


Abstract
Radiolabeled metaiodobenzylguanidine (mIBG) is a highly sensitive and specific marker for detecting neuroblastoma. A semiquantitative mIBG score (Curie score [CS]) was assessed for utility as a prognostic indicator for a cohort of patients with high-risk metastatic disease. Methods: mIBG scans from 280 patients with mIBG-avid, stage 4 neuroblastoma enrolled on the Children’s Oncology Group (COG) protocol A3973 were evaluated at diagnosis (n = 280), after induction chemotherapy (n = 237), and after an autologous stem cell transplantation (n = 178). Individual mIBG scans were evaluated at 10 different anatomic regions, with the scoring of each site (0–3) based on the extent of disease at that anatomic region. Results: There was no correlation between CS at diagnosis and subsequent treatment outcome. Patients with a CS > 2 after induction therapy had a significantly worse event-free survival (EFS) than those with scores ≤ 2 (3-y EFS: 15.4% ± 5.3% vs. 44.9% ± 3.9%, respectively; P < 0.001). A postinduction CS > 2 identified a cohort of patients at greater risk for an event, independent of other known neuroblastoma factors, including age, MYCN status, ploidy, mitosis-karyorrhexis index, and histologic grade. For MYCN-amplified tumors, the presence (CS > 0) versus absence (CS = 0) of residual mIBG avidity after induction was associated with a significantly worse outcome (3-y EFS: 11.8% ± 7.8% vs. 49.6% ± 7.7%, respectively; P = 0.003). After transplantation, patients with a CS > 0 had an EFS inferior to that of patients with a CS of 0 (3-y EFS: 28.9% ± 6.8% vs. 49.3% ± 4.9%, respectively [n = 133]; P = 0.009). Conclusion: Curie scoring carries prognostic significance in the management of patients with high-risk neuroblastoma. In particular, patients with CSs > 2 after induction have extremely poor outcomes and should be considered for alternative therapeutic strategies.
Outcomes for patients with stage 4 high-risk neuroblastoma have been historically poor, with 5-y disease-free survival rates of only 30%–46% for patients older than 1 y (1–3). Despite multimodal therapy, durable remission rates remain low, with 10%–15% of patients progressing during induction therapy and another 40% progressing after an initial response to induction (2,3). The addition of autologous stem cell transplantation (ASCT) after induction therapy, improved surgical and radiotherapy techniques, and the recent use of a chimeric anti-GD2 antibody after transplantation have all led to incremental improvements in disease-free survival (4). The ability to identify both clinical and biologic prognostic markers of response early in a patient’s clinical course may significantly affect subsequent therapy, identifying individuals who may benefit from augmented or alternative therapy.
Metaiodobenzylguanidine (mIBG) is an aralkylguanidine with structural similarity to the catecholamine norepinephrine (5). Scintigraphic studies in the 1980s confirmed the ability of radiolableled mIBG to localize both pheochromocytoma (6,7) and neuroblastoma (8–11). Radioiodination studies with 131I and 123I have been performed, with both 131I-mIBG and 123I-mIBG currently licensed for scintigraphic imaging of neuroblastoma. Approximately 90% of neuroblastomas concentrate either 123I-mIBG or 131I-mIBG within marrow, cortical bone, or soft-tissue sites of disease (11–13). 123I- and 131I-mIBG uptake has been noted in patients with low- or advanced-stage disease, favorable or unfavorable histologic patterns, amplified or nonamplified MYCN gene status, and elevated or normal catecholamine levels (11).
Previous studies have indicated that mIBG uptake may be a useful surrogate marker for evaluating response to therapy (14–21). Initial reports focused on the qualitative features of mIBG scans, primarily noting whether disease was detectable. Over the past 15 y, a semiquantitative scoring system (Curie scoring) has been developed to predict the extent and severity of mIBG-avid disease (14–16). The Curie scoring system has been reproducible, with good intra- and interobserver concordance (16). The presence of mIBG-avid disease immediately before myeloablative therapy has been associated with subsequent disease progression using these criteria (15–17,20,22). However, these studies were often limited by small sample sizes or heterogeneous study populations and therapy regimen (16,22).
The aim of our current study was to investigate the use of the Curie scoring system as a prognostic marker of response and survival for patients with mIBG-avid, stage 4 newly diagnosed high-risk neuroblastoma, treated on the recent Children’s Oncology Group (COG) protocol A3973. The determination of an optimal cut-point with respect to survival at each time point—at diagnosis, after induction, and after transplantation—is examined.
MATERIALS AND METHODS
Patient Population
Three hundred nine patients with newly diagnosed stage 4 (per International Neuroblastoma Staging System) (23) high-risk neuroblastoma who were enrolled on COG protocol A3973, had not received prior systemic therapy, and had undergone mIBG scans at diagnosis were eligible for analysis. Of these 309 patients, 280 (90.6%) exhibited mIBG-avid disease at diagnosis and were subsequently included in this analysis. The 29 patients with non–mIBG-avid disease at diagnosis were excluded from postdiagnosis outcome analysis. All patients had undergone an 123I- or 131I-mIBG scan at diagnosis, with subsequent scans obtained after induction (n = 237) or after ASCT (n = 178) (Table 1). Written informed consent was obtained from all patients (or legal guardians) before study entry.
Patient Characteristics at Diagnosis
Treatment
Treatment consisted of 6 cycles of induction chemotherapy, surgical resection of residual soft-tissue disease, autologous peripheral blood stem cell transplantation (ASCT), radiotherapy, and biotherapy (Fig. 1). Patients were randomized at study entry to undergo purged or unpurged autologous stem cell collection after the second cycle of induction therapy, with subsequent ASCT after the sixth induction cycle. Tumor cell purging of peripheral blood stem cells was performed using immunomagnetic beads in a central laboratory. Radiotherapy guidelines for the primary and metastatic sites were specified, including the total dose administered and fractionation. Patients subsequently received 6 monthly cycles of isotretinoin beginning day +66 after transplantation. In addition, 46 patients were enrolled onto COG ANBL0032 and treated with chimeric anti-GD2 antibody plus isotretinoin (4).

Overview of COG A3973 therapy. mIBG scans were obtained at 3 time points: (1) at diagnosis, (2) after induction, and (3) after ASCT. Study therapy: induction cycles 1, 2, 4, and 6 (cyclophosphamide, doxorubicin, and vincristine); induction cycles 3 and 5 (cisplatin and etoposide). ASCT (carboplatin, etoposide, and melphalan). Radiotherapy (XRT) to primary and metastatic sites, beginning no sooner than 28 d after ASCT. Biotherapy: isotretinoin given for 14 consecutive days in 28-d cycle (6 cycles) ± ch14.18 antibody.
Diagnostic Imaging: mIBG Scans
Diagnostic imaging was performed with either 123I-mIBG or 131I-mIBG scanning techniques (11,24). For thyroid protection, supersaturated potassium iodide was typically begun 24 h before the diagnostic mIBG dose and subsequently continued for 3–7 d. 123I-mIBG or 131I-mIBG planar images, with or without tomography, were acquired using recommended guidelines (11,24).
mIBG Semiquantitative Scoring: Modified Curie Scoring Method
mIBG scoring was performed using a modified Curie scoring system. Initially developed in 1995, scoring is based on the presence of mIBG uptake in multiple anatomic regions (14,15). Ten different sites were scored, including 9 skeletal sites (head, chest, T-spine, L-spine, pelvis, upper arms, lower arms, femurs, and lower legs) and an additional tenth site for soft-tissue lesions (Fig. 2A). Skeletal sites were individually scored from 0 to 3 as follows: 0, no mIBG involvement; 1, one mIBG-avid lesion present; 2, more than one mIBG-avid lesion present; and 3, mIBG avidity present in >50% of an individual site. Soft-tissue lesions were scored as follows: 0, no mIBG involvement; 1, one mIBG-avid soft-tissue lesion present; 2, more than one mIBG-avid soft-tissue lesion present; and 3, mIBG avidity in a soft-tissue lesion that occupied >50% of the chest or abdomen. A patient’s Curie score at each time point was calculated as the sum of scores over all individual sites, with a maximum score of 30 (Fig. 2B). All mIBG scans were centrally reviewed by 2 nuclear medicine physicians, without knowledge of original scan reports, CT scan results, or other clinical information.

(A) Anatomic regions for Curie scoring. (B) Anterior and posterior images from 123I-mIBG scans obtained at diagnosis (left) and at end of induction (right) in patient with stage 4, high-risk neuroblastoma. At diagnosis, there was diffuse abnormal 123I-mIBG uptake throughout entire axial and appendicular skeleton (regions 1–9) and uptake in solitary soft-tissue mass, resulting in Curie score of 28 (score = 27 [3 × 9 skeletal regions] + 1 [soft-tissue region]). After induction, there was decreased but persistent abnormal 123I-mIBG uptake resulting in Curie score of 12 (score = 3 [region 1] + 1 [region 5] + 3 [region 6] + 3 [region 8] + 2 [region 9]).
Statistical Analysis
Patients were categorized by Curie score (0 vs. >0; ≤ optimum cutoff vs. > optimum cutoff) and compared with respect to survival at each time point. The optimum cutoff was determined by maximizing the Youden index with respect to how well the Curie score differentiated patients who had and did not have an event, defined as relapse, progressive disease, secondary malignancy, or death. For instance, a patient with an event with a Curie score above a particular cutoff value would be correctly categorized whereas a patient with an event and a Curie score below the cutoff value would be incorrectly categorized. The Youden index is the maximum of (sensitivity + specificity – 1) over all threshold values of the Curie score and allows evaluation of a diagnostic test with respect to its true-positive and true-negative rates (25,26).
Survival comparisons were drawn at each individual site by score (0 vs. >0 only) and for patients with MYCN-amplified and -nonamplified tumors. The percentage change in Curie score from diagnostic to postdiagnostic scans for patients with both sets of mIBG scan readings was stratified on the basis of score reduction (≥ or <50% reduction and ≥ or <75% reduction), with survival compared between groups.
For event-free survival (EFS), time to event was defined as the time from diagnosis until the time of first event, or until the time of last contact if no event occurred. For overall survival, death was the only event considered. At each postdiagnosis time point, time to event was calculated from the date of the mIBG scan. Patients who had an event between the date of diagnosis and the date of postdiagnosis mIBG scan went off-study and hence were not included in the analysis at that time point. Survival analyses were performed using the methods of Kaplan and Meier (27), with standard errors per Peto et al. (28). EFS and overall survival are presented as the rate ± SE. Survival curves were compared using a log-rank test. The freeze date for the survival data was August 2009.
To determine the independent prognostic strength for survival of the Curie score in the presence of various prognostic factors, including age (<18 mo vs. ≥18 mo), MYCN status (nonamplified vs. amplified), and ploidy (hyperdiploid vs. diploid), Cox proportional hazards models with the Efron method of handling tied event times were fit. Shimada histology was not included in the models because it is confounded with age; thus, the component variables mitosis-karyorrhexis index (low or intermediate vs. high) and histologic grade (undifferentiated or poorly differentiated vs. differentiating) were included instead. Any violations of the proportional hazards assumption were handled by treating the covariate as time-dependent, accomplished by including a covariate by survival–time interaction term in the model (29). Backward selection was used to determine the most parsimonious model. P values of less than 0.05 were considered statistically significant.
RESULTS
Characteristics for the 280 patients at diagnosis are shown in Table 1. Six hundred ninety-five mIBG scans were scored: 280 at diagnosis, 237 after induction, and 178 after transplantation. 123I-mIBG scintigraphy was used in 509 (73%) scans and 131I-mIBG in 186 (27%). In 260 (93%) of the 280 patients, the same radioisotope was used for imaging at all time points. No differences were noted in median Curie scores or EFS on the basis of the type of radioisotope used for imaging, allowing us to combine 123I- and 131I-mIBG scan results for analysis (30). The median Curie score at diagnosis was 12 (range, 1–30); after induction, 0 (range, 0–26); and after transplantation, 0 (range, 0–24).
At Diagnosis
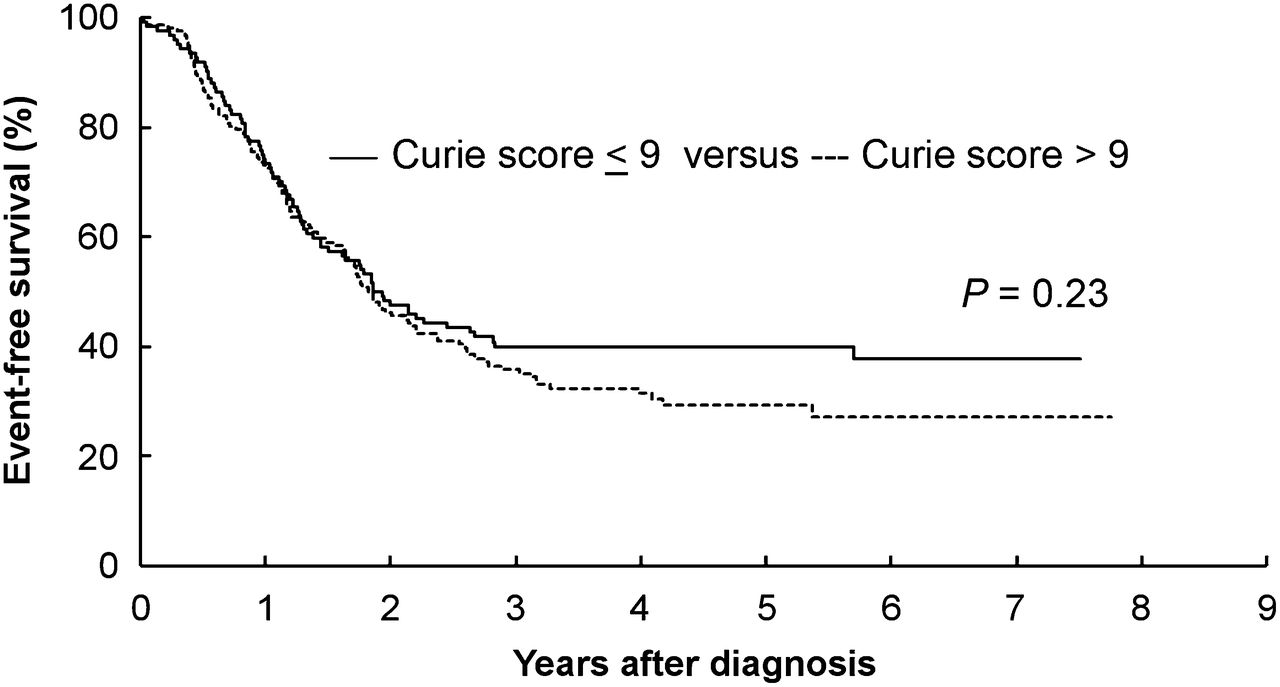
The 3-y EFS for the 280 patients with mIBG-avid disease (Curie score > 0) at diagnosis was 37.6% ± 3.0%. The optimal cut-point for analyses, as determined by the Youden index, was a Curie score of 9. Three-year EFS was 39.9% ± 4.7% for patients with a Curie score ≤ 9 (n = 124) versus 35.8% ± 4.0% for those with a score > 9 (n = 156) at diagnosis (Fig. 3, P = 0.23). Individual sites of mIBG-avid disease at diagnosis did not affect EFS (data not shown). MYCN status was available in 225 of the 280 cases. When stratified by the presence or absence of MYCN amplification, EFS was not affected by Curie scores at diagnosis.
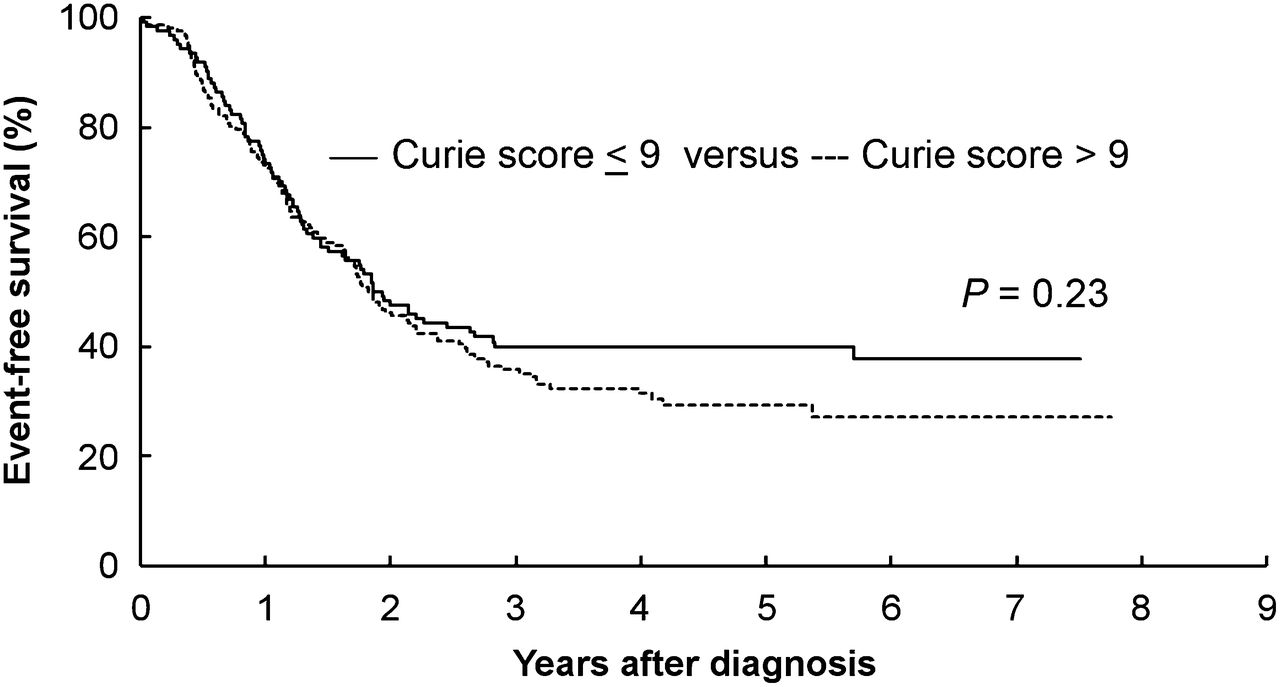
EFS by Curie score (≤9 vs. >9) at diagnosis (P = 0.23), based on Youden index determination of optimal cut-point.
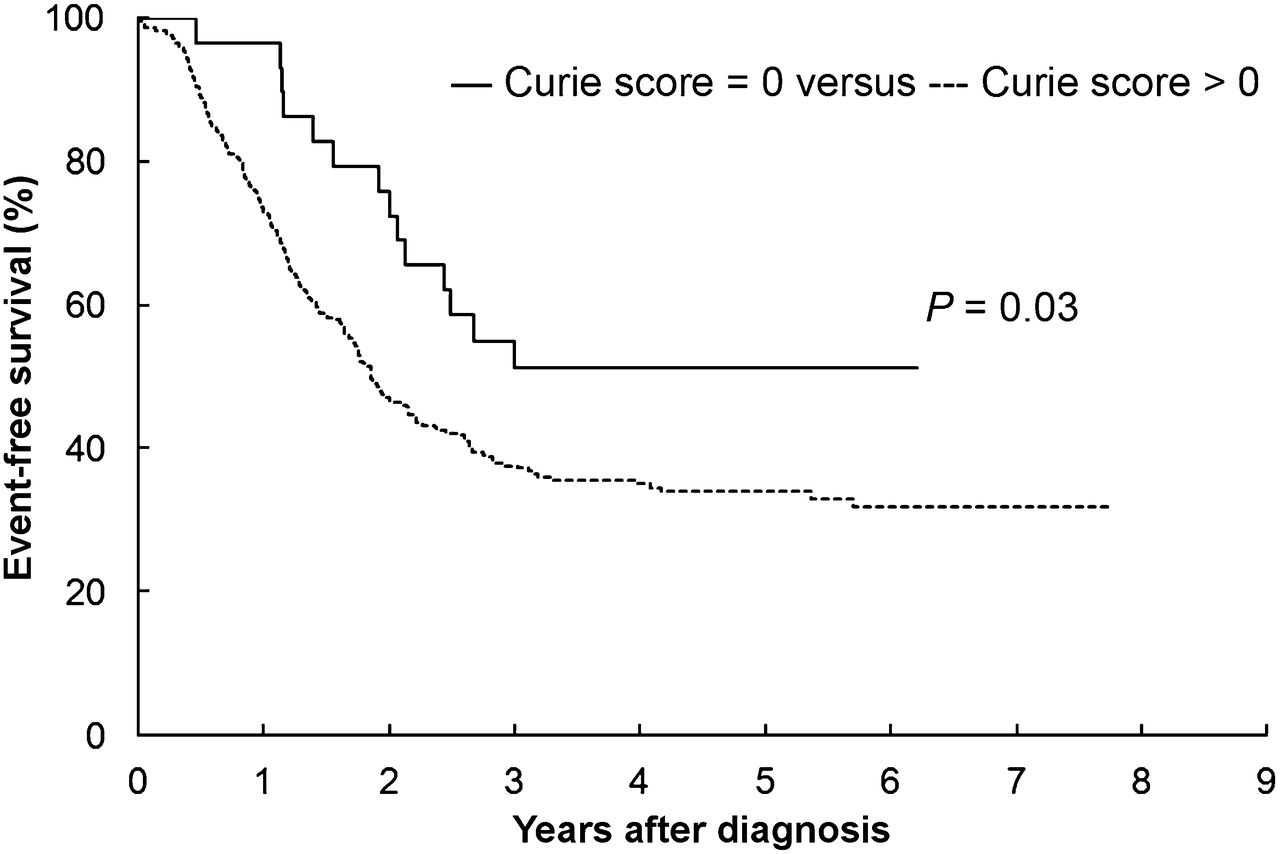
The 3-y EFS was significantly higher for the subset of patients (n = 29) with non–mIBG-avid disease (Curie score = 0) at diagnosis than for the 280 patients with mIBG-avid disease present (55.0% ± 9.5% vs. 37.6% ± 3.0%, P = 0.033) (Fig. 4). Patients with non–mIBG-avid disease at diagnosis were excluded from any subsequent analysis.
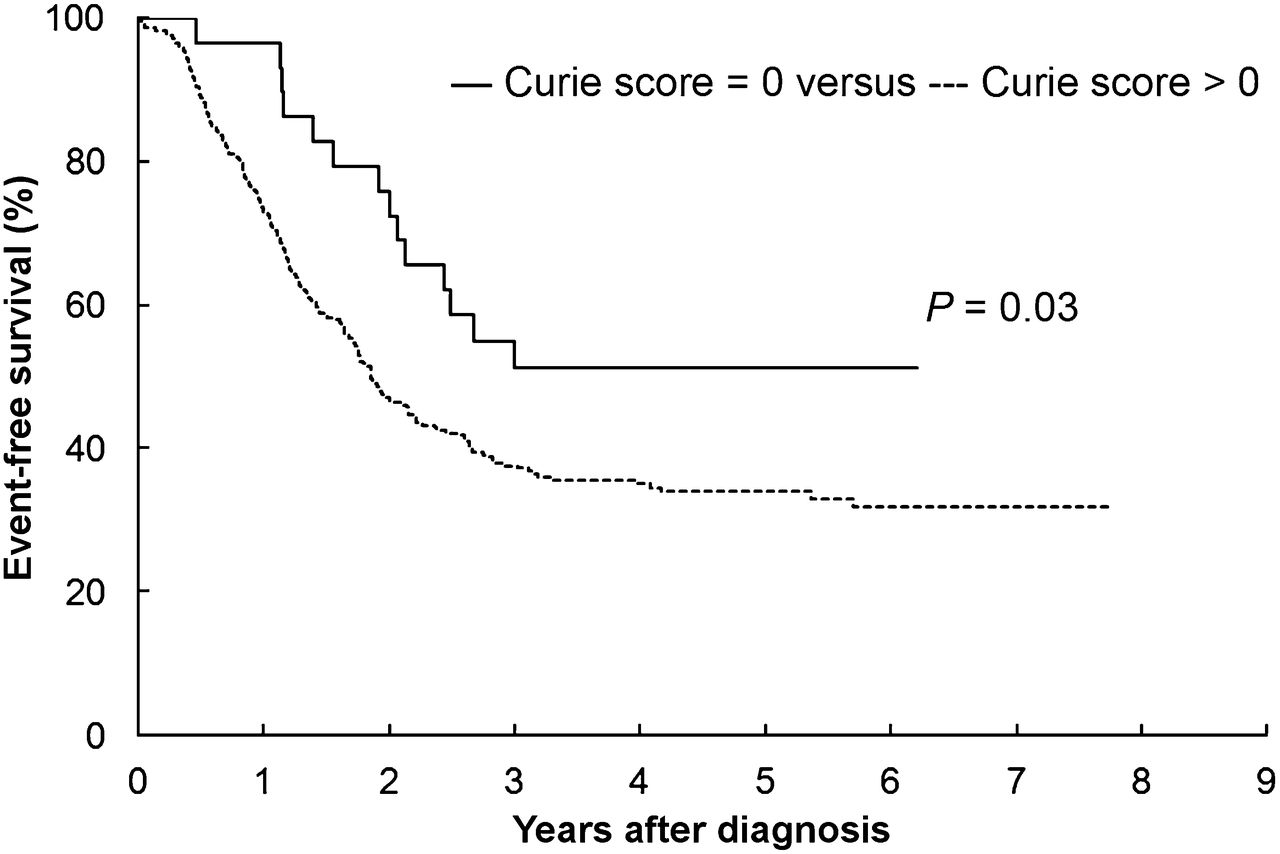
EFS for patients with Curie score (0 vs. >0) at diagnosis (P = 0.033).
After Induction
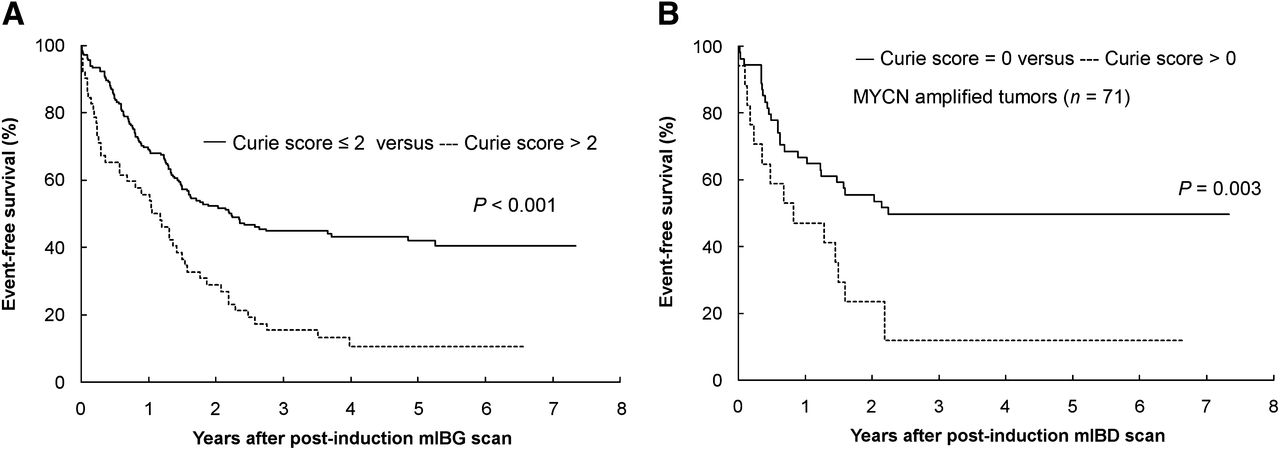
The 3-y EFS for the 237 patients with mIBG scans after induction was 38.3% ± 3.4%. EFS was subsequently determined according to Curie score, with time to event starting from the date of the postinduction mIBG scan. The optimum cut-point after induction, determined by maximizing the Youden index, was a Curie score of 2. Patients with a Curie score > 2 (n = 52) had a significantly decreased EFS in comparison to those with Curie scores ≤ 2 (n = 185) after induction (3-y EFS: 15.4% ± 5.3% vs. 44.9% ± 3.9%, P < 0.001) (Fig. 5A). The presence of any mIBG-avid disease (Curie score > 0, n = 93) after induction was also associated with a significantly worse EFS than a Curie score of 0 (n = 144) after induction (3-y EFS: 26.1% ± 4.8% vs. 46.1% ± 4.5%, P = 0.001). Patients with a Curie score of 1 or 2 after induction (n = 41) had an EFS similar to that of patients with a Curie score of 0 (n = 144) (3-y EFS: 40.5% ± 8.1% vs. 46.1% ± 4.5%, P = 0.40). mIBG avidity isolated to soft-tissue disease alone (n = 23) after induction was associated with a 3-y EFS of 37.7% ± 10.5%.

(A) EFS by Curie score (≤2 vs. >2) after induction (P < 0.001), based on Youden index determination of optimal cut-point. (B) EFS by Curie score (0 vs. >0) after induction (P = 0.003), for patients with MYCN-amplified tumors.
The impact of postinduction Curie scores on outcome was examined relative to MYCN gene status. MYCN status was available in 191 of the 237 (81%) patients with postinduction mIBG scans, with MYCN amplification present in 71 of the 191 cases and nonamplification present in 120. When the optimal cut-point of 2 was used, the 3-y EFS for patients with MYCN-amplified disease was significantly greater for patients with Curie scores ≤ 2 (n = 65) versus >2 (n = 6) after induction (44.2% ± 6.9% vs. 0.0%, P < 0.001). Likewise, the 3-y EFS for patients with non–MYCN-amplified disease was significantly greater for those patients with Curie scores ≤ 2 (n = 90) versus >2 (n = 30) (50.6% ± 5.5% vs. 20.8% ± 8.0%, P = 0.001). For patients with MYCN-amplified disease in particular, the presence of any mIBG avidity (Curie score > 0) after induction (n = 17) was associated with a significantly worse EFS when compared with patients who were mIBG-negative (n = 54) at that time point (3-y EFS: 11.8% ± 7.8% vs. 49.6% ± 7.7%, P = 0.003) (Fig. 5B).
EFS was affected by the relative change in Curie score, from diagnosis to after induction. Patients with ≥50% reduction in Curie score from diagnosis to after induction (n = 194) had significantly improved EFS when compared with those with <50% reduction (n = 43) (3-y EFS: 42.9% ± 3.8% vs. 17.3% ± 5.9%, P < 0.001). Similar EFS findings were noted when a ≥75% reduction in Curie score was assessed (3-y EFS: 44.4% ± 4.0% [n = 183] vs. 17.4% ± 5.3% [n = 54], P < 0.001). However, the presence of a Curie score > 2 after induction continued to carry prognostic significance, even when taking into consideration the relative change in Curie scores. Survival remained poor for patients with Curie scores > 2 after induction, regardless of whether a ≥50% (n = 16) or <50% (n = 36) reduction in scores (3-y EFS: 18.8% ± 12.0% vs. 13.9% ± 5.8%, P = 0.508) was noted (diagnosis to after induction). Similar results were noted when a 75% score reduction (3-y EFS: 22.9% ± 19.6 vs. 14.0% ± 5.3%, P = 0.571) was examined.
A backward-selected Cox model in terms of EFS with a cutoff of 2 after induction indicated that Curie score and ploidy were predictive of EFS, with Curie score values > 2 and diploid tumors corresponding to an increase in the risk of event of 2.473 (n = 187; P < 0.001) and 1.538 (P = 0.025), respectively. The order of removal was age, histologic grade, mitosis-karyorrhexis index, and MYCN status, with the least statistically significant term dropping out at each step.
After Transplantation
The optimum cut-point after transplantation, determined by maximizing the Youden index, was a Curie score of 0. Patients with a Curie score > 0 after transplantation (n = 45) had a significantly worse EFS in comparison to those patients with Curie scores of 0 (3-y EFS: 28.9% ± 6.8% vs. 49.3% ± 4.9% [n = 133], P = 0.009) (Fig. 6).

EFS by Curie score (0 vs. >0) after transplantation (P = 0.009), based on Youden index determination of optimal cut-point.
MYCN gene status was available in 140 of the 178 (79%) patients with posttransplantation mIBG scans. In contrast to after induction, none of the outcome comparisons by Curie score were statistically significant when stratified by MYCN status. For patients with MYCN-amplified disease, EFS was similar for patients with Curie scores > 0 versus 0 (3-y EFS: 37.5% ± 17.1% [n = 8] vs. 45.5% ± 8.7% [n = 44], P = 0.618).
Relative scores were also determined according to percentage reduction in Curie score from diagnosis to after transplantation. Only the outcome comparison for EFS with a ≥75% reduction (n = 152) was statistically significant when compared with those with a <75% reduction (n = 26) (3-y EFS: 47.1% ± 4.5% vs. 26.9% ± 8.7%, P = 0.014).
Impact of Chimeric Anti-GD2 Antibody Therapy
Though all patients received therapy on a uniform protocol (COG A3973), 46 were additionally treated with chimeric anti-GD2 antibody (ch14.18) on COG ANBL0032, on completion of COG A3973 therapy. For patients with Curie scores ≤ 2 after induction, the 3-y EFS for those patients subsequently treated with chimeric antibody (n = 39) was similar to that of the patients (n = 146) not receiving antibody (3-y EFS: 48.7% ± 8.0% vs. 43.9% ± 4.5%, P = 0.526). The sample size was too small to identify differences in outcome for patients with Curie scores > 2 after induction, when based on subsequent treatment with or without chimeric antibody.
DISCUSSION
In the current study, the quantitative assessment of mIBG scintigraphy after induction chemotherapy was strongly associated with outcome in children with stage 4, mIBG-avid, high-risk neuroblastoma. The presence of a Curie score > 2 after induction therapy was associated with extremely poor survival (15.4% 3-y EFS) and identified a cohort of patients at greater risk for an event, independent of other established prognostic markers. Furthermore, patients with MYCN-amplified disease had little benefit from ASCT and subsequent consolidation therapy if they exhibited any mIBG avidity (Curie score > 0) after induction. A beneficial role for ASCT in high-risk neuroblastoma has previously been reported in several cooperative group trials (1,2,31,32). On the basis of our findings, alternative therapy options should be considered for patients with Curie scores > 2 after induction, including the addition of novel agents before or during consolidation therapy.
Other studies have examined the prognostic impact of mIBG uptake at various time points during therapy, with varying results (14–22,33). Katzenstein et al. noted a similar correlation of elevated Curie score (>2) after induction and EFS in a small series of 29 patients (20). Ladenstein et al., in a large retrospective analysis of the European Bone Marrow Transplant (EBMT) registry, noted that patients with residual mIBG-avid sites after induction had inferior outcomes after subsequent ASCT (22). However, there was significant interpatient variability in therapy in this report, with patients treated over a 14-y period (1978–1992) using a wide range of induction and consolidation regimens. Similar to this EBMT report, we confirmed the finding that patients with residual mIBG-avid disease (Curie score > 0) after induction therapy have inferior outcomes after subsequent consolidation therapy. In comparison to the EBMT report, a strength of our current study is the use of a common induction and consolidation regimen, with patients treated using a single COG high-risk neuroblastoma study.
The effectiveness of anti-GD2 chimeric antibody (ch14.18) in the management of high-risk neuroblastoma has been reported by Yu et al. (4), with current high-risk neuroblastoma studies advocating ch14.18 as posttransplantation maintenance therapy. Whether the agent is most effective in the management of patients with low tumor burdens (minimal residual disease) is under consideration. In the current analysis, minimal residual disease may be defined as the presence of a low Curie score (≤2) after induction. Our data suggest that chimeric antibody did not affect survival in patients with low Curie scores (≤2) after induction, with no differences in 3-y EFS identified in those treated with or without chimeric antibody. The data should be interpreted with caution, however, given the retrospective nature of this study and potential patient–investigator bias whether to enroll patients onto COG ANBL0032 (randomized chimeric antibody study) after completion of COG A3973 therapy. The effectiveness of chimeric antibody therapy in patients with low (or high) Curie scores after induction will be examined in future COG studies in which larger populations of patients are treated with chimeric antibody therapy.
Similar to prior reports, non–mIBG-avid disease was noted in 10% of patients (280/309) with stage 4 disease who were enrolled on COG A3973 (8–13). The improved survival in patients with stage 4, non–mIBG-avid disease at diagnosis was surprising, with EFS nearly 20% higher in non–mIBG-avid than mIBG-avid tumors (P = 0.033). A formal demographic and outcome comparison for patients treated on COG A3973 with mIBG-negative versus mIBG-positive disease at diagnosis is under examination.
Previous studies have noted that relative scores, determined by the percentage change in Curie score from diagnostic to postdiagnostic scans, carried prognostic significance (14,15). In our current study, however, the impact of relative scores was mitigated in patients who exhibited absolute Curie scores > 2 after induction, suggesting that the absolute Curie score after induction carried greater prognostic significance than relative scores at that time point. Patients with persistently elevated Curie scores (>2) after induction had inferior outcomes, regardless of whether a 50% or 75% reduction in Curie score had been noted. Thus, a patient whose Curie score decreased from 25 to 5 (diagnosis to after induction) could still be projected to have a poor outcome. Historically, International Neuroblastoma Response Criteria have been used to assess response to therapy (23). On the basis of these criteria, for example, a partial response to therapy was historically defined as a >50% reduction in the number of mIBG-avid sites, nonresponsive disease a <50% reduction in the number of mIBG-avid sites, and progressive disease the development of any new mIBG-avid disease. Our current study may ultimately affect future neuroblastoma response definition, with mIBG response potentially defined by an absolute Curie score at specified time points.
The Curie scoring for our study was performed by a central scan review, without knowledge of patient response or outcome. The reproducibility of Curie scoring at local and regional centers will become paramount if this scoring method is to be included in risk-group stratification in future clinical trials. A prospective COG study is currently being developed to address this issue.
A prognostic marker is most valuable when effective therapy can be administered using that prognostic marker. For patients with Curie scores > 2 after induction, current options are limited. The use of therapeutic doses of 131I-mIBG as an adjunct to ASCT, either incorporated directly into the ASCT conditioning regimen or administered at a separate time point, has been reported to have therapeutic potential (34–40). To date, therapeutic doses of 131I-mIBG have been primarily used in patients with refractory or relapsed disease, with response rates of 30%–40% noted (39). The use of 131I-mIBG therapy during induction or consolidation therapy is now a potential option for high-risk patients. Other approaches may include the introduction of novel biologic or immunomodulatory agents that may be active against mIBG-avid, chemotherapy refractory disease.
CONCLUSION
mIBG scoring is a useful tool to predict outcome for patients with mIBG-avid, stage 4 neuroblastoma. In particular, patients with Curie scores > 2 after induction may be considered for alternative therapeutic options. The results of these data will undergo validation in upcoming COG high-risk neuroblastoma studies and cross-validation in related European neuroblastoma trials.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study was supported in part by the Elaine and Leland Blatt Foundation and NIH grants U10 CA98413, U10 CA98543, and U10 CA29511. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Thomas J. FitzGerald and staff at the Quality Assurance Review Center (QARC), especially Deirdre Logan, Sandy Kessel, and Fran Laurie, for their tremendous support of this project.
Footnotes
Published online Feb. 25, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication September 6, 2012.
- Accepted for publication November 5, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Exceptional response to the ALK and ROS1 inhibitor lorlatinib and subsequent mechanism of resistance in relapsed ALK F1174L-mutated neuroblastoma
- EVALUATION OF THE EFFECT OF MESENCHYMAL STEM CELLS ON CHEMOTHERAPY RESPONSE FOR NEUROBLASTOMA TREATMENT IN AN EXPERIMENTAL ANIMAL MODEL
- A Phase II Trial of Hu14.18K322A in Combination with Induction Chemotherapy in Children with Newly Diagnosed High-Risk Neuroblastoma
- Antitumor Activity and Tolerability of hu14.18-IL2 with GMCSF and Isotretinoin in Recurrent or Refractory Neuroblastoma: A Children's Oncology Group Phase II Study
- Validation of Postinduction Curie Scores in High-Risk Neuroblastoma: A Childrens Oncology Group and SIOPEN Group Report on SIOPEN/HR-NBL1
- Expression of Five Neuroblastoma Genes in Bone Marrow or Blood of Patients with Relapsed/Refractory Neuroblastoma Provides a New Biomarker for Disease and Prognosis
- Norepinephrine Transporter as a Target for Imaging and Therapy
- A Metastatic Mouse Model Identifies Genes That Regulate Neuroblastoma Metastasis
- Assessment of Primary Site Response in Children With High-Risk Neuroblastoma: An International Multicenter Study
- Neuroblastoma mRNAs Predict Outcome in Children With Stage 4 Neuroblastoma: A European HR-NBL1/SIOPEN Study