


Abstract
The aim of this study is to evaluate the incremental staging information, management impact, and prognostic stratification of PET/CT in the primary staging of esophageal cancer in a cohort of patients with mature survival data. Methods: Between July 2002 and June 2005, 139 consecutive patients with newly diagnosed esophageal cancer underwent conventional staging investigations (CSI), followed by PET/CT. Disease stage was classified according to the American Joint Committee on Cancer staging system (6th edition) and grouped as stage I–IIA, stage IIB–III, and stage IV reflecting broad groupings that determine therapeutic choice. Validation of results was performed when PET/CT and CSI stage groups were discordant and in those patients where PET/CT changed management. Management impact was determined by comparing prospectively recorded pre-PET/CT management plans with post-PET/CT management plans. Survival after follow-up of at least 5 y in patients was analyzed using the Kaplan–Meier product limit method and the Cox proportional hazards regression model. Results: PET/CT changed the stage group in 56 of 139 (40%) patients and changed management in 47 of 139 (34%) patients. In 22 patients, therapy was changed from curative to palliative and in 3 from palliative to curative; in 11, treatment modality was changed without a change in treatment intent, and in 11 the delivery of therapy or diagnostic procedure was changed. Of the 47 patients with management change, imaging results could be validated in 31 patients, and PET/CT correctly changed management in 26 (84%) of these. Of the remaining 5 patients, CSI stage was also incorrect in 4 and correct in 1. Median survival was 23 mo. PET/CT stages I–IIA, IIB–III, and IV had a 5-y survival of 40%, 38%, and 6%, respectively. Post-PET/CT stage group and treatment intent were both strongly associated with survival (P < 0.001). Conclusion: PET/CT provides incremental staging information compared with CSI, changes management in one third of patients, and has powerful prognostic stratification in the primary staging of esophageal cancer.
Esophageal cancer is a deadly disease with more than 50% of patients having unresectable or metastatic disease at the time of presentation (1). Recent data from the Surveillance Epidemiology and End Results database indicate an age-adjusted incidence rate of 4.5 per 100,000 men and women per year and an age-adjusted death rate of 4.3 per 100,000 men and women per year (2). The 5-y relative survival for patients diagnosed with esophageal cancer between 2001 and 2007 was 37.3% for those without nodal involvement, but this represented less than a quarter of all patients (2). For the 32% of patients presenting with regional nodal involvement, the 5-y survival fell to 18.4%, whereas the 5-y survival for the 32% of patients with documented metastatic disease was only 3.1% (2). Therefore, disease stage has profound prognostic implications.
For those with early-stage resectable esophageal tumors, curative treatment options include surgery or definitive chemoradiation in patients with significant medical comorbidities. However, in locally advanced disease, neoadjuvant chemotherapy or chemoradiation is often used in combination with surgery in an attempt to augment the poor survival rates. Despite improvements in perioperative care, esophagectomy still has significant morbidity and mortality risks (3). Given these risks, patients with medical comorbidities or more advanced locoregional disease may be considered for definitive treatment with chemoradiation alone whereas patients with metastatic disease require strategies that provide the best chance of ameliorating symptoms and maintaining quality of life. Therefore, accurate tumor staging is essential in directing patients to appropriate surgical or multimodality therapies, particularly in patients with locally advanced disease who have high a priori likelihood of remote nodal or distant metastatic disease that precludes curative treatment attempts.
Noninvasive imaging techniques play an important role in the staging of esophageal cancer patients. Conventional staging investigations (CSI) include dedicated CT scans and endoscopic ultrasound (EUS). EUS can assess the extent of mucosal involvement and peritumoral nodal metastases but is constrained in locally advanced cases in which passage of the endoscope may not be possible. Dedicated CT scans can assess local invasion of adjacent mediastinal structures as well as regional nodal enlargement and metastatic disease. However, this technique has been shown to be less sensitive for detection of regional nodal and distant metastatic disease, compared with 18F-FDG PET, which has been shown to be of incremental value in the primary staging of esophageal cancer (4–14). PET provides more accurate staging, provides more accurate prognostic stratification, and can change management in more than one third of patients (4,6). PET does, however, have limitations in the assessment of the primary tumor and particularly in the detection of peritumoral nodal disease (7,9,11,13).
Over the past decade, PET/CT has become established in cancer imaging, allowing the functional information of PET to be fused with the anatomic information from CT. Several studies have reported PET/CT to be more accurate than either PET alone or CSI in assessing locoregional lymph nodes and in detecting distant metastatic disease (15–23). Given the importance of disease stage to treatment choice, this superior accuracy is likely to have a high impact on management decisions. In addition, it is therefore likely that PET/CT will provide powerful prognostic stratification in the primary staging of esophageal cancer. However, few studies have been reported with sufficient long-term patient follow-up to demonstrate this latter capability. At the Peter MacCallum Cancer Centre, PET/CT has been routinely used in the staging of esophageal cancer patients being considered for curative treatment since 2002. Therefore, the aim of this study was to assess the incremental staging information, management impact, and prognostic stratification of PET/CT, compared with CSI, in the primary staging of patients with esophageal cancer in a cohort of patients with mature follow-up data. This study builds on our previous results using stand-alone 18F-FDG PET (6).
MATERIALS AND METHODS
Patient Population
All patients referred to the Peter MacCallum Cancer Centre between July 2002 and June 2005 for primary staging of biopsy-proven esophageal cancer with PET/CT who were potentially suitable for curative treatment were prospectively entered into a database. Patients were excluded from analysis if they had systemic metastatic disease confirmed on biopsy or unequivocally identified on CSI and were not being considered for curative treatment. The study was approved by our institutional ethics committee.
CSI
The pre-PET/CT disease stage was determined on the basis of CSI results that were obtained 0–60 d before PET/CT acquisition without intervening treatment. CSI included dedicated CT scans acquired for all patients and EUS for selected patients depending on the clinical scenario. Dedicated CT was performed of the chest, abdomen, and pelvis with intravenous contrast unless clinically contraindicated. For patients managed at the Peter MacCallum Cancer Centre, CSI results were reviewed for diagnostic quality at our institutional multidisciplinary meetings and repeated if deemed technically inadequate.
18F-FDG PET/CT
18F-FDG PET/CT scans were obtained using a dedicated PET/CT scanner (Discovery LS; GE Healthcare) incorporating a 4-slice CT component. CT images were acquired without intravenous or oral contrast, using parameters of 140 kVp and 80 mAs. CT data were used for both attenuation correction and anatomic localization. Our imaging protocol required patients to fast for 6 h before administration of 18F-FDG (5 MBq/kg, up to a maximum of 400 MBq), with blood glucose levels required to be 10 mmol/L or less. PET data were reconstructed using an ordered-subset expectation maximization algorithm. Scans were acquired from the base of skull to the upper thighs for all patients. PET/CT images were examined by a nuclear medicine physician with at least 6 mo of experience in interpreting PET/CT results at the start of the study and at least 3 y of 18F-FDG PET experience. PET/CT images were interpreted qualitatively, with sites of disease identified as 18F-FDG–avid foci in a nonphysiologic distribution of intensity typically greater than adjacent normal tissues (and particularly higher than hepatic uptake) unless the sites were of small volume, for which partial-volume effects needed to be taken into consideration. Clinical reports were issued in full knowledge of CSI results to reflect routine practice. This study, therefore, evaluated the incremental rather than the independent information provided by PET/CT.
Determination of Disease Stage
Disease stage was determined according to the sixth edition of the American Joint Committee on Cancer staging system (24). Although the sixth edition has since been updated, we used that edition because it was in clinical use at the time of patient recruitment. The pre-PET/CT stage was determined on the basis of CSI results. The post-PET/CT stage was determined on the basis of PET/CT results, except when the size of the primary tumor or peritumoral nodal disease was likely below the resolution of PET. In this event, the T stage was determined on the basis of CSI or biopsy results, and lobulation of the primary tumor on PET/CT was accepted as evidence of peritumoral nodal involvement if disease at this location was demonstrated on CSI. PET/CT and CSI results were compared using the routine clinical reports, which, once issued, were entered into a database and not reinterpreted in the light of subsequent clinical information. Equivocal CSI and PET/CT results were interpreted as not representing disease on the principle that wherever possible patients should be given the benefit of the doubt in selecting the treatment most likely to effect cure. We elected to group the disease stages into 3 broad categories: early lymph node–negative disease (stage I–IIA), locally advanced disease (stage IIB–III), and metastatic disease (stage IV). These groupings broadly influence therapeutic choices, with surgery for stage I–IIA, multimodality therapy for stage IIB–III, and palliative treatment for stage IV being the most common approaches in these groups. Stage IV disease included stage M1a patients with celiac or cervical nodal involvement of lower and upper esophageal primary tumors, respectively.
Management Impact of PET/CT
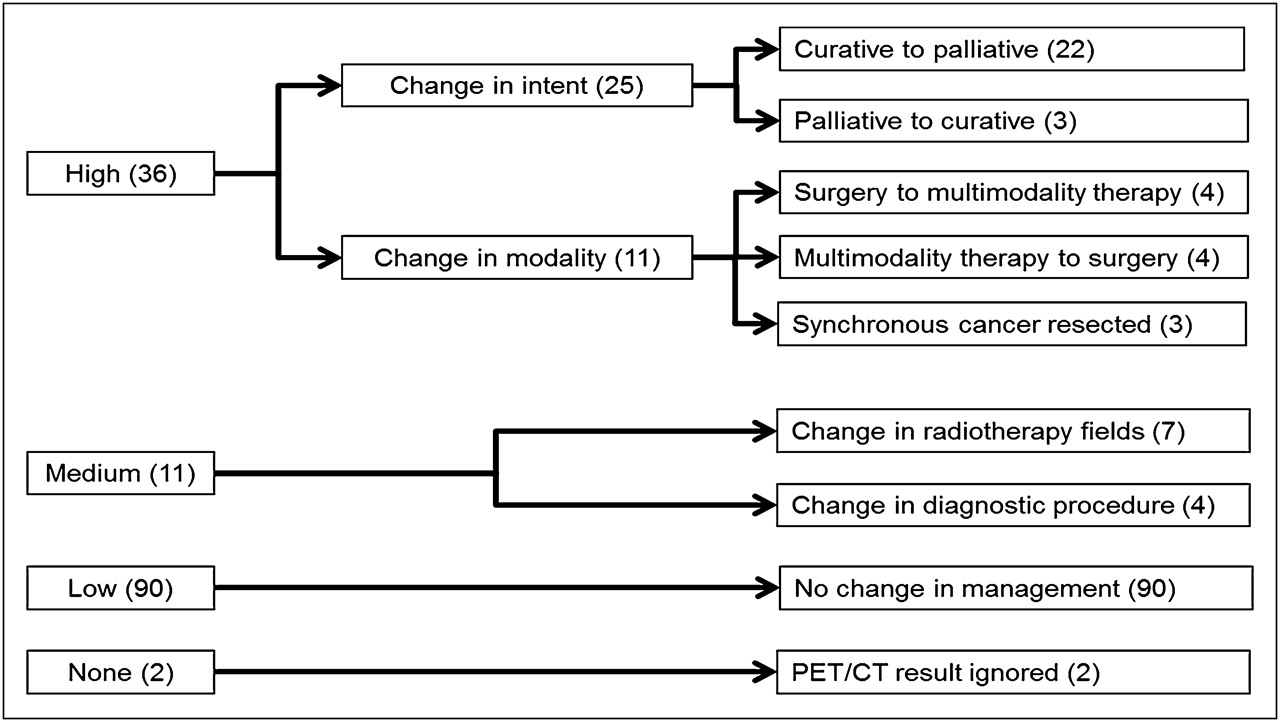
The management impact of PET/CT was assessed by comparing the prospectively recorded pre-PET/CT management plan with the post-PET/CT management plan. The post-PET/CT management plan was determined from the medical record or by direct contact with the treating clinician. The impact of PET/CT on management was based on our previously published criteria and defined as high (the treatment modality or intent was changed), medium (the treatment modality or intent remained unchanged, although the method of treatment delivery or planned diagnostic procedure was changed), low (PET/CT results were consistent with planned management, and treatment modality or intent was unchanged), or none (the management plan was not changed, despite being inconsistent with the post-PET/CT stage—that is, PET/CT results were ignored) (25).
Validation of Results
The validation of results was performed for patients with discordant PET/CT and CSI stage group and for those in whom PET/CT changed management. Validation of results was determined by correlation with pathologic or intraoperative findings. When pathologic or intraoperative evaluation was not obtained, evidence of lesion progression on serial anatomic imaging was considered as confirmation of malignant disease. When pathologic, surgical, or serial imaging was not performed, clinical outcome was used to validate imaging findings. Imaging results were considered not assessable when no further pathologic, surgical, or serial imaging was performed and clinical outcome was deemed insufficient to definitively validate results or when intervening treatment may have altered the natural history of the disease.
Follow-up
Overall survival was used as the primary endpoint to evaluate prognostic significance. Overall survival was measured from the date of the PET/CT scan to the date of death from any cause or the date of last contact, censored after 5 y of follow-up. At least 5 y of follow-up were available in all surviving patients. For patients managed at Peter MacCallum Cancer Centre, clinical follow-up was performed 3 monthly for 2 y and 6 monthly for 2–5 y after treatment. Imaging was performed only to follow-up equivocal abnormalities on staging investigations or to evaluate symptoms or signs suggestive of residual or recurrent disease. For patients managed elsewhere, follow-up was obtained through contacting the treating specialists or family physicians and collecting any biopsy or imaging results.
Statistical Methods
Kaplan–Meier curves were used to describe survival for each stage group as defined by both CSI and PET/CT. Survival based on whether curative or palliative treatment was planned after PET/CT was also analyzed. Log-rank tests were used to compare the survival curves. The Cox proportional hazards regression model was used to estimate the hazard ratios and confidence intervals. A P value less than 0.05 was considered statistically significant.
RESULTS
Patient Characteristics
A total of 139 consecutive patients underwent PET/CT for the primary staging of esophageal cancer. A summary of patient and tumor characteristics is listed in Table 1. The median age for the cohort was 67 y (range, 32–85 y). There was a predominance of adenocarcinomas, with 80 of 85 (94%) of these tumors being located in the lower third of the esophagus or at the gastroesophageal junction.
Patient and Tumor Characteristics
Comparison of Pre- and Post-PET/CT Stage
Comparison of the pre- and post-PET/CT stage groups is outlined in Table 2. There was discordance between the pre-PET/CT stage group determined by CSI and the post-PET/CT stage group in 56 of 139 patients (40%). Overall, PET/CT upstaged 37 (27%) patients and downstaged 19 (14%) patients. The percentage of discordant post-PET/CT stage groups was similar between each pre-PET/CT stage group. Of the 83 patients with unchanged CSI and PET/CT stage group, PET/CT detected additional nodal or systemic metastatic lesions in 20 patients without changing the overall stage group. Of these 20 patients, PET/CT detected additional regional or remote nodal metastases in 14 patients and upstaged 4 patients from stage IVA to stage IVB by detecting previously occult distant metastatic disease. In the remaining 2 patients, PET/CT detected additional sites of systemic metastases for patients with suspected but not definite stage IVB disease on CSI who were still being considered for curative treatment. In addition, PET/CT detected synchronous additional primary malignancies in 5 patients (3 colorectal cancers and 2 primary lung cancers).
Comparison of Pre-PET/CT and Post-PET/CT Disease Stage Groups
Validation of Imaging Results
PET/CT findings resulted in discordant stage grouping or a change in management in 75 of 139 patients (54%). Of these 75 patients, imaging findings could be validated in 44 patients (59%): by either pathologic or intraoperative findings in 20 patients (45%) or by serial imaging or clinical follow-up in 24 patients (55%). Fifty-six of these 75 patients had discordant stage grouping on PET/CT and CSI, for which imaging findings could be validated in 33 patients (59%). Of these 33 patients, PET/CT was correct in 22 (67%), CSI was correct in 4 (12%), and neither PET/CT nor CSI was correct in 7 (21%). For the 7 patients for whom neither PET/CT nor CSI was correct, PET/CT correctly excluded remote nodal or systemic metastatic disease in 3 patients and detected an additional synchronous primary malignancy in 1 patient despite false-negative assessment of low-volume periesophageal nodal disease in each of these cases. In the remaining 3 patients for whom both PET/CT and CSI were incorrect, 2 patients had underestimation of disease extent by both modalities despite being upstaged from CSI stage I–IIA to PET/CT IIB–III, and 1 patient had a false-positive lung metastasis on PET/CT while also having false-negative periesophageal nodal assessment on CSI.
Disease stage was unverifiable in 23 of 56 patients (41%) with discordant stage groupings because of therapeutic intervention of unconfirmed sites of disease visualized only on imaging (12 patients), development of nodal or systemic disease on follow-up after unsuccessful local treatment of the primary tumor (7 patients), or death before confirmation of disease stage (4 patients).
Management Impact of PET/CT
Overall, PET/CT changed management in 47 of 139 patients (34%). Of these, 36 (26%) were of high impact and 11 (8%) of medium impact. The details of the PET/CT-induced management changes are outlined in Figure 1, and an example is shown in Figure 2. Of the 47 patients in whom PET/CT changed management, the disease stage could be validated in 31 (66%), including 16 for whom there was a change in curative or palliative treatment intent. In these 16 patients, PET/CT was correct in all 14 changed from curative to palliative treatment, and PET/CT correctly excluded sites of systemic metastatic disease in the 2 patients changed from palliative to curative treatment (despite false-negative PET/CT assessment of low-volume periesophageal nodal disease in both of these patients). In the remaining 15 assessable patients with a PET/CT-induced management change, PET/CT correctly changed management in 10, predominantly because of correctly modifying the disease extent. For the other 5 patients, there was management change with incorrect PET/CT staging. Of these 5 patients, 3 patients had multimodality therapy changed to surgery after false-negative periesophageal nodal assessment on PET/CT (2 of which were also incorrectly staged with CSI), 1 patient had planned surgical therapy changed to multimodality therapy after PET/CT upstaged CSI stage I–IIA to stage IIB–III but failed to detect systemic metastatic disease, and 1 patient underwent biopsy of an 18F-FDG–avid lung lesion (confirmed to be benign on pathologic examination) before continuing with planned curative treatment. Importantly, incorrect PET/CT staging did not deny curative treatment in these 5 patients, and CSI was also incorrect in all but 1. This 1 patient with incorrect PET/CT staging and correct CSI staging had management changed from curative chemoradiotherapy to curative surgery after false-negative assessment of periesophageal nodal disease on PET/CT.

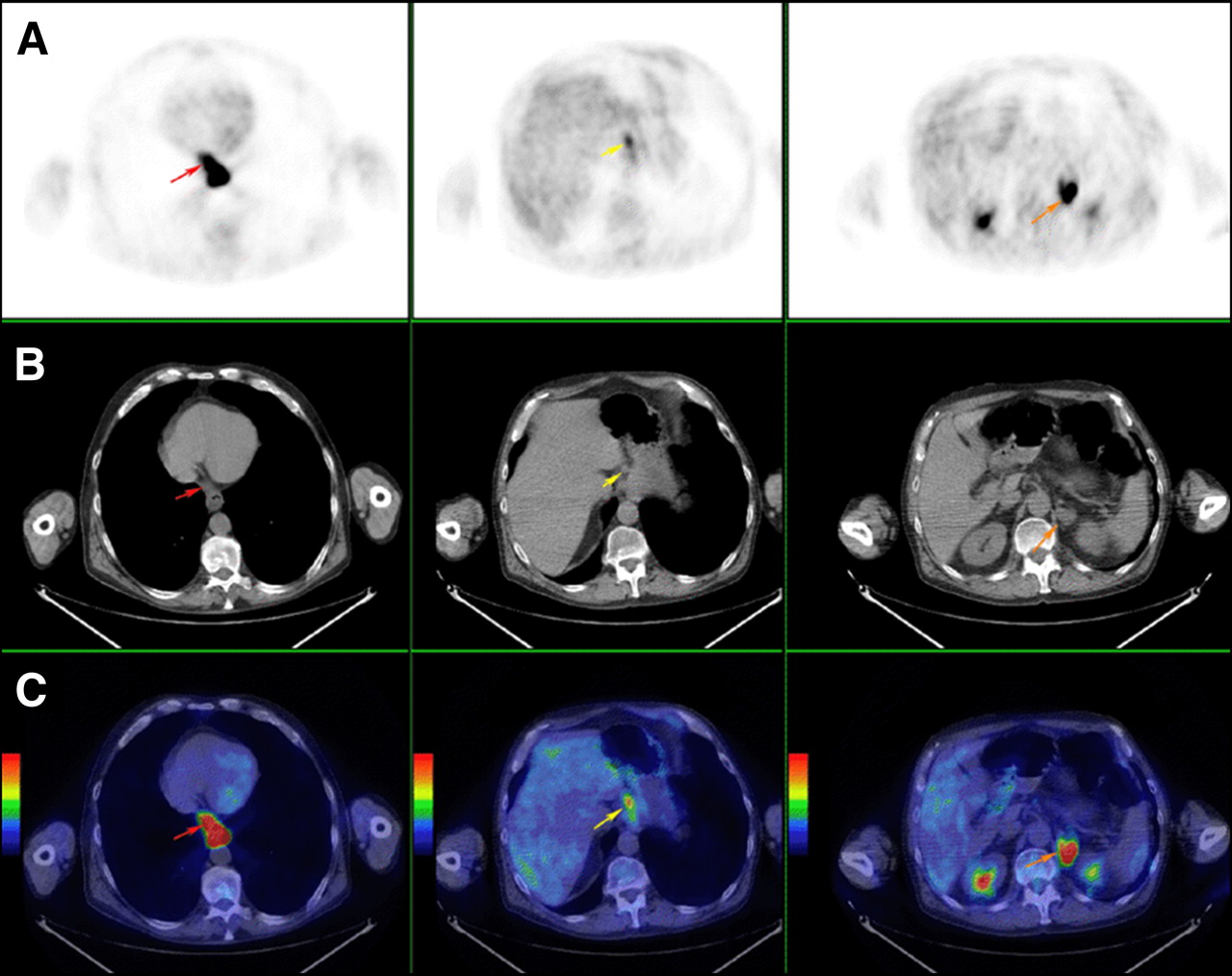
Illustration of management impact of PET/CT.
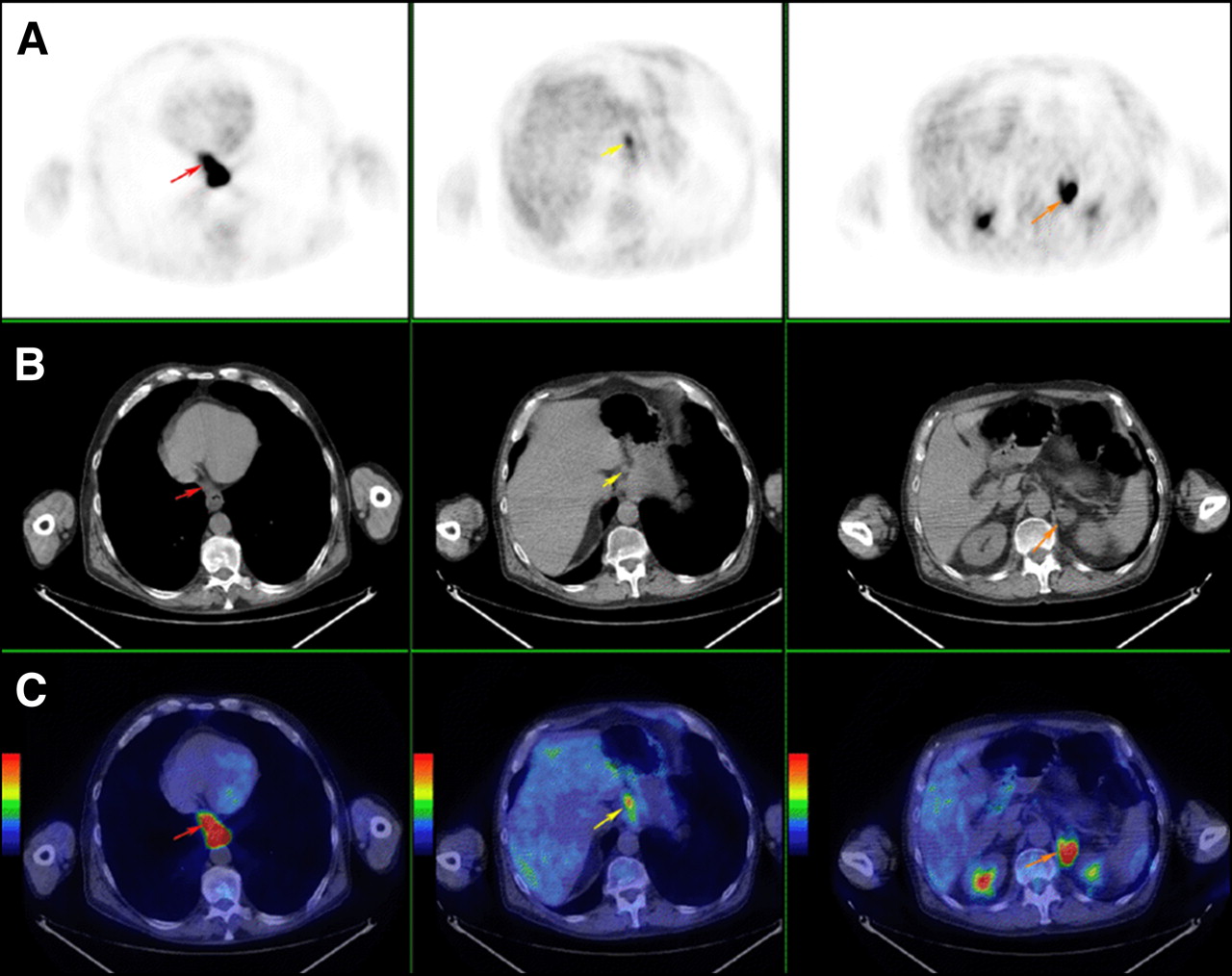
PET (A), coregistered CT (B), and fused PET/CT (C) images in patient undergoing primary staging for a lower esophageal cancer. PET/CT demonstrated intense 18F-FDG activity in the primary tumor and metastatic nodal disease in a periesophageal (red arrows) and a left gastric node (yellow arrows), which were not considered pathologically enlarged on prior staging dedicated CT. A left adrenal lesion was of indeterminate etiology on CT but was intensely 18F-FDG–avid compatible with a distant metastasis (orange arrows). Planned curative surgery was avoided and the patient received palliative treatment. The left adrenal metastasis was confirmed by progressive enlargement on serial imaging.
PET/CT had a low impact in 90 patients (65%) whose treatment was not changed on the basis of PET/CT results, predominantly because of concordance with CSI. Two patients were classified as no impact, with PET/CT results being ignored in management decisions. In one of these patients, PET/CT detected an occult liver metastasis, which was initially ignored by treating clinicians but was later confirmed on serial imaging. In the other no-impact scan, the PET/CT result was ignored because there was no increased metabolic activity in the primary tumor or nodal metastatic disease seen on CSI.
Actual Management
The actual management received corresponded to the post-PET/CT planned management in 117 of 139 patients (84%). Of the remaining 22 patients, 17 did not complete planned curative surgery, predominantly because of unresectable disease evident intraoperatively or interval disease progression following neoadjuvant therapy. The remaining 5 patients had nonsurgical management plans altered, predominantly because of an intervening change in clinical assessment.
Prediction of Survival by CSI and PET/CT
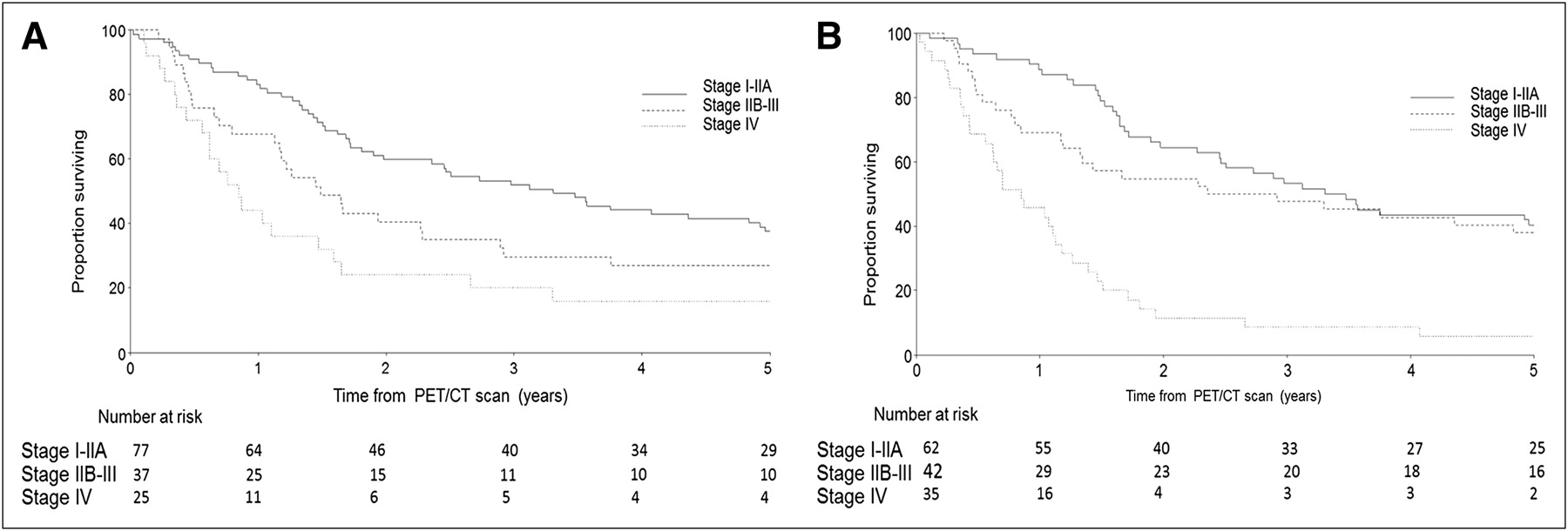
The median survival of the cohort was 23 mo. Both CSI and PET/CT were able to provide prognostic stratification with separation of survival curves according to stage group (Fig. 3), although there was convergence of survival curves in the PET/CT I–IIA and IIB–III stage groups toward the conclusion of follow-up. The trend across the survival curves was statistically significant for both CSI (P = 0.002) and PET/CT (P < 0.001). The 2-y survival rate for stage IV patients was 24% for CSI stage and 11% for PET/CT stage. The 5-y survival of patients with PET/CT stage IV disease was 6%, representing 2 patients: 1 patient with distant nodal disease successfully resected and 1 patient with a false-positive pulmonary metastasis on PET/CT confirmed to be benign on biopsy before curative surgery. No patient planned for palliative treatment after PET/CT was alive at 5 y, whereas the 5-y survival of patients planned for curative treatment after PET/CT was 38% (Fig. 4).
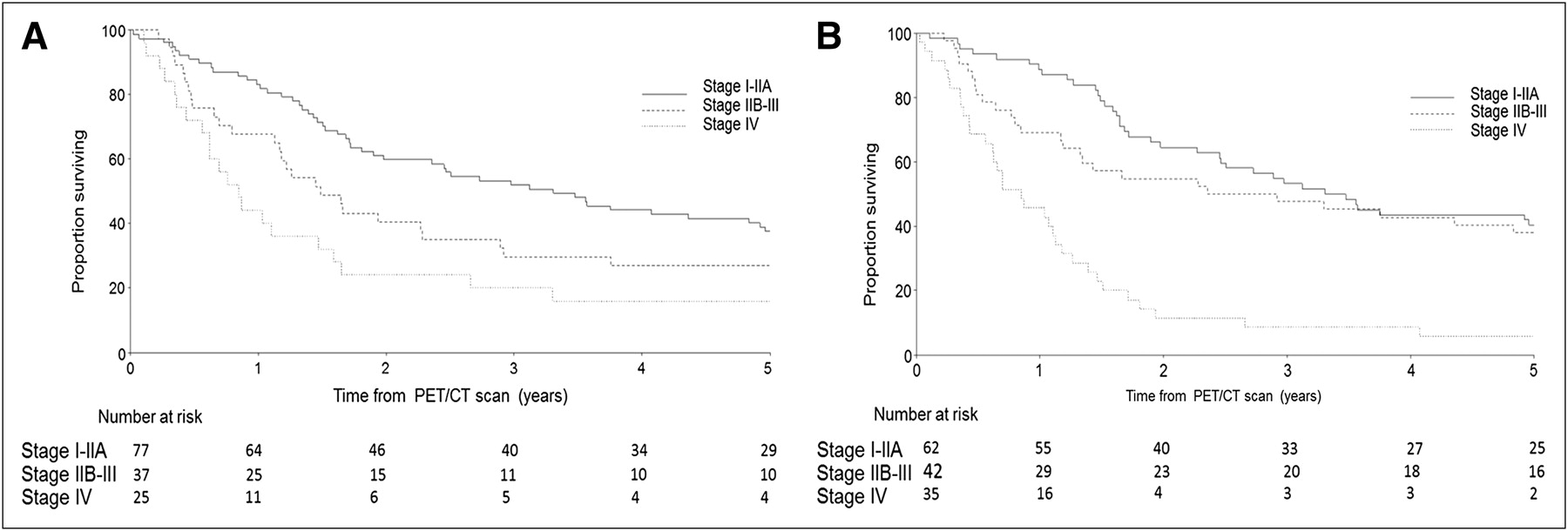
Overall survival of stage groups based on CSI (A) and PET/CT (B) results.
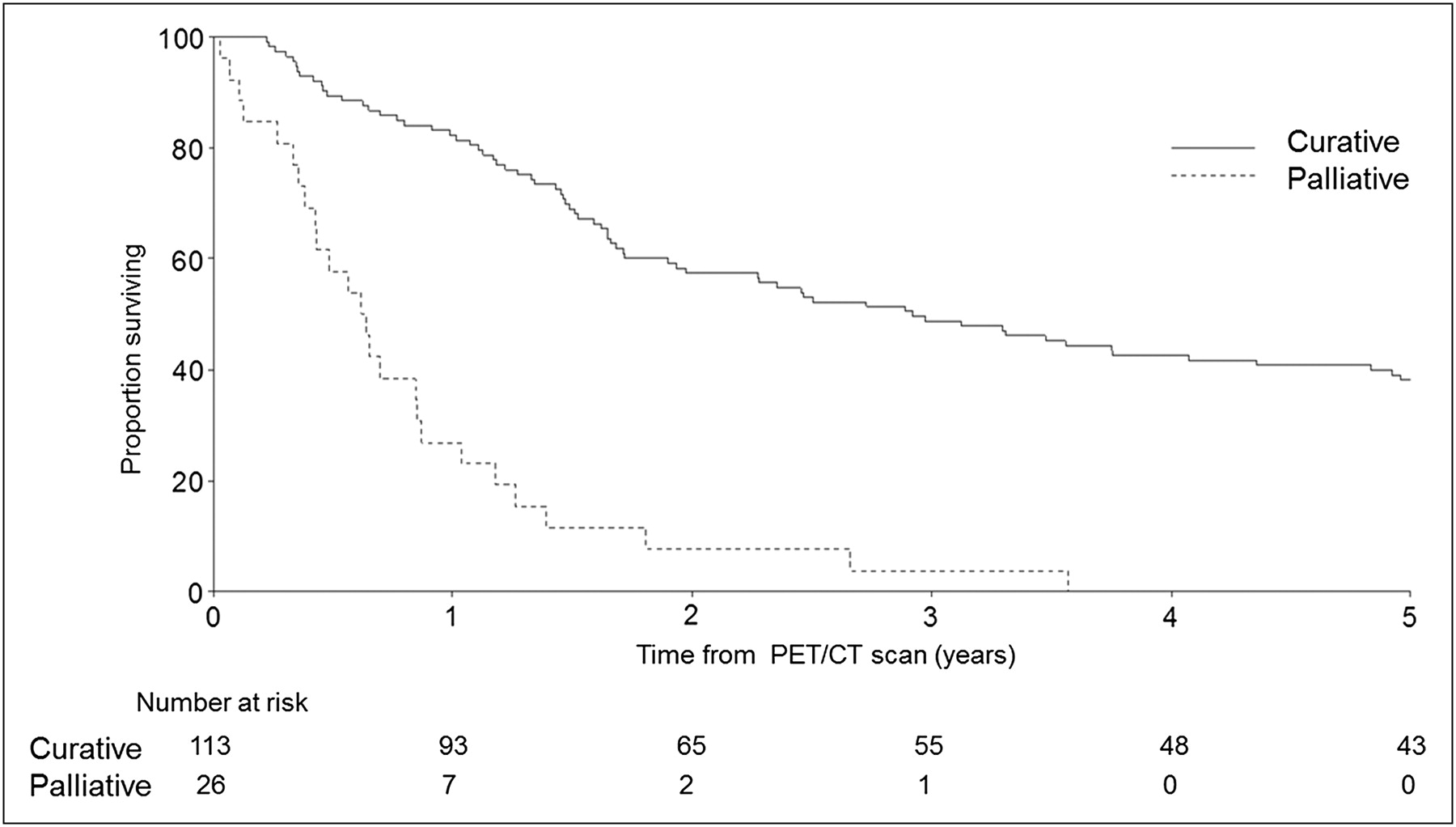
Overall survival based on post-PET/CT planned treatment intent.
The univariate analysis using the Cox proportional hazards regression model demonstrated that CSI stage IV patients had an estimated 2.5-fold higher hazard of death than CSI stage I–IIA patients. This is compared with PET/CT stage IV patients having an estimated 3.9-fold higher hazard of death than PET/CT stage I–IIA patients (Table 3). After incorporating PET/CT findings into the treatment plan, 113 patients were planned for curative treatment and 26 patients were planned for palliative treatment. The post-PET/CT planned treatment intent was highly predictive of survival (P < 0.001). The hazard rate for palliative patients compared with curative was 5.4 (95% confidence interval, 3.3–8.7) (Table 3).
Overall Survival According to CSI and PET/CT Stage Groups
DISCUSSION
In contrast to CSI, which predominantly relies on anatomic criteria for diagnosis, PET visualizes sites of malignant disease by detecting their intrinsically elevated metabolic requirements. This functional assessment of cancer with PET provides several advantages over morphologic assessment with CSI in a wide variety of cancers, including more accurate staging. This advantage is particularly true in esophageal cancer, with PET, compared with CSI, providing superior assessment of remote nodal and systemic metastatic disease (5–8,10–14). Such lesions are important to both treatment choice and delivery, with their detection contributing significantly to the observed rate of PET-induced management change in more than one third of patients (4,6). By combining both functional and anatomic information, fused PET/CT, compared with PET alone, has been shown by several authors to further improve accuracy, particularly in the assessment of nodal metastatic disease (15,17,20,21,23). Our results confirm the high utility of PET/CT in the primary staging of esophageal cancer, with alteration in stage group in 40% and a change in management in 34% of patients. Furthermore, our results demonstrate that this change in management is based on correct staging in the majority of the patients.
In this study, validation of imaging findings was limited to discordant PET/CT and CSI stage groups and to those for whom PET/CT changed management. Furthermore, EUS was performed on selected patients and was guided only by clinical need. Although this approach limits formal conclusions regarding the sensitivity and specificity of PET/CT and CSI, validation of discordant imaging findings, such as remote nodal or systemic metastatic disease (which are unable to be assessed by EUS), and those findings that result in management change is significantly more relevant to clinical decision making. This point is well illustrated by several patients in this cohort having discordant (and correct) PET/CT assessment of remote nodal or systemic metastatic disease, which appropriately changed management despite false-negative PET/CT assessment of low-volume periesophageal nodal disease. The clinical significance of false-negative nodal assessment is, however, expected to be less when these nodes are in a peritumoral location because such nodes are likely to be resected with the primary tumor or included in the radiation treatment volume. Although some studies have also revealed a moderate rate of false-negative nodes on PET/CT (17,26), this is to be expected when any imaging modality is compared with detailed histologic evaluation, which can detect even microscopic nodal deposits. CSI has similar limitations. Despite this potential limitation of PET, recent evidence suggests that patients with PET-detected nodal metastatic disease have a worse prognosis than those whose nodal disease is undetectable on PET, suggesting that the PET N stage may be an appropriate parameter in directing patients to more aggressive preoperative treatment (27). For patients with early lymph node–negative disease, our results suggest PET/CT can upstage 40% of this group. This result needs to be interpreted with caution, however, and may not apply to patients with early T1 tumors given the known limitations of PET in the assessment of the primary tumor (9) and the probable selection bias in our series. with small or superficial tumors being less likely to be referred for staging with PET/CT. In addition, some gastroesophageal junction tumors may be non–18F-FDG-avid, possibly limiting the utility of PET/CT evaluation in this group (28).
We have shown that PET/CT provides powerful prognostic stratification of esophageal cancer, with these results extending the findings of our prior study out to 5 y. Interestingly, despite initial separation, there was convergence of survival curves of PET/CT stage I–IIA and stage IIB–III patients toward the conclusion of follow-up. This convergence likely reflects more aggressive treatment allocated to stage IIB–III patients than to patients with less advanced disease, resulting in comparable 5-y survival. Furthermore, the 5-y survival of patients with PET/CT stage IIB–III disease was 38% in our study, which is superior to that previously reported by other groups (9%–34% for stage IIB and 6%–16% for stage III) (1,29,30). It is also substantially superior even when compared with the reported relative survival rate for patients diagnosed with nodal disease in the Surveillance Epidemiology and End Results database (18.4%) (2). Given that there were few false-positive PET/CT findings, this phenomenon likely reflects more accurate staging and direction to appropriate (and possibly more aggressive) treatment after incorporation of PET/CT results into patient management algorithms. This hypothesis is supported by our previously published data showing that integrating 18F-FDG PET into the staging process significantly improves radiotherapy treatment planning (31).
We chose to assess the prognostic stratification of PET/CT based on the qualitative assessment of disease stage group rather than on additional quantitative parameters. This decision is justified, in view of reports that the semiquantitative parameter maximum standardized uptake value may be of limited usefulness in the assessment of prognosis (4,32,33), although studies are conflicting in this regard (34,35). Interestingly, recent evidence suggests that other quantitative PET parameters incorporating tumor size and total lesion glycolysis may be significant prognostic indicators for overall survival (32), which may be of interest in future studies.
Limitations of this study include that CSI were not standardized but were adapted on the basis of endoscopic findings and other clinical features. This does, however, reflect typical clinical practice and accordingly we believe that this nonstandardization does not detract from our results. Another limitation inherent with this study design is that clinicians’ stated pre-PET/CT management plans may have differed from what their actual management would have been had PET/CT been unavailable to assist their decision. Nevertheless, review of the pre-PET management plans was primarily concordant with institutional treatment policies based on the assumed stage of disease on CSI. Furthermore, when actual treatment was inconsistent with the findings on PET/CT, there was usually a cogent reason for this. Finally, our study used the sixth edition of the American Joint Committee on Cancer staging system rather than the seventh edition (36), which has been in clinical use since 2010. In the new seventh edition, the N stage has been subclassified on the basis of the number of positive regional lymph nodes rather than nodal location, and the stage IVA (M1a) disease category has been removed. The new staging system is most pertinent to patients undergoing surgery and is difficult, if not impossible, to apply in patients undergoing chemoradiation without nodal sampling. Accordingly, whereas application of the new staging system may have altered the stage category of some patients in our cohort, our results remain highly relevant to the therapeutic choices pertinent to multidisciplinary care of esophageal cancer. In particular, the detection of remote nodal disease that may otherwise have been excluded from the radiation treatment volume, or the demonstration of previously occult systemic metastases rendering patients incurable by surgery or radiotherapy, is likely to more directly influence management and outcome than is counting the number of nodes involved in a resected surgical specimen.
CONCLUSION
PET/CT provides incremental staging information, changes management in one third of patients and has powerful prognostic stratification in the primary staging of esophageal cancer. PET/CT should be incorporated in routine clinical practice for the primary staging of patients with esophageal cancer. The relatively high survival of patients with locally advanced disease on PET/CT indicates that these patients may have benefitted from more aggressive and more appropriately planned multimodality treatment.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online May 11, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication December 5, 2011.
- Accepted for publication January 31, 2012.




{kind=link}
{kind=link}
{kind=link}
{kind=link}