ≥3 mo; no prior chemotherapy in a metastatic setting; and adequate hematologic, hepatic, and renal functions. Patients with liver-limited metastasis were excluded. Adjuvant chemotherapy with fluoropyrimidines alone was allowed if it was completed ≥6 mo before enrollment, but no prior adjuvant chemotherapy with oxaliplatin was allowed. Prior radiotherapy was permitted if it was not administered to the target lesions selected for this study and had been completed ≥4 wk before registration. Patients were recruited by referral from the investigators.
Study Treatment and Radiologic Response Evaluation
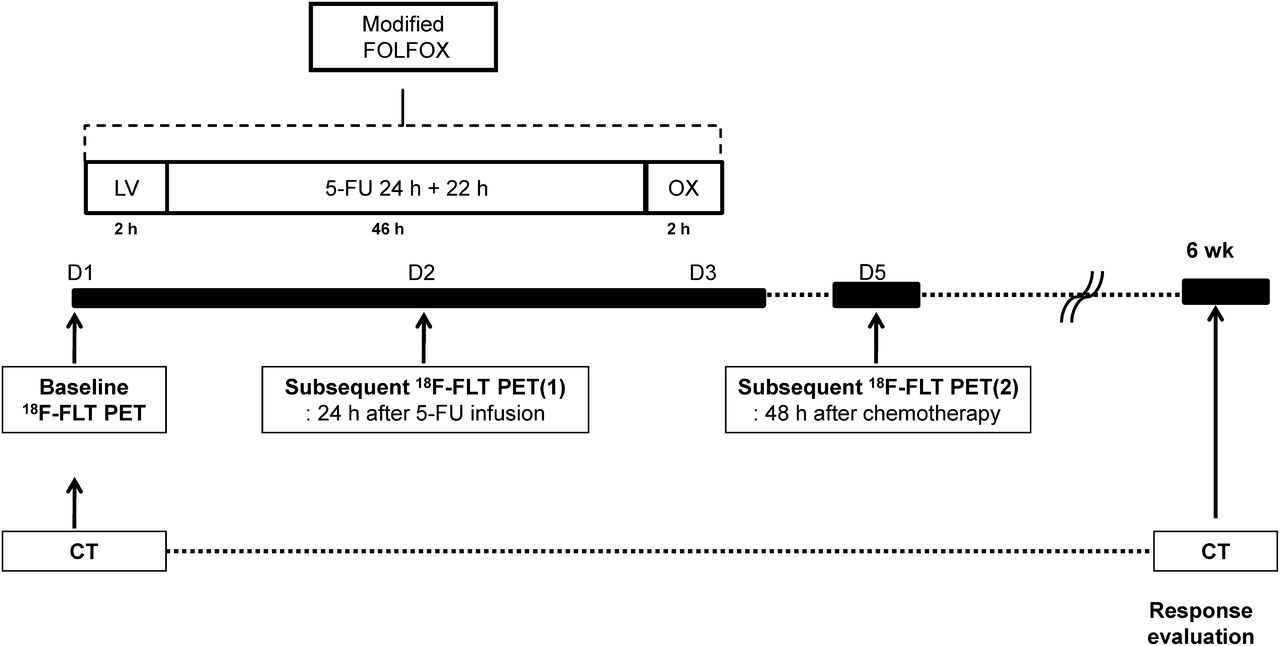
Patients were treated with a modified FOLFOX regimen, consisting of leucovorin (200 mg/m2) on day 1, subsequent continuous infusion of 5-FU on days 1 and 2 (2,400 mg/m2 for 46 h), and oxaliplatin (85 mg/m2) on day 3 (Fig. 1). Oxaliplatin was administered simultaneously with leucovorin on day 1 from the second cycle of chemotherapy. Study treatments were planned to be continued until disease progression, patient refusal, or unacceptable toxicity. CT scans were obtained within 2 wk before chemotherapy and every 3 cycles of chemotherapy (6 wk) or when disease progression was suspected. Morphologic response was evaluated by CT every 6 wk according to RECIST 1.0, without knowledge of the results of 18F-FLT PET.
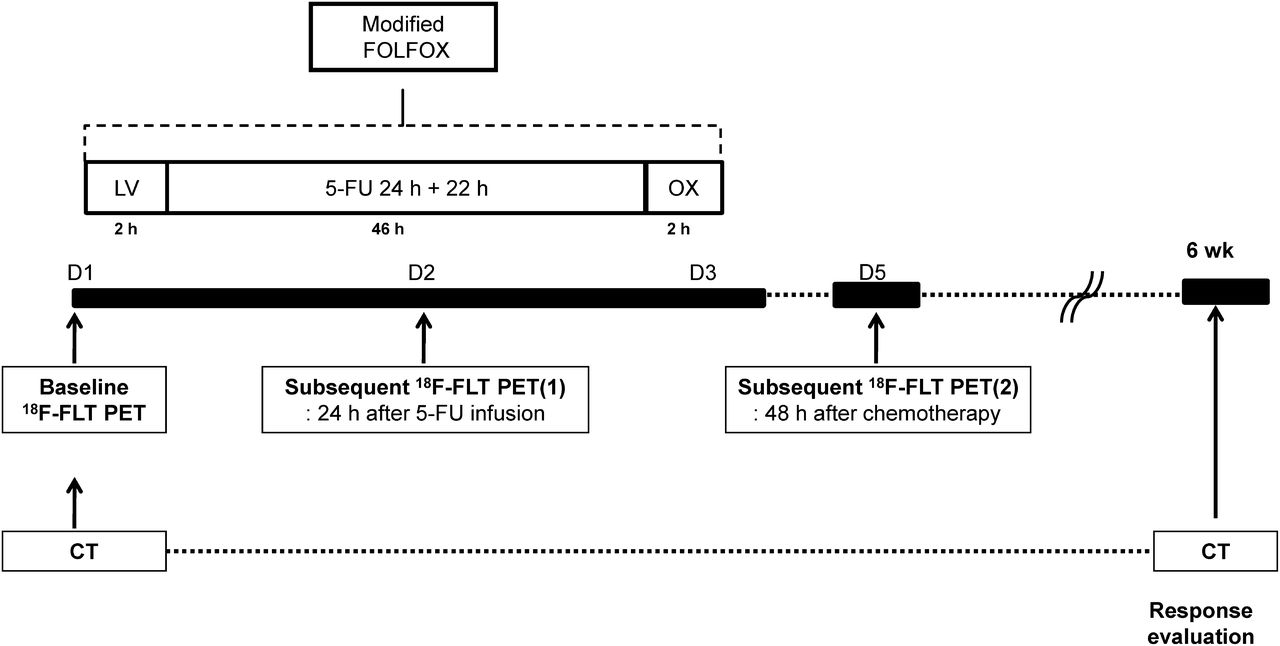
Schematic design of FOLFOX (oxaliplatin [OX] plus leucovorin [LV] and infusional 5-FU) chemotherapy and 18F-FLT PET imaging procedures.
18F-FLT PET Imaging
18F-FLT was synthesized as previously described (17). The amount of 18F-FLT injected was 159.1 ± 22.2 MBq (range, 111–185 MBq). The specific activity was ≥223 TBq/mmol. The radiochemical purity was 100.0% (range, 98.7%–100.0%).
18F-FLT PET imaging was performed 3 times before, during, and after FOLFOX chemotherapy with a PET/CT scanner (Biograph True Point 40; Siemens). Baseline 18F-FLT PET was performed within 2 wk before chemotherapy. Subsequent 18F-FLT PET studies were performed 24 h after the continuous infusion of 5-FU (day 2) and 48 h after completion of chemotherapy (day 5). The 18F-FLT PET images were obtained at 1 h after the intravenous injection of 18F-FLT. Noncontrast CT imaging (120 kV, 50 mAs, CARE Dose 4D; Siemens) from the skull base to the mid thigh was performed in a spiral mode for attenuation correction. A 3-dimensional emission scan of the same area was obtained for 2 min per bed position. For the third 18F-FLT PET study, limited-area tumor imaging with ≥2 bed positions was performed with the same acquisition parameters as were applied for the previous scan.
The effective radiation dose from three 18F-FLT administrations was estimated to be 15.5 and 18.2 mSv for male and female subjects, respectively (18). The total radiation exposure from the 3 CT examinations was ≤10 mSv. Emission images were reconstructed by True X reconstruction with 3 iterations and 21 subsets. No correction for partial-volume effects was performed.
The 18F-FLT PET results were analyzed quantitatively by the consensus of 2 board-certified nuclear medicine physicians who were masked to the clinical outcome results. Quantitative image analysis of 18F-FLT uptake included calculation of the maximum standardized uptake value (SUVMAX, single maximum pixel count within the volumes of interest) of all target lesions, which was obtained with the vendor’s software (Syngo TrueD; Siemens). The SUVMAX of 1 extrahepatic target lesion with the most intense 18F-FLT uptake was selected for the comparative analysis between treatment responses by CT scan and survival outcomes. The percentage change in SUVMAX between baseline and subsequent PET images was calculated. The standardized uptake value (SUV) of the blood pool was calculated to assess changes in 18F-FLT availability in blood to the tumor after FOLFOX by drawing a circular region of interest of 1 cm in diameter on the descending aorta and extended 2 cm over the z-axis. The SUV was defined as activity (Bq/g)/[injected activity (Bq)/body weight (g)].
Statistical Analysis
A sample size of 16 patients achieves 82% power to detect a difference of 0.1 between the null hypothesis mean of 0.30 and the alternative hypothesis mean of 0.20 for SUVMAX, with an estimated SD of 0.15 and significance level of 0.05 by 1-sided 1-sample t test. We planned for the enrollment of 18 patients, because a dropout rate of 10% was assumed.
Quantitative measurements of 18F-FLT PET are reported as median values with ranges. Other descriptive statistical data are presented as proportions and medians with ranges. The Wilcoxon signed-rank test was used to assess the significance of the change in SUV during FOLFOX treatment. Differences between 2 groups of patients were tested by the Mann–Whitney U test. Receiver-operating-characteristic curves were used to identify the optimum cutoff value of the percentage change in SUVMAX for differentiating responding and nonresponding patients. The Fisher exact test was used to correlate changes in 18F-FLT SUVMAX with treatment response after 3 cycles of FOLFOX. Overall survival (OS, time to death), progression-free survival (PFS, time to progression or death), and 95% confidence intervals (CIs) were assessed with the Kaplan–Meier method. A P value of less than 0.05 was considered to be statistically significant. All statistical analyses were performed with SPSS (version 19.0; SPSS Inc.) for Windows (IBM Co.) and GraphPad Prism (version 4.00; GraphPad Software).
RESULTS
Patient Characteristics, Treatment Response, and Survival
Between September 2009 and October 2010, 18 patients with mCRC were enrolled in this study and received FOLFOX as their first-line treatment at Asan Medical Center in Seoul, Republic of Korea. No patient declined participation after receiving the 18F-FLT injection. The patient characteristics are listed in Table 1. A total of 262 cycles of FOLFOX were administered (median, 15 cycles; range, 3–20 cycles). The most common reason for treatment cessation was disease progression (16/18 [89%]). All patients completed the 18F-FLT PET studies and were evaluable for treatment response after 3 cycles of FOLFOX. There were no deviations from the planned protocol. The response rate after 3 cycles of FOLFOX was 27.8% (95% CI, 9.8%–53.5%), with 5 partial responses, 12 stable diseases, and 1 progressive disease (Table 2). Median follow-up time was 24.5 mo (range, 7.1–34.6 mo). During this interval, 16 patients developed progressive disease, 11 of whom died. Median PFS was 8.6 mo (95% CI, 5.1–12.1 mo), and median OS was 27.8 mo (95% CI, 21.0–34.6 mo). The 2-y OS rate was 61.1%.
Patient Characteristics
Treatment Responses to FOLFOX and Changes in 18F-FLT Uptake
Early Response Assessment by 18F-FLT PET
The 18F-FLT PET studies were well tolerated by all patients, completed without any problems, and performed as planned, without any adverse events related to 18F-FLT PET. The mean time interval between 18F-FLT injection and PET imaging was 60.7 ± 3.3 min (range, 55–77 min). The mean time interval between baseline 18F-FLT PET imaging and FOLFOX chemotherapy was 2 h 30 min (range, 1 h 15 min to 3 h 42 min). There was no significant difference in the blood-pool SUVs between baseline (0.7 ± 0.1; range, 0.5–0.8) and day 2 (0.7 ± 0.1; range, 0.5–0.8; P > 0.05) or day 5 (0.7 ± 0.1; range, 0.5–0.9; P > 0.05).
Baseline SUVMAX before treatment and percentage changes of SUVMAX on days 2 and 5 during the first cycle of FOLFOX are listed in Table 2. The median baseline value of SUVMAX for the representative metastatic lesion was 4.9 (range, 1.2–11.3). 18F-FLT uptake increased on day 2 (6.9; range, 1.7–24.9; P < 0.001), but there was no significant difference in the SUVMAX between baseline and day 5 (3.5; range, 1.0–15.4). Figure 2 shows the changes in 18F-FLT uptake (SUVMAX) during and after 1 cycle of FOLFOX. The baseline SUVMAX of the representative metastatic lesion did not differ between responders (5.1; range, 1.2–7.2) and nonresponders (3.7; range, 1.7–11.3). On day 2, the SUVMAX was increased in responders (6.7; range, 1.7–10.5; P = 0.043) and nonresponders (9.5; range, 1.8–24.9; P < 0.001). Percentage changes tended to be higher in nonresponders than in responders, but the difference was not significant (Fig. 2). After 1 cycle of treatment on day 5, the SUVMAX was decreased, compared with baseline, in responders (1.7; range, 1.0–4.2; P < 0.05), but nonresponders did not show a significant change (5.1; range, 1.7–15.4; Fig. 2).

Changes in 18F-FLT uptake (SUVMAX) during (day 2) and after (day 5) 1 cycle of FOLFOX. On day 2, SUVMAX was increased significantly in responders and nonresponders. On day 5, SUVMAX was decreased, compared with baseline values, in responders (P < 0.05), but nonresponders did not show significant change. N.S. = not significant.
The receiver-operating-characteristic curve analysis showed that a threshold of an SUVMAX increase on day 2 of ≤45.8% (low 18F-FLT flare) was optimal for differentiating responders from nonresponders, with a sensitivity of 100% (95% CI, 48.0%–100.0%), specificity of 69.2% (95% CI, 38.6%–90.7%), and relative risk of 2.250 (95% CI, 1.084–4.671; P = 0.029; Table 3). Use of a threshold of an SUVMAX decrease on day 5 of ≥10.6% provided a sensitivity of 100% (95% CI, 48.0%–100.0%), specificity of 76.9% (95% CI, 46.2%–94.7%), and relative risk of 2.667 (95% CI, 1.090–6.524; P = 0.007; Table 3). The CT and 18F-FLT images of a representative nonresponder (patient 2) with high 18F-FLT flare on day 2 and a small reduction in 18F-FLT on day 5 are shown in Figure 3. Results for patient 11, who showed a partial response, low 18F-FLT flare on day 2, and large reduction in 18F-FLT SUVMAX on day 5, are illustrated in Supplemental Figure 1 (supplemental materials are available online only at http://jnm.snmjournals.org).
Treatment Response After 3 Cycles of FOLFOX According to Percentage Changes in 18F-FLT SUVMAX
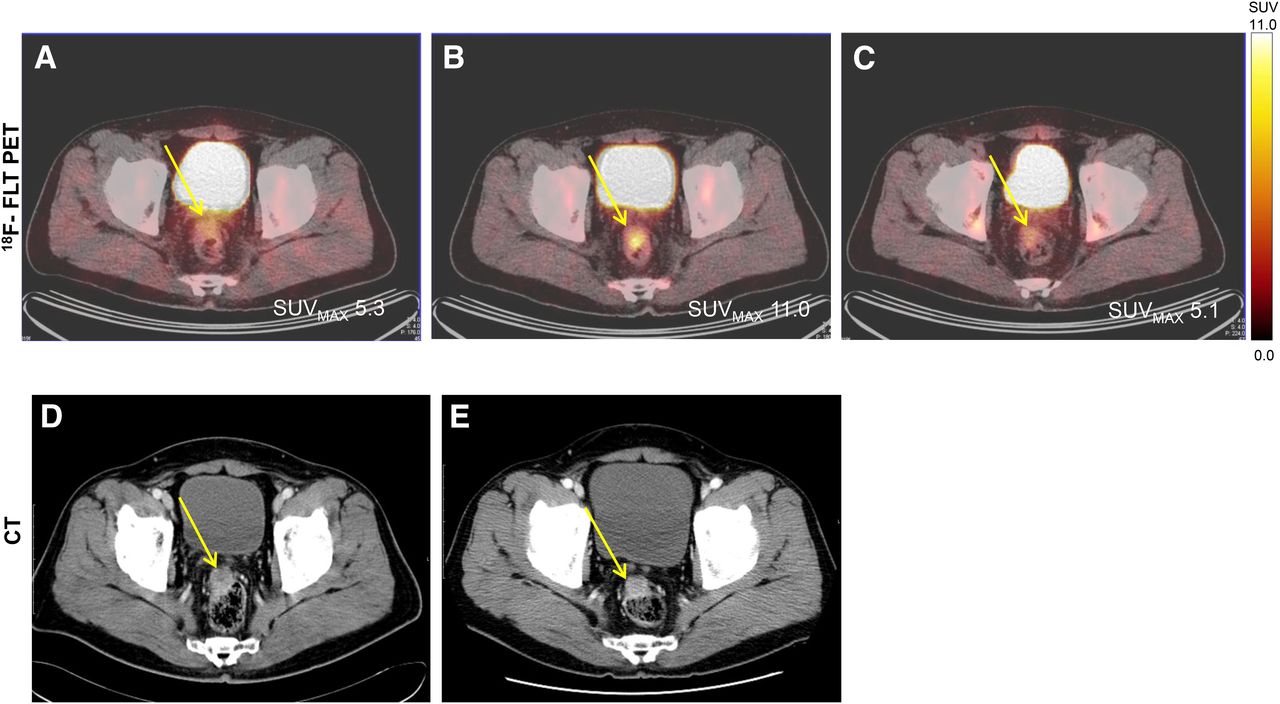
A 60-y-old man with stable disease after 3 cycles of FOLFOX (patient 2). Representative baseline (A) and day 2 18F-FLT PET (B) images showed increase in SUVMAX of peritoneal seeding nodule from 5.3 to 11.0 during 5-FU infusion (107.5% change, high 18F-FLT flare). SUVMAX after completion of first cycle (5.1) showed only –3.8% change, compared with baseline value (C). Transverse CT images before (D) and after FOLFOX (E) show 2.3% reduction in tumor size.
Interestingly, 3 patients (patients 4, 6, and 18) showed persistently increasing SUVMAX over time (Fig. 2). All these patients were nonresponders. Even after excluding these patients, SUVMAX increase on day 2 and decrease on day 5 differentiated responders and nonresponders significantly (P = 0.026).
Survival Outcomes According to 18F-FLT PET Response
The PFS and OS were compared according to the degree of 18F-FLT flare on day 2 and 18F-FLT reduction on day 5 (Fig. 4). The median PFS was 10.0 mo (95% CI, 5.0–15.0 mo) and 8.6 mo (95% CI, 6.8–10.4 mo) for the low- and high-flare group, respectively (Fig. 4A, P = 0.422). Patients with low 18F-FLT flare tended to have a longer survival than patients with high flare. OS did not reach the median value for the low-flare group, and the median OS was 18.7 mo for the high-flare group. The 2-y OS rate was 77.8% in those with low flare and 44.4% in those with high flare (P = 0.051, Fig. 4B). Six of the 9 patients with low 18F-FLT flare was still alive, whereas only 1 of 9 with high 18F-FLT flare was alive at the time of this writing. When PFS and OS were compared according to the presence of low flare on day 2 and a large reduction on day 5, 6 patients who met both criteria tended to have a higher median PFS (10.0 mo; 95% CI, 2.7–17.3 mo) than those who did not (8.3 mo; 95% CI, 7.3–9.3 mo), without statistical significance (P = 0.139, Fig. 4C). At the time this article was being written, 2 patients had no evidence of disease progression. Both of these patients showed low 18F-FLT flares on day 2 and large reductions in 18F-FLT uptake on day 5. OS showed the same tendency, without significant difference (not reached the median value vs. 18.7 mo; 95% CI, 1.4–36.0 mo; P = 0.116; Fig. 4D). Four of 6 patients with both low 18F-FLT flare and a large reduction and 3 of 12 without these criteria were alive at the time of this writing. Two-year OS rates for these groups were 83.3% and 50.0%, respectively. The PFS and OS did not show significant differences with respect to the degree of 18F-FLT reduction on day 5 (data not shown).
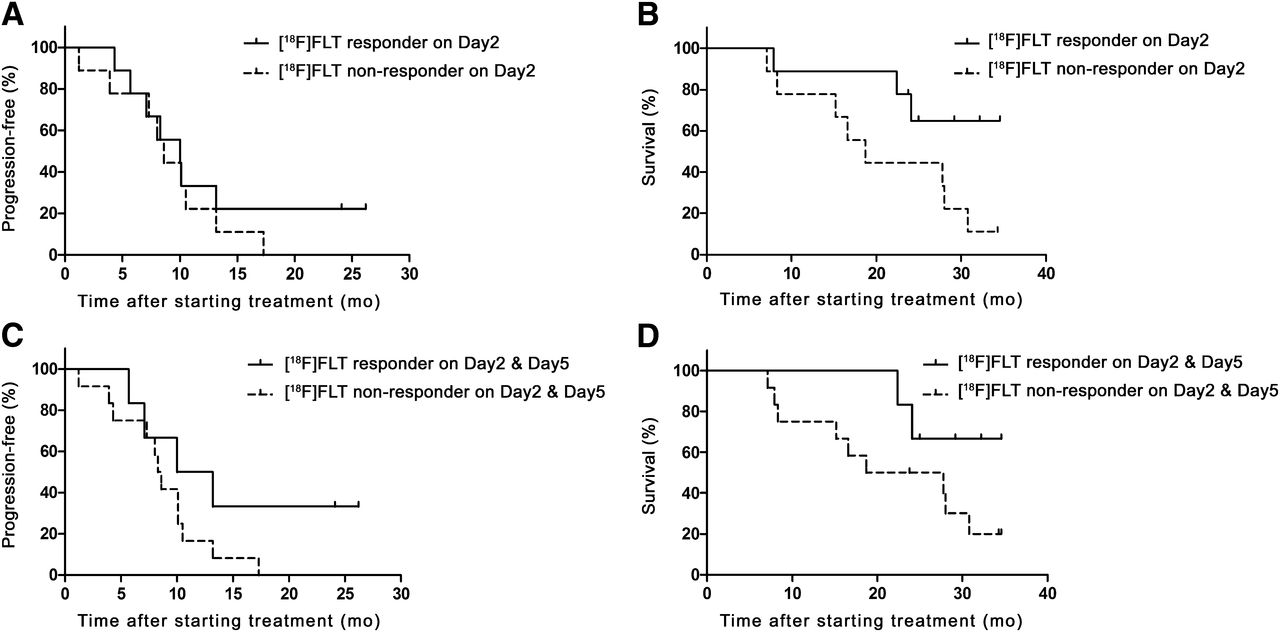
Survival outcomes according to changes in 18F-FLT uptake during and after first cycle of FOLFOX. PFS (A) and OS (B) of patients by 18F-FLT uptake response during 5-FU infusion (18F-FLT flare) were not significantly different, although there was tendency for longer survival in patients in low-flare group (2-y OS rate, 77.8% vs. 44.4%). PFS (C) and OS (D) according to presence of low flare on day 2 and large reduction on day 5 showed same tendency without significant difference.
DISCUSSION
In this exploratory study, the 18F-FLT flare, which reflects an increased uptake of 18F-FLT at 24 h during continuous 5-FU infusion, was related to poor treatment response as assessed by CT and a tendency for poor survival in mCRC patients who received FOLFOX. Decreased 18F-FLT uptake after oxaliplatin was also related to treatment response. The 2 patients without disease progression showed low 18F-FLT flares after 5-FU and large reductions after oxaliplatin. Our findings suggest the feasibility of using 18F-FLT PET imaging for the earlier prediction of treatment response in patients with mCRC receiving FOLFOX.
The combined use of 5-FU and leucovorin inhibits thymidylate synthase and depletes deoxythymidine triphosphate, which is the major effector of 5-FU cytotoxicity (19,20). Resistance to 5-FU may develop through various mechanisms. One mechanism that is related to 18F-FLT flare is the activity of the salvage pathway in circumventing the inhibition of pathways of de novo synthesis (21). The contribution of the salvage pathway to clinical resistance to 5-FU is supported by the increased accumulation of substrates of the salvage pathway after the inhibition of de novo synthesis (7,22), reduced activity of thymidylate synthase inhibitors in the presence of extracellular thymidine (23–26), enhancement of the anticancer activity of 5-FU after thymidine transport is inhibited (27–29), and increased activity of thymidylate synthase inhibition in thymidine kinase–deficient tumors (25,30). Increased thymidine is available through the flare-related redistribution of transporters and increased thymidine kinase 1 activity. The observed association between 18F-FLT flare and poor treatment responses may be explained by the fact that the salvage of de novo synthesis inhibition contributes to resistance to 5-FU. In a previous in vitro study, even subtherapeutic doses of thymidylate synthase inhibitors were able to induce an increase in 3H-thymidine uptake (15). This finding also suggests that 18F-FLT flare may not be related to treatment response. The relative use of the exogenous and endogenous pathways are potentially confounding factors that must be considered when interpreting 18F-FLT PET results (31). 18F-FLT flare may indicate the activity of the salvage pathway for cellular proliferation when therapy is intended to suppress the de novo pathway. It is important to consider that 18F-FLT PET in this study assessed only the pharmacodynamic effect of 5-FU, whereas treatment responses were assessed after FOLFOX. It is known that patients who have failed therapy with 5-FU alone respond better to oxaliplatin if it is combined with 5-FU. It is probable that the low 18F-FLT flare associated with favorable outcome in this study may also be linked to the synergistic effect of oxaliplatin and 5-FU.
18F-FLT uptake in the tumor, as viewed by in vivo imaging, reflects the viable cell density and the avidity of 18F-FLT incorporation on a per-cell basis (32). Previous in vitro and animal studies showed that a transient increase in the cellular 18F-FLT uptake followed by a dose-dependent decrease in 18F-FLT uptake was correlated with a decrease in cell viability or inhibition of DNA synthesis after 24 h (10,13–15). 18F-FLT flare was reported as early as 1 h after the administration of drugs inhibiting thymidylate synthase (10–12), until up to 24 h after 5-FU treatment (9,13). However, successful therapy will eventually reduce 18F-FLT uptake in the tumor as early as 24 h after 5-FU treatment, and afterward the reduction may be even more pronounced (10,13–15). This notion implicates the importance of the time point when 18F-FLT PET is used to assess the tumor response after treatment. In this study, 18F-FLT flare was assessed at 24 h after 5-FU infusion. The time point of day 2 was chosen on the basis of our previous observation that high 18F-FLT flare occurred at 24 h after 5-FU treatment in most of the cell lines tested (9). It is possible that the 5-FU–induced 18F-FLT flare may indicate resistance to 5-FU. Compromised cell viability or inhibition of DNA synthesis may predominate and lead to decreased rather than increased 18F-FLT uptake at 24 h after 5-FU treatment in tumor cells with responders. In the clinical setting, 18F-FLT uptake in the tumor after 5-FU treatment is highly complex and variable. More information on the short- and intermediate-term effects of 5-FU on the enzyme and transporter activities and 18F-FLT uptake is clearly needed. It will also be essential to determine what the clinically appropriate time point for 18F-FLT PET testing should be.
We showed a correlation between the radiologic response and SUVMAX changes on day 5 after oxaliplatin administration. The timing of the third 18F-FLT PET study on day 5 was based on the results from preclinical studies that showed the effect of cisplatin on 18F-FLT or thymidine uptake (13–15). Modern treatment regimens usually use combinations of drugs and radiotherapy. The various components of these therapies may affect the thymidine triphosphate pool size in opposite directions, making the effects on 18F-FLT uptake difficult to predict. Because 5-FU and oxaliplatin may increase or decrease the thymidine kinase 1 activity, it may not be possible to investigate the predictive role of 18F-FLT PET on day 5 relative to the oxaliplatin efficacy. Further investigations on time-induced changes in the expression of nucleoside transporter proteins and key enzymes of thymidine synthesis and metabolism are necessary to confirm our observation. A later time point in the treatment cycle may be better to measure the overall antiproliferation effect of the combination. In this study, we modified FOLFOX for only the first cycle, delaying the administration of oxaliplatin until day 3 after completion of 5-FU infusion. This modification was used to isolate the effects of 5-FU on 18F-FLT flare. The timing of oxaliplatin administration might not have affected the entire efficacy of FOLFOX in this study (33).
This study has several limitations, including small sample size and the exclusion of patients with liver-limited metastases. 18F-FLT is actively taken up into the liver and metabolized to 18F-FLT glucuronide. Increased background activity in liver tissue can affect tumor uptake by partial-volume effects and respiratory motion (34). We may overcome this limitation by including large-sized metastatic lesions (34) or using a dynamic imaging analysis (35). Another limitation of this study is that we included target lesions in the liver and other organs for the evaluation of morphologic treatment response, whereas the measurements of 18F-FLT were performed with hepatic metastases excluded. However, morphologic responses of hepatic and extrahepatic target lesions were in the same direction in each patient. We have no patients who appeared to have a discrepant response, where target lesions in and outside the liver behaved differently (data not shown). Finally, only static images were acquired and later time points analyzed. However, we analyzed the 18F-FLT flare in which a high fraction of 18F-FLT might be phosphorylated. Our SUV analysis at later time points was simple and well tolerated in all patients. No significant difference in the blood-pool SUVs after FOLFOX may indicate no changes in 18F-FLT availability in blood to the tumor. Our measurements might not introduce a significant bias associated with the 18F-FLT metabolite and perfusion.
CONCLUSION
18F-FLT flare observed during continuous infusion of 5-FU and decreased 18F-FLT uptake seen after oxaliplatin administration were related to poor treatment response as assessed by delayed anatomic imaging and were also associated with a tendency for poor survival outcomes. Further investigations are needed to assess whether 18F-FLT uptake has potential as a predictive imaging biomarker of treatment response to FOLFOX. More studies are needed to establish the clinical value of 18F-FLT flare in predicting chemoresistance after thymidylate inhibition in a larger cohort of patients.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study was supported by a grant from the Korea Healthcare Technology R&D Project, Ministry of Health and Welfare, Republic of Korea (A070001 and A062254). No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Jun. 26, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 9, 2012.
- Accepted for publication February 26, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}