


Article Figures & Data
Figures
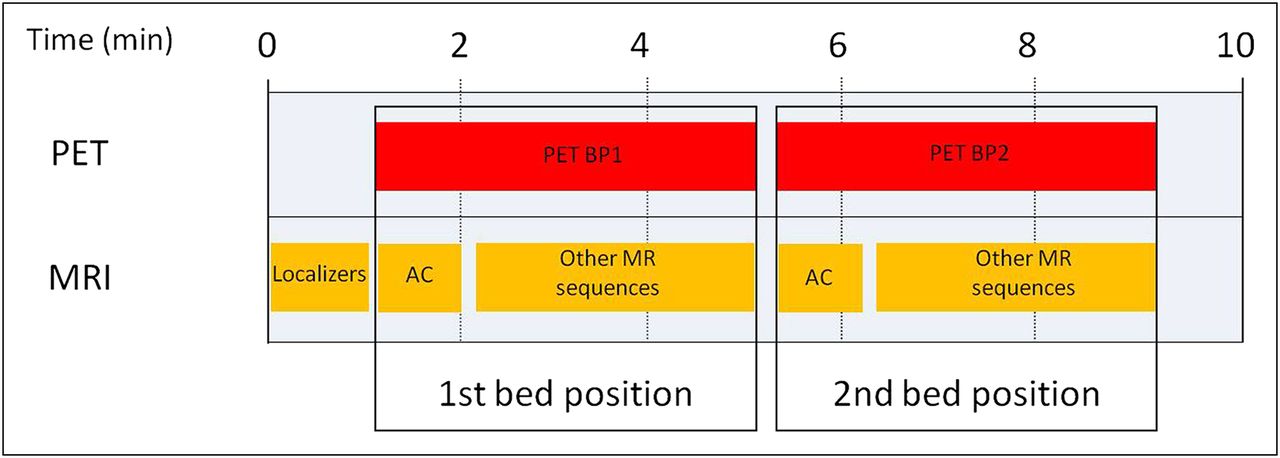
- FIGURE 1.
Diagram of basic acquisition protocol covering 2 bed positions in combined PET/MRI. For each PET bed position (4-min acquisition time in example), MRI AC sequence is acquired first and then MRI component can be used for further acquisitions without moving patient bed. BP1 = bed position 1; BP2 = bed position 2.
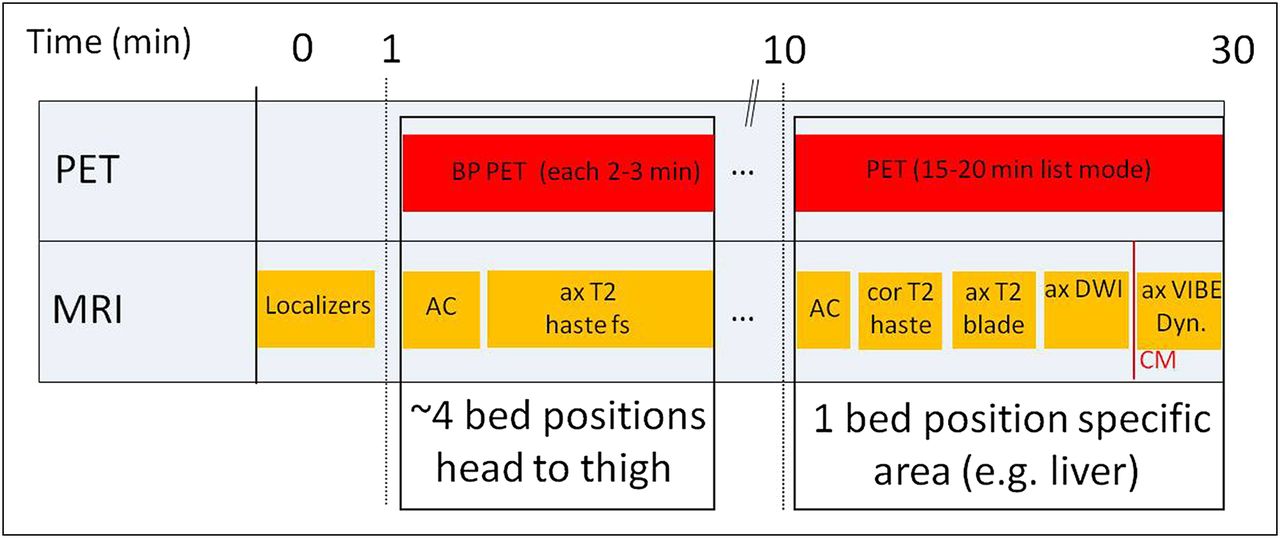
- FIGURE 2.
Diagram of acquisition protocol for combined PET/MRI focusing on single area of interest (in this example, liver imaging), with only limited MRI evaluation of partial or whole body. ax = axial; BP = bed position; cor = coronal; CM = contrast medium; DWI = diffusion-weighted imaging; Dyn. = dynamic; fs = fat-saturated.
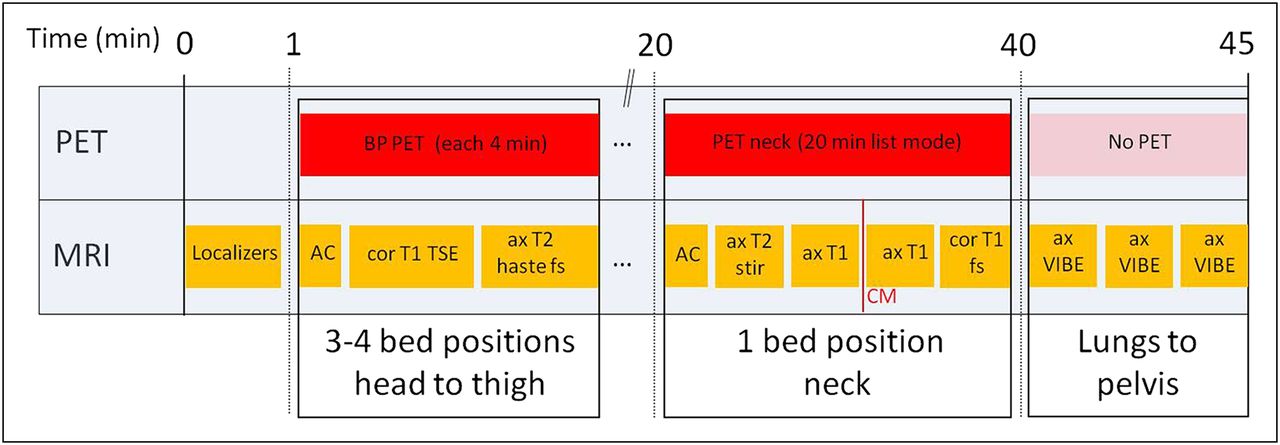
- FIGURE 3.
Diagram of acquisition protocol focusing on head-and-neck imaging in combined PET/MRI with full diagnostic coverage of partial or whole body. ax = axial; BP = bed position; cor = coronal; CM = contrast medium; fs = fat-saturated.
- FIGURE 4.
Example of head-and-neck imaging in combined PET/MRI (18F-FDG): patient with cancer of oral cavity. (A–C) Coronal T1-weighted turbo spin echo, axial PET, and axial T2-weighted fat-saturated HASTE images show no distant metastases. (D and E) T2-weighted hyperintense lesion on MRI with high glucose metabolism on right side in frontal oral cavity is suggestive of tumor.
- FIGURE 5.
Diagram of acquisition protocol focusing on prostate imaging in combined PET/MRI with full diagnostic coverage of partial or whole body. ax = axial; BP = bed position; cor = coronal; CM = contrast medium; fs = fat-saturated.
- FIGURE 6.
Example of prostate imaging in combined PET/MRI (11C-choline): patient with radical prostatectomy and PSA recurrence. (A–C) Coronal T1-weighted turbo spin echo, axial PET, and axial T2-weighted fat-saturated HASTE images show no distant metastases. (D) Axial T2-weighted turbo spin echo image provides superb anatomic details of area of former prostate fossa. (E) Dynamic contrast-enhanced MR image shows early intense contrast enhancement in arterial phase. (F) In fused 11C-choline PET image, moderate focal high uptake is found in corresponding region. (G) Parametric map indicating area under curve confirms early and intense enhancement of suspected lesion.
- FIGURE 7.
Diagram of acquisition protocol focusing on liver imaging in combined PET/MRI with full diagnostic coverage of partial or whole body. ax = axial; BP = bed position; cor = coronal; CM = contrast medium; DWI = diffusion-weighted imaging; Dyn. = dynamic; fs = fat-saturated.
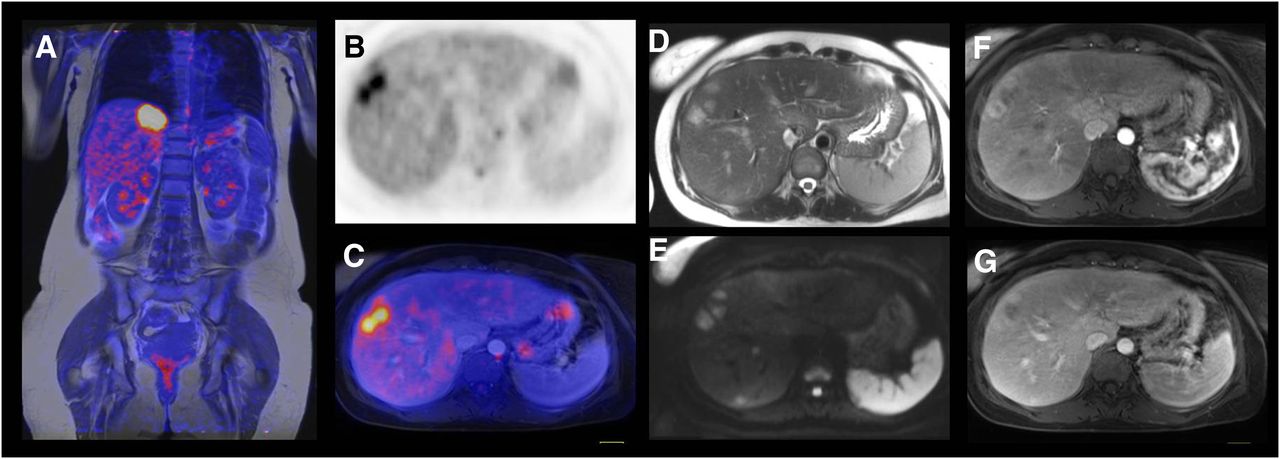
- FIGURE 8.
Example of liver imaging in combined PET/MRI (18F-FDG): patient with breast cancer and liver metastases. (A) Fused coronal T1-weighted turbo spin echo image with PET image shows hypermetabolic lesion in liver below medial part of diaphragm. (B and C) Axial PET image and axial fused image outline 2 adjacent liver metastases in right lobe. (D–G) Axial morphologic MR images (T2-weighted HASTE [D], diffusion-weighted [E], dynamic contrast-enhanced [F and G]) demonstrate high soft-tissue contrast on MRI and superb anatomic delineation of liver metastases.
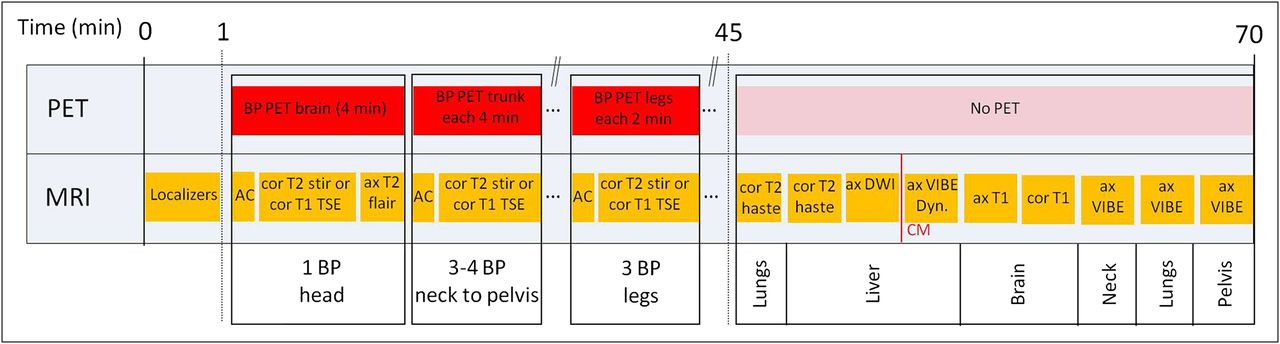
- FIGURE 9.
Diagram of fully diagnostic whole-body acquisition protocol in combined PET/MRI. ax = axial; BP = bed position; cor = coronal; CM = contrast medium; DWI = diffusion-weighted imaging; Dyn. = dynamic; fs = fat-saturated; stir = short-τ inversion recovery.
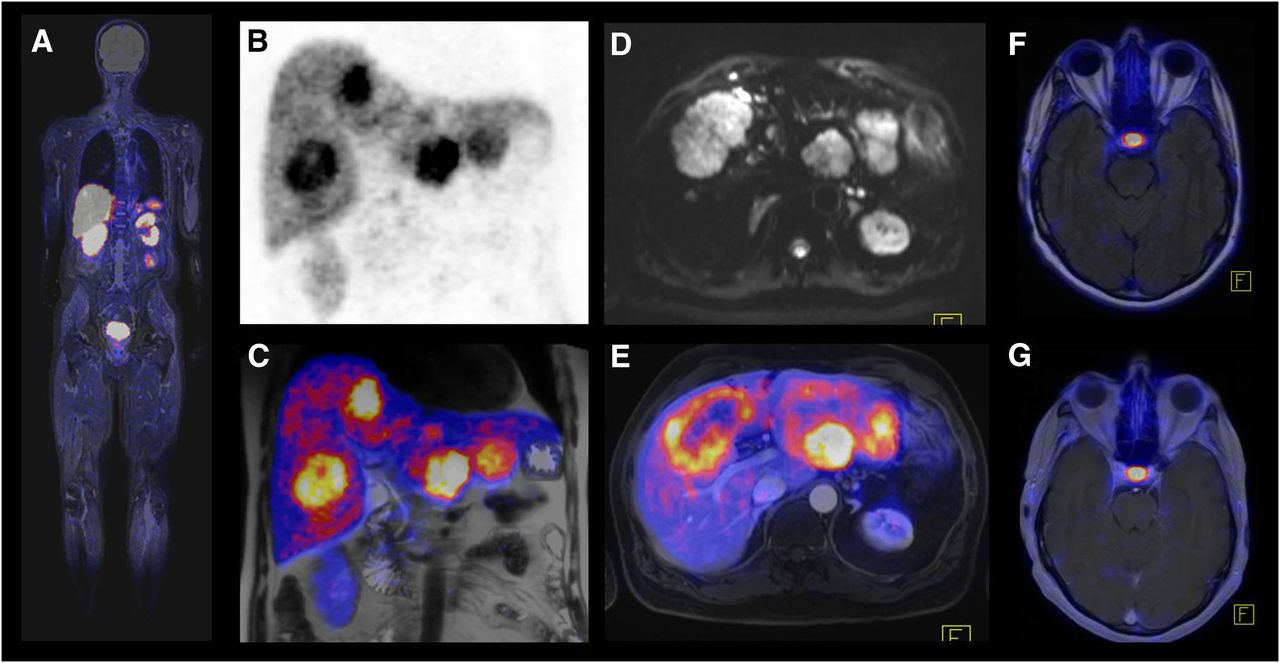
- FIGURE 10.
Example of whole-body imaging in combined PET/MRI (68Ga-DOTATOC): patient with neuroendocrine cancer and liver metastases. (A) Fused coronal T2-weighted short-τ inversion recovery and PET images demonstrate whole extent of examination. Because of incomplete coverage of lower legs by total-imaging-matrix surface coils, intensity and quality of MRI images in this area are substantially reduced. (B and C) PET and fused images show multiple liver metastases with high somatostatin receptor expression. (D) Diffusion-weighted image (with b-value of 50 s/mm2) shows large metastasis with many surrounding small lesions. (E) In comparison to diffusion-weighted image, fused axial T2-weighted fat-saturated HASTE and PET image demonstrates that small lesions are not visible on PET. (F and G) Fused axial T2-weighted fluid-attenuated inversion recovery image and axial T1-weighted gadolinium-enhanced image show physiologic uptake of hypophysis and no evidence of brain metastases.
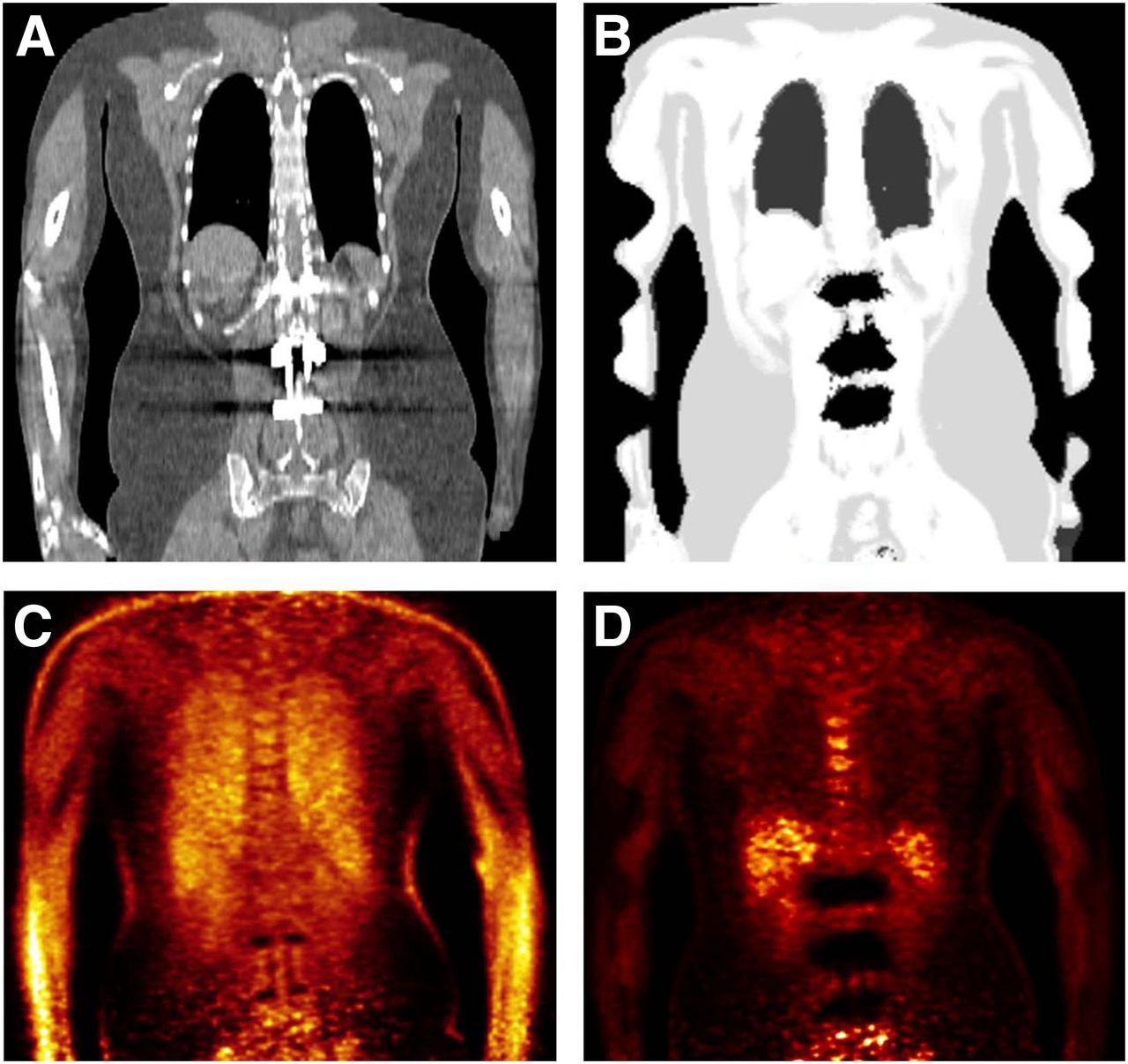
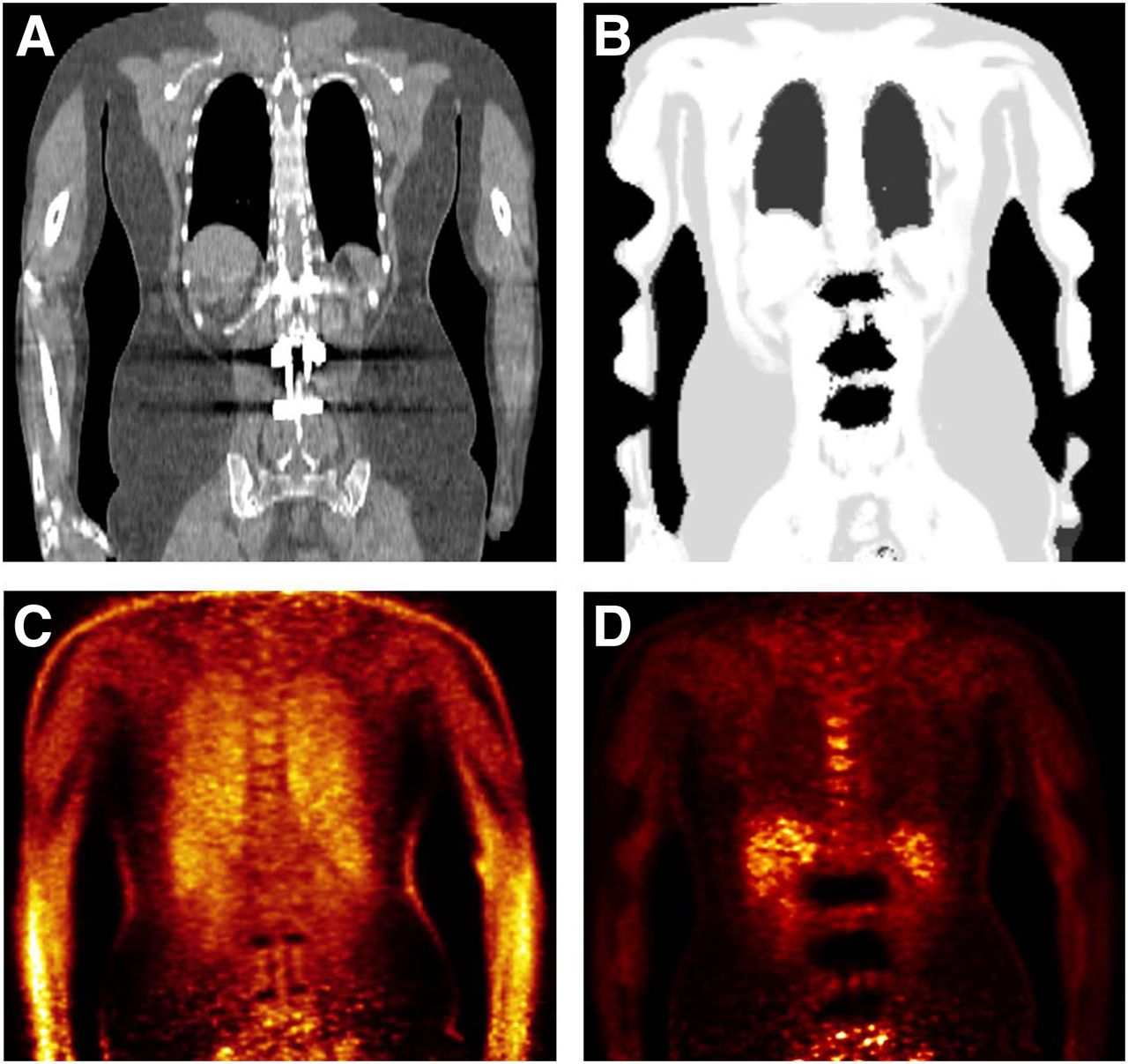
- FIGURE 11.
Patient with metallic implants from lumbar spine surgery. Metallic artifacts in CT image (A) result in region’s being incorrectly segmented as air in MRI-based attenuation map (B). Non-AC PET image (C) shows normal tracer distribution around implants, but MRI-based AC leads to large areas of underestimated uptake (D).
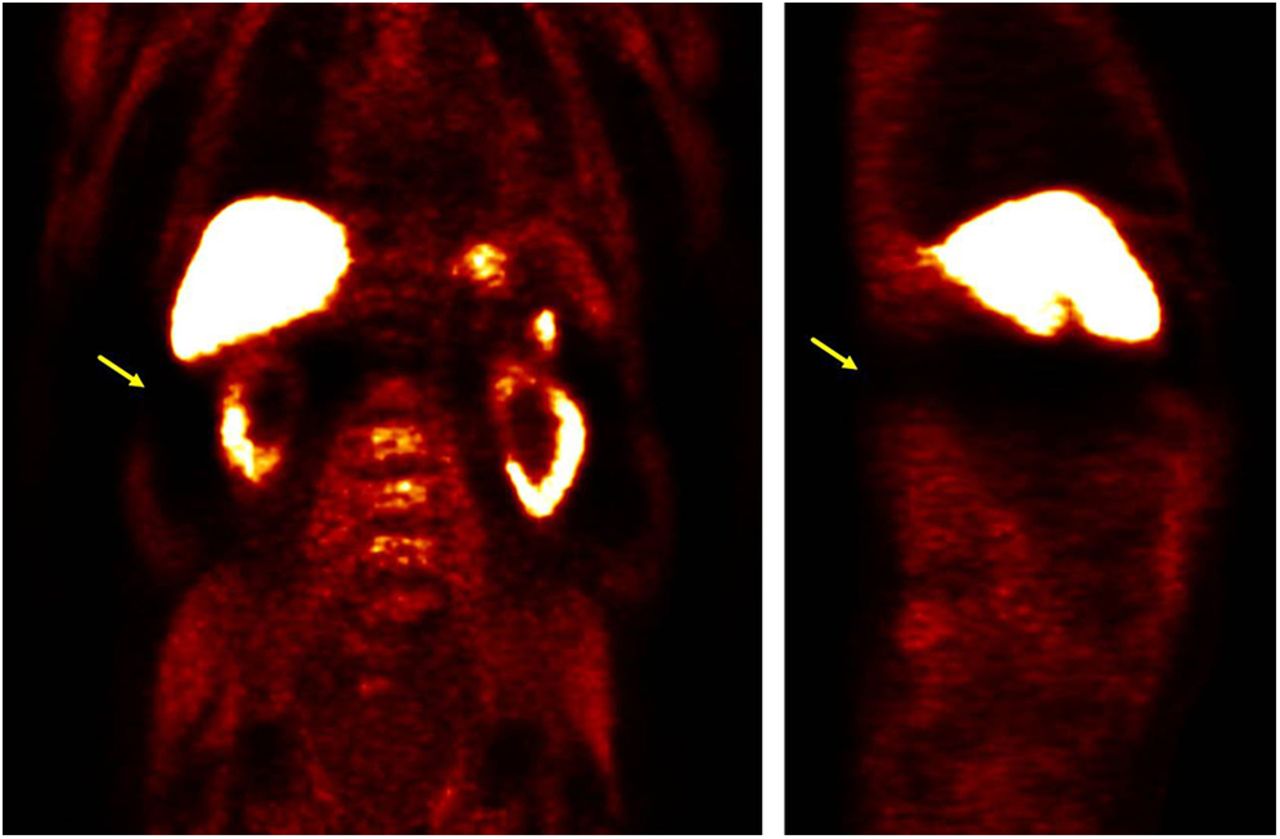
- FIGURE 12.
MRI-based attenuation map (top row) and corresponding 18F-FDG PET images (bottom row) acquired arms-down showing truncation in arms and resulting artifacts: inhomogeneity in liver (anterior–posterior gradient, yellow arrows) and sharp change in uptake in arms corresponding to limit of field of view (blue arrows).
- FIGURE 13.
Severe artifacts in 11C-choline PET images acquired arms-down. Truncation of attenuation map can occasionally lead to biased scatter correction, which renders complete regions unevaluable (yellow arrows).








Tables
- TABLE 1
Technical Aspects and Differences between PET and MRI Relevant for Optimizing Protocols in Integrated PET/MRI
PET MRI Patient schedule Rigorous patient schedule Flexible patient schedule Acquisition at fixed time after injection Additional imaging possible, depending on findings or motion High predictability of acquisition time Prescan preparation Tracer administration Checking of potential contraindications and renal insufficiency when gadolinium is used Resting of patient during uptake time Removal of all metal With 18F-FDG, previous fasting and glucose level measurement In-bed patient preparation Very fast; only uploading of patient onto table Placement of surface coils and headphones Radiation exposure for staff while near patients Time-consuming (3–5 min) Field of view 45–60 cm transaxially 35–45 cm transaxially 15–21 cm axially Up to 50 cm axially Planning Straightforward Experience for fine-tuning Defining of field of view and time per bed position Planning throughout scan Planning by operator at start, with no further interaction Frequent interaction with radiologist Often oblique plane acquisitions Acquisition Step and shoot Isocenter for optimal image quality Overlapping of beds Occasional need for bed motion even in examination of single organs Respiratory motion Production of blurring Frequent production of artifacts Possibility of respiratory gating; increase of acquisition time to preserve image quality Possibility of breath-hold acquisition or respiratory gating Region Sequence Image plane Slice thickness (mm) Gap (%) Slices (no.) Acquisition time (min:s) TR/TE Matrix Field of view (mm) Resolution (mm2) GRAPPA Breath hold Remarks AC Whole body 3D T1 VIBE Dixon Coronal 3.12 0 128 0:19 3.60/1.23–2.46* 192 × 121 500 4.1 × 2.6 2 + MRI-based AC Diagnostic sequences for whole-body coverage Whole body T1 TSE Coronal 5 30 25–36 1:11 600/8.7 384 × 230 450 2.0 × 1.2 2 + for chest, abdomen Whole body T2 STIR Coronal 5 30 25–36 1:25–3:15† 7.9/500 259 × 384 450 2.9 × 1.8 3 Free breathing Diagnostic sequences for partial-body coverage Partial body T2 HASTE fat sat Axial 5 20 25 1:08 1,600/95 320 × 260 380 1.5 × 1.2 2 Free breathing Partial body = chest to pelvis, dark-blood pulse Lungs 3D VIBE + CM Axial 4 0 72 0:18 3.24/1.23 320 × 240 400 1.7 × 1.3 2 + 11% slice oversampling Abdomen to pelvis 3D VIBE + CM Axial 5 0 44 0:16 3.29/1.16 320 × 260 460 1.8 × 1.4 2 + Two stacks; 45% slice oversampling Prostate cancer recurrence Prostate T2 TSE Axial 3 20 31 4:47 4,610/101 320 × 310 200 0.6 × 0.6 2 – Prostate DWI Axial 3.6 0 20 5:39 4,500/93 160 × 120 260 2.2 × 1.6 2 – b = 50, 400, 800 s/mm2 Prostate 3D TWIST Axial 3.6 0 20 5:24 4.83/1.87 192 × 132 260 2.0 × 1.4 2 – DCE; temporal resolution, 4.25 s Primary staging of ENT tumors Neck T1 TSE ± CM Axial 4.0 20 30 3:46 1,330/10 384 × 384 230 0.6 × 0.6 2 – Each sequence before and after CM Neck T2 STIR Axial 4.0 20 30 3:48 5,810/54 320 × 320 230 0.7 × 0.7 2 – Neck T1 TSE fat sat + CM Coronal 4.0 20 20 3:37 1,290/9.6 320 × 320 230 0.7 × 0.7 2 – Neck T2 STIR Sagittal 4.0 2 28 4:11 5,090/57 384 × 345 240 0.7 × 0.6 2 – Focus on potential liver metastases Liver T2 HASTE Coronal 5.0 20 30 0:42 1,400/96 256 × 256 380 1.5 × 1.5 3 + Liver T2 HASTE fat sat Axial 5.0 20 35 1:08 1,600/95 320 × 260 380 1.5 × 1.2 2 + Liver DWI Axial 5.0 20 35 5:04 7,800/82 192 × 144 380 2.6 × 2.0 2 Free breathing b = 50, 400, 800 s/mm2 Liver VIBE Axial 3.0 20 64 0:18 4.06/1.91 320 × 240 380 1.6 × 1.2 2 + DCE: without CM, arterial, portal-venous, late phase; 13% slice oversampling Diagnostic whole-body protocol‡ Brain T2 FLAIR Axial 4.0 30 25 2:08 9,000/85 256 × 192 220 1.1 × 0.9 2 – Brain T1 GRE +CM Axial 4.0 30 25 2:10 250/2.48 320 × 256 220 0.9 × 0.7 — – Brain T1 GRE +CM Coronal 4.0 30 35 1:25 250/2.48 320 × 256 220 0.9 × 0.7 — – Lungs T2 HASTE Coronal 8.0 30 30 0:22 650/28 320 × 256 400 1.6 × 1.3 3 + Liver DWI Axial 5.0 20 35 4:08 9,200/85 192 × 144 380 2.6 × 2.0 2 Free breathing b = 50, 800 s/mm2 Neck VIBE Dixon Axial 4.0 20 36 0:28 5.61/2.46–3.69 320 × 260 400 1.5 × 1.3 2 – 44% slice oversampling ↵* Fat saturation techniques with Dixon require 2 repetition times.
↵† Acquisition time is dependent on number of averages and slices per slab specific for different body regions (3–5).
↵‡ Only sequences not part of other protocols are mentioned.
3D = 3-dimensional; b = b-value; BLADE = noncartesian k-space data acquisition for motion correction in TSE sequences; CM = contrast medium; DCE = dynamic contrast enhanced; DWI = diffusion-weighted imaging; FLAIR = fluid-attenuated inversion recovery; GRAPPA = generalized autocalibrating partially-parallel acquisition (as integrated parallel-acquisition technique [iPAT; Siemens Healthcare]); GRE = gradient echo; sat = saturation; STIR = short-τ inversion recovery; TE = echo time; TR = repetition time; TSE = turbo spin echo; TWIST = dynamic contrast-enhanced sequence with k-space sharing.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Concurrent Respiratory Motion Correction of Abdominal PET and Dynamic Contrast-Enhanced-MRI Using a Compressed Sensing Approach
- New Approaches to Molecular Imaging of Multiple Myeloma
- Techniques, Benefits, and Challenges of PET-MR
- Motion Correction Strategies for Integrated PET/MR
- Diagnostic Value of Diffusion-Weighted Imaging in Simultaneous 18F-FDG PET/MR Imaging for Whole-Body Staging of Women with Pelvic Malignancies
- Radiotracer Dose Reduction in Integrated PET/MR: Implications from National Electrical Manufacturers Association Phantom Studies
- Workflow Considerations in PET/MR Imaging
- Principles of PET/MR Imaging
- Performance of Whole-Body Integrated 18F-FDG PET/MR in Comparison to PET/CT for Evaluation of Malignant Bone Lesions
- Implementation and Performance Evaluation of Simultaneous PET/MR Whole-Body Imaging with Continuous Table Motion
- Monocyte-Directed RNAi Targeting CCR2 Improves Infarct Healing in Atherosclerosis-Prone Mice
- PET and MR Imaging: The Odd Couple or a Match Made in Heaven?