


Abstract
Megalin-mediated renal retention of radiolabeled somatostatin analogs may lead to nephrotoxicity during peptide receptor radionuclide therapy (PRRT). The cytoprotective agent amifostine protected rats from long-term nephrotoxicity after PRRT with 177Lu-DOTA,Tyr3-octreotate. This study describes the direct effect of amifostine on kidney and tumor uptake of 111In-DOTA,Tyr3-octreotate. Methods: In vivo biodistribution studies were performed using CA20948 tumor–bearing rats, with or without amifostine coadministration, via several routes. In vitro uptake was studied in somatostatin receptor–expressing CA20948 and megalin or cubilin receptor–expressing BN-16 cells, in the absence or presence of amifostine or its active metabolite WR-1065. Results: Coadministration of amifostine decreased renal uptake of radiolabeled octreotate in vivo, whereas tumor uptake was not affected. In agreement, amifostine and WR-1065 coincubation reduced uptake in BN-16 but not in CA20948 cells. Conclusion: Amifostine may provide renal protection during PRRT using somatostatin analogs, both by mitigation of radiation damage and the currently observed reduction of absorbed kidney radiation dose.
Patients with metastasized somatostatin receptor–overexpressing tumors can benefit significantly from peptide receptor radionuclide therapy (PRRT) using 177Lu- or 90Y-labeled somatostatin analogs, for example, Tyr3-octreotate (1). However, megalin receptor–mediated reabsorption of radiopeptides in the renal proximal tubules may lead to long-term renal damage (2). Renoprotection by coinfusion of the cationic amino acids lysine and arginine is commonly applied, reducing renal uptake of radiolabeled somatostatin analogs by 40% (2,3). Kidney protection may also be achieved by mitigation of radiation-induced tissue damage by radioprotective drugs such as amifostine (3).
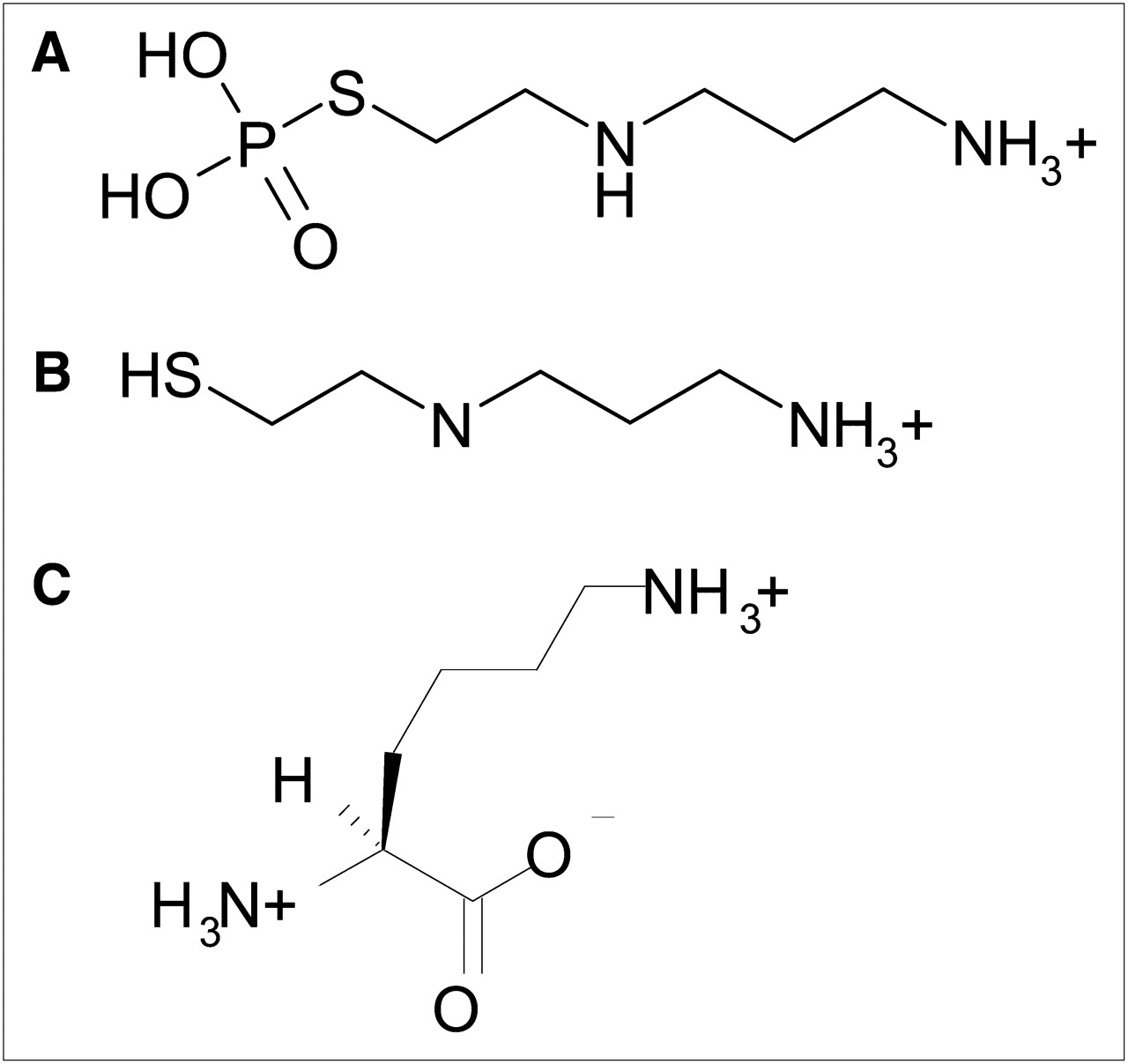
The radical scavenger amifostine (Ethyol, WR-2721; MedImmune Oncology, Inc.) was developed by the Walter Reed Army Institute of Research as a radioprotective drug in case of nuclear war. It is approved by the Food and Drug Administration for application during radiotherapy (4) and chemotherapy (5) to protect healthy tissues such as kidneys, salivary glands, and bone marrow progenitor cells (6). Scavenging of free oxygen radicals was reported as a mechanism of action (4). Amifostine is converted into its active compound WR-1065 after dephosphorylation by alkaline phosphatase, which is present in, for example, arteriolar endothelium of various normal tissues and proximal tubular epithelium in the kidney (7). The molecular structures of amifostine and WR-1065 are shown in Figure 1, demonstrating structural resemblance with lysine at the N-terminal end.

Molecular structures of amifostine, WR-1065, and lysine. (A) Amifostine = WR-2721 = C5H15N2O3PS = H2N-(CH2)3-NH-(CH2)2-S-PO3H2; molecular weight = 214.2. (B) WR-1065 = C5H14N2S = H2N-(CH2)3-NH-(CH2)2-SH; molecular weight = 134.3. (C) Lysine = C6H14N2O2 = H2N-(CH2)4-CH(NH2)-COOH; molecular weight = 142.2.
Intraperitoneal administration of amifostine protected rat kidneys from fibrosis and tubular atrophy beyond 150 d after external-beam irradiation (8). We previously reported that intravenous coadministration of amifostine, followed by 7 daily subcutaneous injections, also protected kidneys from long-term toxicity after internal irradiation by 177Lu-DOTA,Tyr3-octreotate (3). Non–tumor-bearing rats were studied; therefore, potential tumor protection against therapeutic effects of PRRT by amifostine could not be examined. The conversion of amifostine into WR-1065 is much higher in normal than in tumor tissues, because in normal tissues alkaline phosphatase activity in capillaries is high whereas in tumor tissues vascularization is abnormal, with low expression of alkaline phosphatase and a relatively low pH (9). Hence, attenuation of tumor therapy by amifostine is not expected; however, preclinical reports are ambiguous on this issue (9–11).
In the current study, we aimed to gain more insight into the renal protection mechanism of amifostine. In addition, we studied potential tumor protection by amifostine—that is, interference with tumor uptake of radiolabeled octreotate, both in vivo and in vitro. Amifostine was coadministered intravenously or subcutaneously with 111In-DOTA,Tyr3-octreotate to somatostatin receptor (sst)–expressing CA20948 tumor–bearing rats, routes also applied in patients. Uptake of 111In-DOTA,Tyr3-octreotate in the presence of amifostine and WR-1065 was examined in CA20948 and BN-16 cells, with BN-16 cells as a model for renal uptake because of megalin expression.
MATERIALS AND METHODS
Radionuclides, Peptide, and Chemicals
111InCl3 was purchased from Covidien. DOTA,Tyr3-octreotate and octreotide were supplied by BioSynthema. Radiolabeling of 111In-DOTA,Tyr3-octreotate was performed as described (12) at a specific activity of 50–80 MBq/μg for in vitro experiments and at 3 MBq/15 μg or 3 MBq/0.5 μg for in vivo studies.
Human serum albumin (HSA) kits (Vasculocis) were purchased from IBA Molecular Benelux and labeled with 99mTc (10 MBq/2 mg/mL).
Amifostine (Ethyol) was purchased from Pinnacle Biologics; 500-mg vials were reconstituted in 9.7 mL of saline. WR-1065 was kindly provided by the Drug Synthesis and Chemistry Branch, Division of Cancer Treatment, National Institutes of Health. l-lysine and bovine serum albumin (BSA) were obtained from Sigma.
Animal Experiments
Animal studies were conducted in accordance with the guidelines of the Animal Welfare Committee at Erasmus MC. Male Lewis rats were purchased from Harlan.
Two weeks after subcutaneous inoculation of approximately 106 CA20948 tumor cells in both flanks of the rats, biodistribution studies were performed in 6 groups of 4 animals. Four groups received 15 μg and 2 groups 0.5 μg of 111In-DOTA,Tyr3-octreotate intravenously via the penis vein. Amifostine (50 mg, ∼200 mg/kg) or saline was administered 30 min before radiolabeled octreotate (preinjection) or immediately before radiolabeled octreotate via 2 routes: intravenously via the tail vein or subcutaneously (coinjection). After 24 h, tumors, kidneys, and other organs were collected, weighed, and counted for radioactivity. Uptake was expressed as percentage of injected activity per gram of tissue. Results obtained for amifostine-treated rats were expressed as percentage of data obtained in control rats.
In Vitro BN-16 and CA20948 Cell Assays
Rat yolk sac carcinoma epithelial (BN-16) cells were kindly provided by Prof. Pierre J. Verroust, Department of Anatomy, University of Aarhus, Denmark (13). Uptake of 3⋅10−3 M 99mTc-HSA was determined after 1-h incubation to verify megalin expression, as previously described (14). Then, uptake of 10−9 M 111In-DOTA,Tyr3-octreotate in both BN-16 (megalin+, sst−) and CA20948 (megalin−, sst+) cells was tested, without or with addition of 10−4 M, 10−3 M, or 10−2 M amifostine, WR-1065, or lysine. An excess of BSA (10 mg/well) or octreotide (10−5M) was added as a specificity control. Uptake was expressed as percentage of added activity per milligram of cellular protein (%A/mg). Control values were set at 100%, and results of coincubation with the different agents were expressed as a percentage thereof. At least 2 experiments were performed in triplicate.
Statistics
Data were expressed as mean ± SD. Statistical analyses were performed using a Student t test. Values of P less than 0.05 were considered to be significantly different.
RESULTS
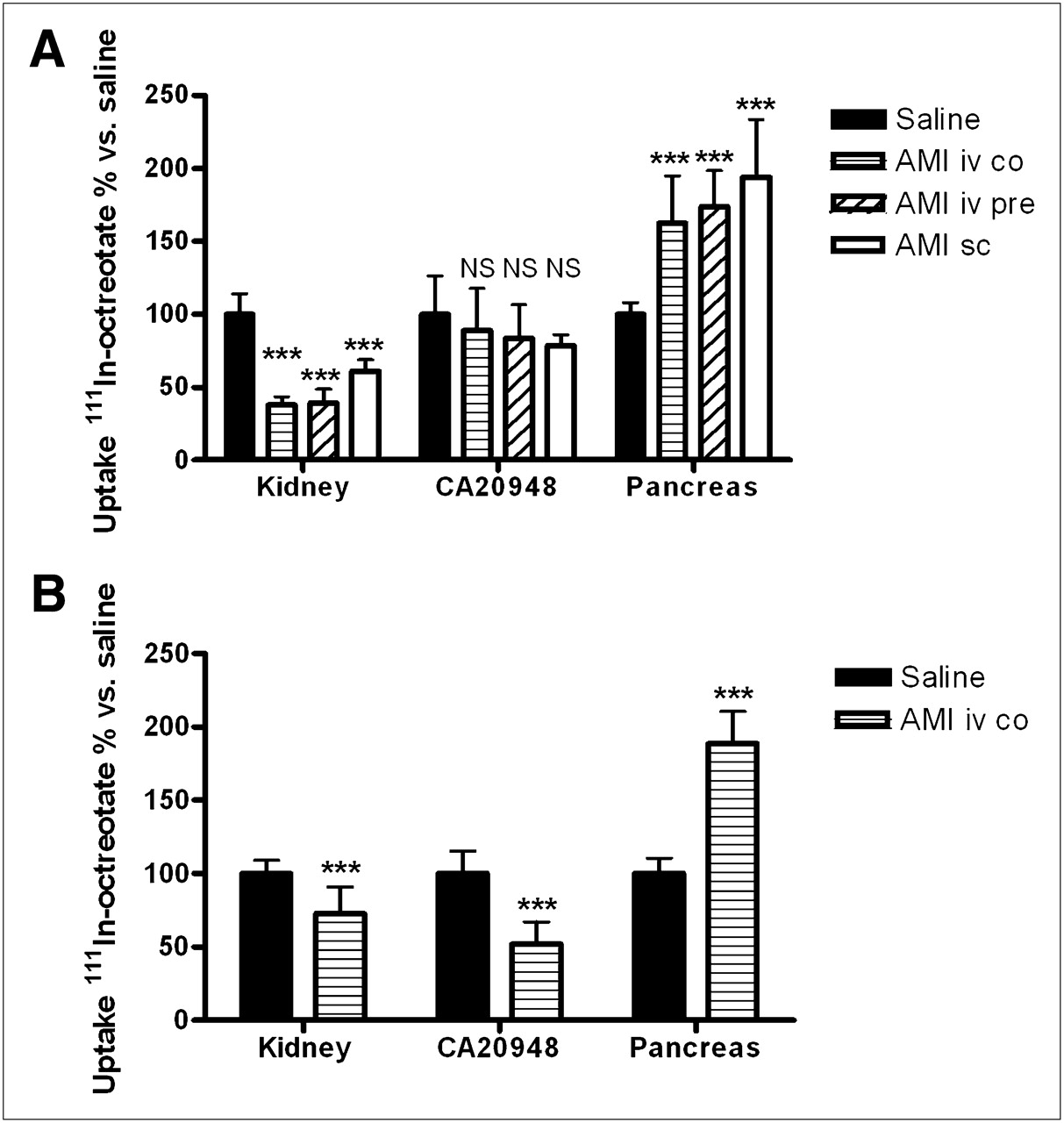
111In-DOTA,Tyr3-octreotate biodistribution was studied with 0.5 and 15 μg of peptide, to simulate diagnostic and therapeutic application of radiolabeled octreotate. To label the therapeutic dose of 555 MBq of 177Lu for PRRT in rats (3), 15 μg of DOTA,Tyr3-octreotate is required, whereas 0.5 μg of peptide leads to optimal uptake in sst-expressing tissues (Table 1) (15). The effects of coadministration of amifostine were primarily examined using 15 μg of 111In-DOTA,Tyr3-octreotate, applying 3 methods of administration (Fig. 2). A 39% reduction of the renal retention of 111In-DOTA,Tyr3-octreotate was found using subcutaneous injection of amifostine, whereas intravenous co- or preinjection of amifostine resulted in 62% and 61% reduction of renal retention, respectively. On the other hand, intravenous coinjection of amifostine with only 0.5 μg of 111In-DOTA,Tyr3-octreotate resulted in a mere renal uptake reduction of 27%. Concerning sst-mediated uptake, amifostine coadministration with 15 μg of 111In-DOTA,Tyr3-octreotate caused no significant effect on CA20948 uptake of 111In-DOTA,Tyr3-octreotate, but an almost 2-fold increase of radioactivity in the pancreas, adrenals, and stomach was detected. This latter phenomenon was also found using 0.5 μg of peptide 111In-DOTA,Tyr3-octreotate, but in this case a 48% reduction of tumor uptake was encountered.
Biodistribution of 111In-DOTA,Tyr3-Octreotate in CA20948 Tumor–Bearing Rats at 24 Hours After Injection (n = 4)

Biodistribution of 15 μg (A) or 0.5 μg (B) of 111In-DOTA,Tyr3-octreotate (3 MBq) in CA20948 tumor–bearing rats with coadministration of saline or amifostine (200 mg/kg) via different routes of injection at 24 h after administration (n = 4). Uptake was calculated as percentage of injected activity per gram of tissue, and value of the saline group was set at 100%. Uptake values obtained in amifostine groups were expressed as percentage of control values ± SD. ***P < 0.0001 vs. saline group. Differences between renal uptake using 15 μg of 111In-DOTA,Tyr3-octreotate in amifostine sc group vs. amifostine iv co and amifostine iv pre were significantly different as well (P < 0.0001 and P = 0.0002, respectively). AMI iv co = intravenous coinjection of amifostine with 111In-DOTA,Tyr3-octreotate; amifostine iv pre = intravenous injection of amifostine 30 min before 111In-DOTA,Tyr3-octreotate; amifostine sc = subcutaneous injection of amifostine immediately before 111In-DOTA,Tyr3-octreotate; NS = not significant.
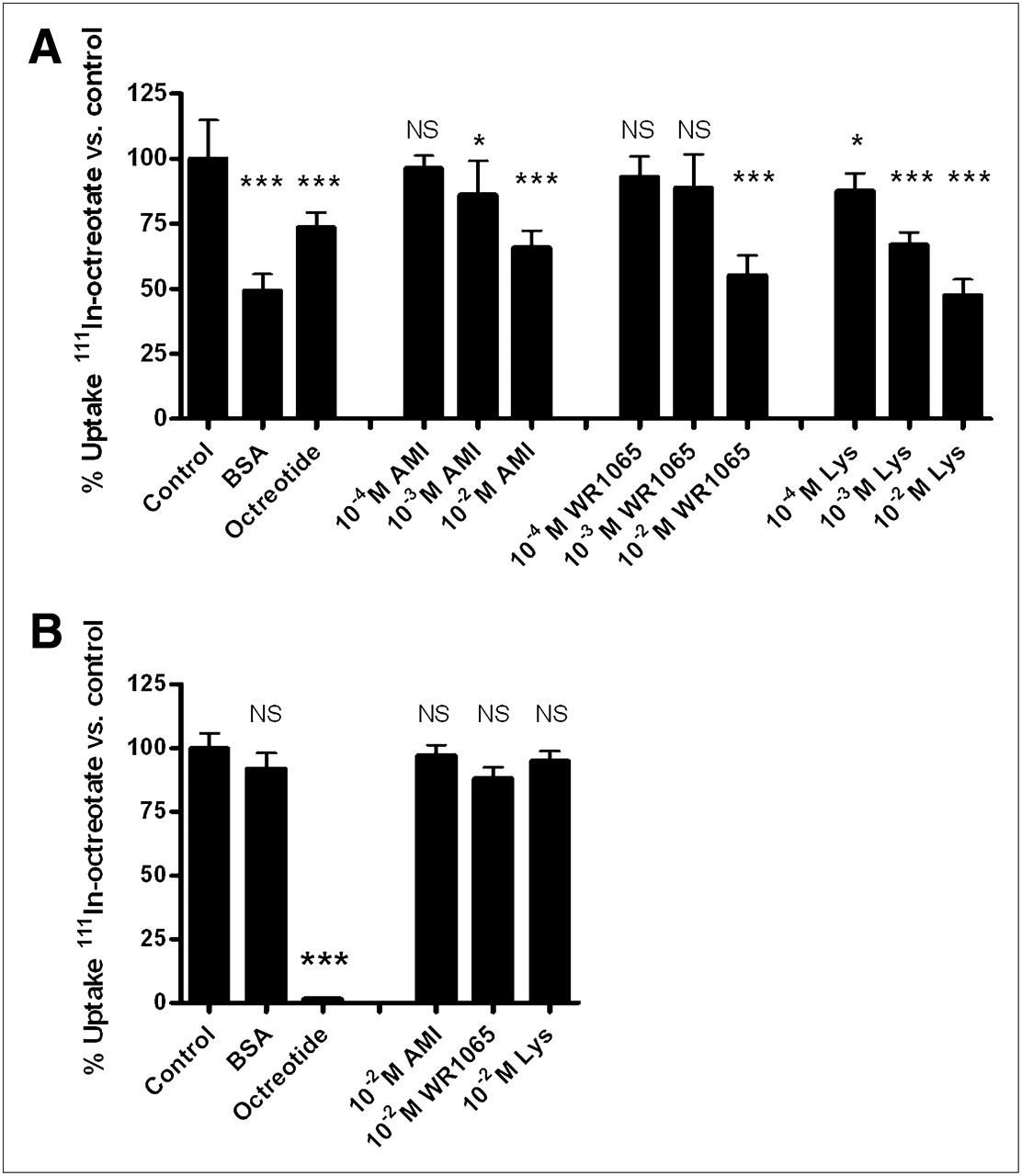
Next, in vitro studies were performed using BN-16 cells in which a specific 99mTc-HSA uptake of 20.6 ± 1.2%A/mg confirmed high megalin expression (data not shown). Uptake of 111In-DOTA,Tyr3-octreotate was 0.7 ± 0.1 in BN-16 cells and 13.5 ± 0.8%A/mg in sst2-positive CA20948 cells. This uptake could be inhibited by an excess of BSA or octreotide, respectively (Fig. 3). Moreover, a significant inhibition of 111In-DOTA,Tyr3-octreotate uptake in BN-16 cells was exerted in a dose-dependent way by WR-1065 (to 55.0% ± 7.8%) and amifostine (to 65.9% ± 6.3%) using 10−2 M, comparable to the inhibitory effects of 10−2 M lysine and BSA. No significant competitive effects of amifostine or WR-1065 on 111In-DOTA,Tyr3-octreotate uptake were found in CA20948 cells.

In vitro uptake of 10−9 M 111In-DOTA,Tyr3-octreotate in megalin-expressing BN-16 cells (A) or sst-expressing CA20948 cells (B), without or with addition of (10−4 M, 10−3 M or) 10−2 M amifostine, WR-1065, or lysine. Ten milligrams per well of BSA or 10−5 M octreotide were added as specificity controls to BN-16 and CA20948 cells, respectively. Control values were set at 100%, and effects of coincubation with different agents were expressed as percentage vs. control values ± SD. *P < 0.05. ***P < 0.0001 vs. control. AMI = amifostine; Lys = lysine; NS = not significant.
DISCUSSION
Previously, we described the ability of amifostine to protect rat kidneys from radiation damage after a 35- to 70-Gy absorbed radiation dose to the kidneys induced by 177Lu-DOTA,Tyr3-octreotate (3). Mitigation of radiation-induced nephrotoxicity seemed to be reached by sustaining a protective level of the active amifostine metabolite WR-1065 in the kidneys during the first week after therapy (9). Besides this radioprotective effect, we now speculate that, in addition, WR-1065 could act as a competitor in the charge-dependent megalin-mediated renal reabsorption of radiolabeled octreotate. Our theory is based on the currently identified reduction of uptake of 111In-DOTA,Tyr3-octreotate in rat kidneys in vivo and in BN-16 cells in vitro in the presence of amifostine or WR-1065. This phenomenon is also known for the positively charged lysine, which resembles WR-1065 at the N-terminal end (2,3).
Administered amifostine is rapidly cleared from the blood; within 6–30 min only 6%–10% of the drug remains, whereas after 5–10 min the maximum levels of WR-1065 are reached in the liver and kidneys (10,16). This peak of WR-1065 occurs later after subcutaneous than after intravenous administration of amifostine (16), possibly explaining the lower level of reduction of renal uptake we found after subcutaneous administration. In the literature, initially the intravenous route was recommended for amifostine, but the need for exact timing, transient hypotension occurring in approximately 50% of cases, and side effects such as nausea and vomiting complicated incorporation into clinical practice (17). The more easily applied and better-tolerated subcutaneous route appeared to result in a comparable radioprotection efficacy after external-beam irradiation (18). Likewise, in rats similar cytoprotective effects were found using intraperitoneal, intravenous, or subcutaneous administration of amifostine at 200 mg/kg before or after 6–15 Gy of irradiation (8,19).
Further improvement of kidney protection from 177Lu-DOTA,Tyr3-octreotate may be reached by the combination of lysine and amifostine, to achieve both short-term reduction of renal radioactivity and long-term renal function protection. Because either an additive or a competitive effect for megalin may occur, the examination of the optimal timing and route of administration of both agents are important.
The potential risk of undesired tumor protection by amifostine is being discussed since cotreatment was started (10). Here, we describe unaffected in vivo tumor uptake of 15 μg of 111In-DOTA,Tyr3-octreotate in rats with coadministered amifostine, which is in agreement with unaltered in vitro uptake of 111In-DOTA,Tyr3-octreotate by CA20928 tumor cells coincubated with amifostine and WR-1065. Our results fit with recent metaanalyses concluding that amifostine did not compromise the antitumor efficacy of chemotherapy and radiotherapy (4,20).
The striking observation that amifostine coadministration increased uptake of 111In-DOTA,Tyr3-octreotate in sst-expressing normal organs may partially be explained by an earlier described transient drop in systolic blood pressure induced by a bolus injection of amifostine (17). The blood pressure was not registered, but hypotension would result in a prolonged circulation time of 111In-DOTA,Tyr3-octreotate and reduced blood supply to the subcutaneously developed tumors. These effects may have led to increased uptake in, for example, the radioinsensitive pancreas but a decreased CA20948 uptake using the optimal 0.5 μg of 111In-DOTA,Tyr3-octreotate amount for high tumor uptake (15). Differences in receptor saturation and turnover rate of the receptor or peptide complex between tumors and normal tissues may be the reason for this discrepancy.
Besides kidney protection, administration of amifostine during PRRT might also accomplish radioprotection of bone marrow, the other organ at risk in patients (1,6). Thus, application of amifostine might enable a safe increase of therapeutic radiation doses by PRRT to improve cure rates of this promising therapy.
CONCLUSION
Coadministration of the cytoprotector amifostine with radiolabeled octreotate reduced its renal uptake. This effect appears to be partially based on inhibition of the megalin-mediated renal reabsorption of radiopeptides by amifostine or its active metabolite WR-1065. Interference with tumor uptake was not detected in vitro and in vivo in rats during therapeutic conditions. Therefore, amifostine may be applied to provide kidney protection during PRRT both to reduce the radiation absorbed dose to the kidney and to prevent late development of radiation-induced renal fibrosis.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
Drs. Flavio Forrer, Cristina Müller, and Edgar Rolleman contributed to fruitful discussions. Technical assistance by Dr. Monique de Visser, Linda van der Graaf, Erik de Blois, and other technicians of the Department of Nuclear Medicine, Erasmus MC, was greatly appreciated. This study was supported by the Dutch Cancer Foundation grant no. EMCR 2007-3758. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 10, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication September 26, 2011.
- Accepted for publication January 31, 2012.





{kind=link}
{kind=link}
{kind=link}